
Percutek Therapeutics
Developer of Minimally Invasive Cardiovascular Treatment Devices

Today, I will introduce to youZhang Zhang/Wang Lei Team from Tangdu Hospital, Air Force Medical UniversitySharing of TEVAR Surgery with In-situ Reconstruction of Aortic Arch Branches Using Only 0.018" CTO Guidewire Soft Tip. The patient had an aortic arch aneurysm, with a diameter expansion of 51mm located in the anterior wall of the aortic arch. The lesion extended proximally to involve the root of the left subclavian artery, leaving an insufficient proximal anchoring zone. It was necessary to extend the proximal anchoring zone and reconstruct the left subclavian artery branch. However, the distance between the left common carotid artery and the left subclavian artery was only 6mm. What surgical plan should be chosen to effectively occlude the aneurysm lesion and efficiently reconstruct the left subclavian branch while ensuring long-term prognosis? Zhang Zhang/Wang Lei's team applied the Percutek Therapeutics thoracic aortic stent graft to effectively occlude the aortic arch aneurysm lesion. They used only the 0.018" CTO guidewire soft tip and completed the reconstruction of the left subclavian artery efficiently through the in-situ fenestration technique. The patient had a good postoperative outcome.
Age:64 years old
Gender:Male
Chief Complaint:Pulmonary nodules found for over 3 years.
History of Present Illness:A left lung nodule was discovered in another hospital 3 years ago. Two days ago, a chest CT performed at another hospital due to high blood pressure indicated malignant changes in the left lung and aneurysmal dilation of the aortic arch. The patient was subsequently admitted to our hospital for further diagnosis and treatment, and was enrolled in the outpatient department with "lung mass."
Past Medical History:Previously healthy. Has a history of hypertension for over 20 years, with the highest blood pressure recorded at 180/90 mmHg. Regular medication has kept it under control. History of coronary heart disease for 6 years. Underwent cholecystectomy for gallstones at another hospital more than twenty years ago.
Preoperative Diagnosis:Aortic aneurysm, Hypertension grade 3 (very high risk), Coronary heart disease, Pulmonary mass (upper left).
Detailed Explanation of CTA:Localized aneurysm-like dilation of the aortic arch, with a diameter of approximately 51*42mm, and the proximal end has involved the root of the left subclavian artery. The left subclavian artery is tortuous, with its root located on the anterior wall of the aortic arch, forming an acute angle of only 30° with the aorta. The distance between the left common carotid artery and the left subclavian artery is only 6mm. Multiple calcified plaques, non-calcified plaques, and mixed plaques have formed in the walls of the aortic arch and descending thoracic aorta, causing mild local lumen stenosis. Central-type lung cancer with obstructive pneumonia. Calcified plaques are present in the coronary artery pathways bilaterally.

Preoperative Three-dimensional Reconstruction

Preoperative CTA Cross-Section
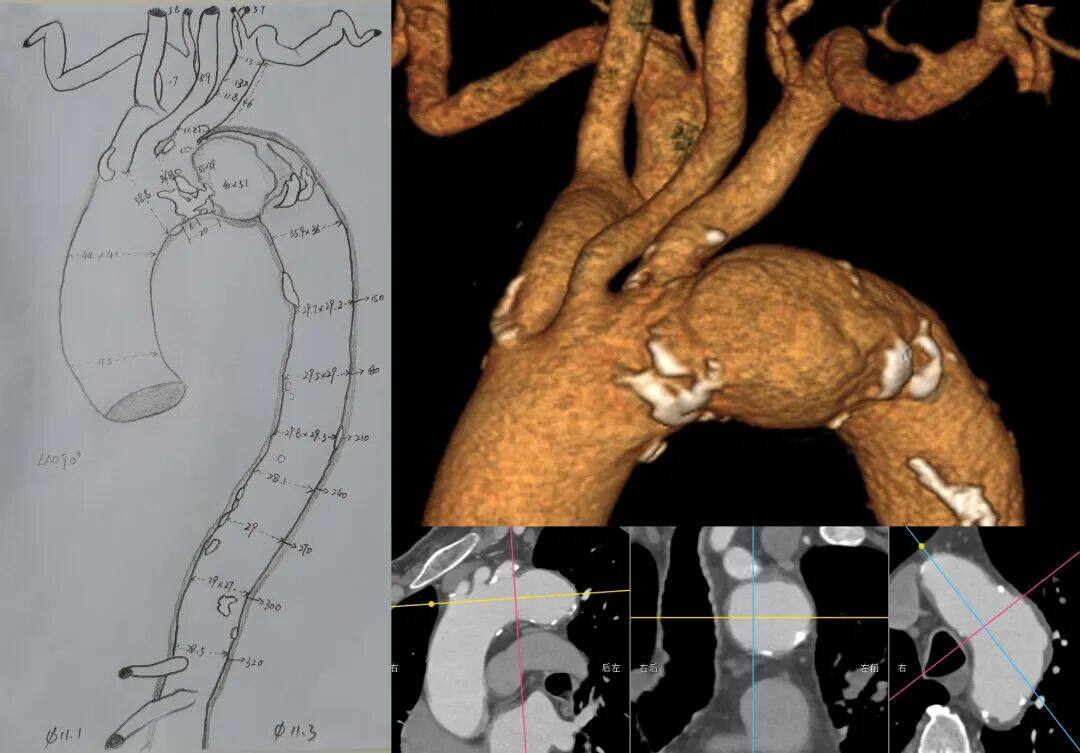
Measurement Data
Aneurysm of the aortic arch, located at the anterior wall of the arch, with the proximal end already involving the root of the left subclavian artery. The proximal anchoring zone is significantly insufficient, and the distance between the left common carotid artery and the left subclavian artery is only 6mm. It is necessary to extend the anchoring zone proximally and reconstruct the left subclavian artery.
The left subclavian artery originates from the anterior wall of the aortic arch, with tortuosity, stenosis, and angulation, forming an acute angle with the aortic arch. This presents challenges for in-situ fenestration angle control during surgery. Additionally, common covered stents on the market pose significant difficulties for fenestration.
The diameter of the aortic arch aneurysm is significantly enlarged, requiring high proximal sealing performance for the thoracic aortic stent graft.
Multiple calcifications in the aortic arch should be handled with gentle manipulation.
Surgical Plan Strategy
Endovascular Repair of Thoracic Aortic Stent Graft Directly Covering the Left Subclavian Artery:The operation is simple and the effect is clear, but covering the left subclavian artery may cause clinical manifestations of posterior circulation ischemia and upper limb ischemia in patients.
Endovascular Repair of Thoracic Aortic Stent Graft + Left Subclavian Artery Chimney Technique:The surgical procedure is relatively simple, but the left subclavian artery is tortuous and stenotic, with a high risk of endoleak and occlusion, and the mid-to-long term outcomes are suboptimal.
Endovascular Repair of Thoracic Aortic Stent Graft with In Vitro Fenestration:The closure effect of the lesion is good, which can preserve the original hemodynamic characteristics, but the operation is complex. The stent needs to be modified according to the measurement results before the surgery, which takes a long time; during the surgery, precise positioning of the ultra-selection window is required, posing higher risks.
Single-branched Stent Thoracic Endovascular Aortic Repair:The lesion closure effect is good, but the left subclavian artery is angulated, increasing the risk of branch stent occlusion in the long term.
Endovascular Repair of Thoracic Aortic Stent Graft + In-situ Fenestration:The lesion closure is effective, and there is no need to modify the stent before surgery. However, the in-situ fenestration of traditional aortic covered stents has higher requirements for interventional devices, necessitating special membrane-piercing instruments such as in-situ fenestration needles, lasers, and biopsy needles.
The proximal end of the main body of Percutek Therapeutics' thoracic aortic stent graft can be easily fenestrated in situ using only a 0.018" CTO guidewire with a soft tip. Considering the mid-to-long term treatment outcomes and the simplicity of intraoperative manipulation, after comprehensive evaluation, the Zhang Zhang/Wang Lei team chose Percutek Therapeutics' Tianyi.®Endovascular repair of the thoracic aorta with a covered stent graft and reconstruction of the left subclavian artery using in-situ fenestration technology.
Endovascular Repair of Thoracic Aortic Aneurysm + Single-Stent In-situ Fenestration
01. The patient was placed in the supine position, routinely disinfected, and covered with sterile drapes. After successful general anesthesia, the right femoral artery was punctured, and a short sheath was introduced for standby use. The left brachial artery was incised, and a guidewire was inserted through puncture. An 8.5F steerable sheath was placed, and a gold-marker pigtail angiography catheter was guided to the ascending aortic level for angiography, which showed a large aneurysm-like dilation of the aortic arch, consistent with the preoperative CT.

LAO Angiography

RAO Angiography
02. Accurately measure the aortic diameter at the distal end of the root of the left common carotid artery during the operation to determine the model of the Percutek Therapeutics thoracic aortic stent graft. Introduce the Lunderquist super-stiff guidewire through the right femoral artery, withdraw the gold-marker pigtail catheter, and deliver the Percutek thoracic aortic stent graft system. Precisely position it at the distal end of the root of the left common carotid artery, release 2-3 segments, confirm the position again, then release the entire stent and the post-release bare stent. Another angiography showed: precise stent positioning, good expansion, no angular deformity, good blood supply to the left common carotid artery, and no significant endoleak.

Implantation of Percutek Thoracic Stent

Proximal positioning at the distal root of LCCA

Slow Release 2 Sections to Confirm Position Again

Full Release Stent
03. A single-bend catheter was introduced via the left brachial artery sheath, with the tip positioned at the covered stent in the aortic arch. A 250T guidewire was inserted and used in conjunction with the single-bend catheter to successfully perform an in-situ fenestration at the root of the left subclavian artery. Hand-injected contrast confirmed that the guidewire had entered the covered stent.

Insert single-bend catheter and 250T guidewire

250T Guidewire Successfully Penetrates the Membrane at the Root of LSA
04. Sequentially dilate the fenestration using 3-30mm Sterling balloons and 8-40mm Mustang balloons, and pass through the aortic fenestration site using the balloon-with-sheath technique.

3-30mm Balloon Dilation

8-40mm Balloon Dilation
RAO Confirmation

Balloon with sheath into the membrane
05. Angiography of the left subclavian artery showed: Minimal contrast agent leakage from the left subclavian artery. A 12-58mm Lifestream balloon-expandable covered stent was implanted and deployed.

Import LifeStream Stent

Balloon-Expandable LifeStream Stent
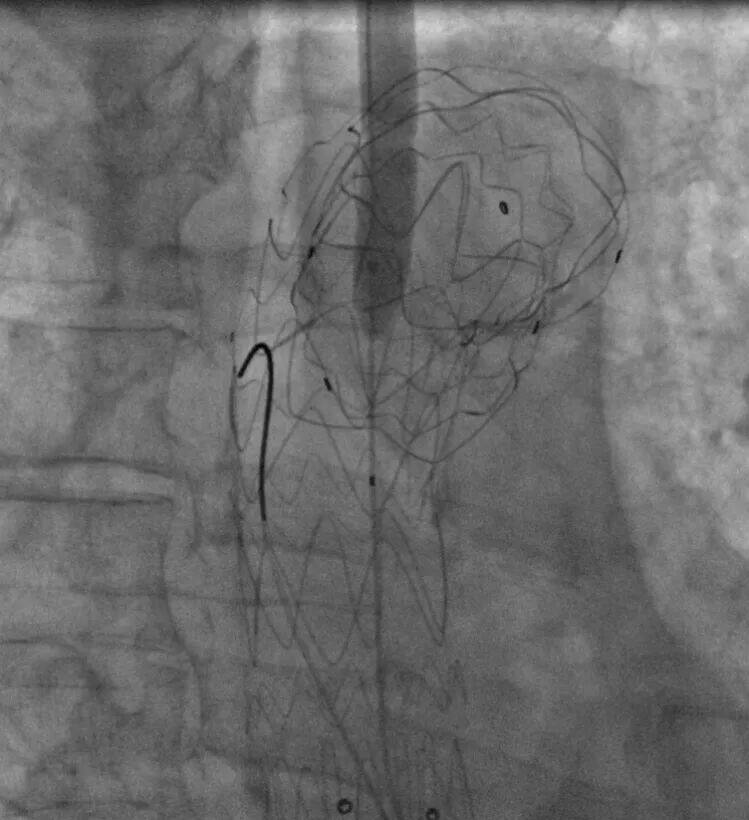
06. The final angiography showed satisfactory results, with the thoracic aortic stent in good position, smooth blood flow, no significant endoleak, good blood supply to the three branches above the arch, positive blood flow in the left subclavian artery, and good visualization of the bilateral carotid arteries, vertebral arteries, and intracranial arteries.

Angiography after LAO surgery

Angiography after RAO surgery
07. Withdraw the stent delivery system, catheters, guidewires, and other interventional treatment facilities. Inspect the left brachial artery, suture the arterial puncture site, close the surgical incision, and apply pressure dressing to the puncture site and surgical incision. The surgery is completed, achieving the expected preoperative outcome.
One-month postoperative review compared with preoperative

Preoperative/Postoperative 3D Reconstruction

Preoperative/Postoperative CTA Cross-Section
Two weeks after the surgery, the patient underwent tumor resection in the thoracic surgery department and was followed up. One month after the surgery, the复查 showed good recovery, with no signs of cerebral infarction or cerebral ischemia. The aortic arch aneurysm was completely isolated, and the branch stent was patent with a good morphology.
Summary of Case Experience
This case study involves a patient with an aortic arch aneurysm, where the lesion's proximal end has extended to the root of the left subclavian artery, leaving an insufficient proximal anchoring zone. Additionally, the distance between the left common carotid artery and the left subclavian artery is only 6mm, necessitating the extension of the proximal anchoring zone and reconstruction of the left subclavian artery. Moreover, the left subclavian artery originates from the anterior wall of the aortic arch, with tortuosity, stenosis, and angulation, forming an acute angle with the aortic arch, which presents challenges for in-situ fenestration angle control during surgery. After careful consideration of the surgical plan, including the selection of the procedure type and stent graft, the Zhang Zhang/Wang Lei team chose the Percutek Therapeutics thoracic stent graft system for this case. Using only a 0.018" 250T CTO guidewire with a soft tip, they successfully punctured the membrane, efficiently completing the supra-aortic reconstruction of the left subclavian artery. The Percutek Therapeutics thoracic aortic stent graft demonstrated precise proximal positioning, with the fenestration area being easily penetrable and expandable. The membrane could be instantly punctured using just the soft tip of the CTO guidewire. The balloon dilation process was simple, safe, and reliable, and after stent implantation, the morphology was excellent with good sealing of the lesion, no endoleak, clear outcomes, and favorable patient prognosis. Ultimately, the supra-aortic reconstruction results aligned with preoperative planning expectations.

Professor Zhang Zhang
Director of the Department of Interventional Vascular Surgery, Tangdu Hospital, Air Force Medical University; Associate Chief Physician; Doctor of Medicine; Master's Supervisor. Pioneered the completion of Sandwich technique and self-made IBD endovascular aneurysm repair in abdominal aortic aneurysms, performed the first mechanical thrombectomy in Northwest China, 3D printing-assisted fenestrated endovascular aortic stent repair, immediate puncture artificial vascular dialysis access, and other high-end surgeries in Western China. Conducted direct lymphangiography and established the first comprehensive clinic for vascular lymphatic surgery. Currently serves as Standing Committee Member of the Endovascular Society of the Chinese Medical Doctor Association, Member of the Vascular Surgery Branch of the Chinese Medical Doctor Association, Vice Chairman of the Youth Council of the Asia-Pacific Vascular Academic Alliance, Deputy Secretary General (and Standing Committee Member) of the Youth Committee of the Peripheral Vascular Disease Society of the Chinese Society of Microcirculation, Chairman of the Peripheral Vascular Branch of the Shaanxi Day Surgery Medical Association, Vice Chairman of the Endovascular Society of the Shaanxi Medical Doctor Association, Vice Chairman of the Peripheral Vascular Disease Committee of the Shaanxi Geriatrics Society, Vice Chairman of the Interventional Vascular Committee of the Shaanxi Integrated Traditional Chinese and Western Medicine Society, Vice Chairman of the Shaanxi Vascular Alliance (IUA), and Standing Committee Member of the Vascular Surgery Branch of the Shaanxi Medical Doctor Association. Presided over four research projects including the National Natural Science Foundation of China, key projects of Shaanxi Province, and military youth training programs. Published seven SCI papers in the past five years (with the highest single-article impact factor of 12.95), more than 20 core journal articles, authored three monographs, co-authored seven books, obtained 11 patents, and participated in formulating the first domestic expert consensus on mechanical thrombectomy, the first domestic expert consensus on thromboangiitis obliterans, and the 2021 expert consensus on varicose veins of the lower extremities. Currently serves as editorial board member and reviewer for core journals such as the Journal of Vascular and Endovascular Surgery, Journal of Robotic Surgery, Journal of Air Force Medical University, and Chinese Journal of Traumatology (English Edition). Awarded Third-Class Merit once in 2020 and named "Advanced Individual in Epidemic Prevention" in 2021.

Professor Wang Lei
Associate Chief Physician of the Department of Interventional Vascular Surgery at Tangdu Hospital, Air Force Medical University. Currently serves as a member of the Open Surgery Group of the Vascular Surgery Branch of the Chinese Medical Doctor Association, a member of the Vascular Surgery Professional Committee of the Shaanxi Medical Doctor Association, a member of the Endovascular Professional Committee of the Shaanxi Medical Doctor Association, a member of the Youth Academic Committee of the Asia-Pacific Vascular Academic Alliance, the Deputy Chairman of the Peripheral Vascular Branch of the Shaanxi Day Surgery Medical Association, a Standing Committee Member of the Peripheral Vascular Committee of the Shaanxi Geriatric Medical Association, and a Standing Committee Member of the Interventional Vascular Specialty Committee of the Shaanxi Integrated Traditional Chinese and Western Medicine Association, among others.

Department Introduction
Department of Interventional Vascular Surgery, Tangdu Hospital, Air Force Medical University
The Interventional Radiology Department of Tangdu Hospital was established in 1994 as the first independent interventional specialty in China. It is an authorized discipline for doctoral and master’s degrees and serves as the National Training Center for Minimally Invasive Pain Interventions, the National Training Base for Minimally Invasive Oncology Interventions, the National Peripheral Vascular Training Base, the Clinical Skills Training Center of the Pain Specialty Committee of the Chinese Association of Integrative Medicine, the Shaanxi Provincial Society of Interventional Radiology, the Anti-Cancer Society, and holds triple chair positions in the Peripheral Vascular Branch of the Day Surgery Society. It is also the Deputy Chair Unit of the Youth Committee of the Asia-Pacific Vascular Academic Alliance. The department has two wards with 65 beds and is equipped with two dedicated interventional operating rooms. It includes two large DSA units (GE Healthcare, USA), ultrasound equipment, and various monitoring and anesthesia devices. One of the operating rooms is a laminar flow hybrid operating room capable of performing various open/interventional hybrid surgeries. The department currently has 73 medical staff members, including six senior professionals, four doctoral and master’s supervisors, eight doctors with Ph.D.s, and 14 with master’s degrees, ensuring sufficient talent reserves and a well-structured personnel hierarchy.
The department has three sub-specialties: vascular surgery, pain management, and comprehensive interventional procedures. It is capable of performing interventional diagnosis and treatment for various vascular and non-vascular diseases, pain-related conditions, and complex open vascular surgeries across all parts of the body. It is a fully-equipped minimally invasive diagnosis and treatment department with qualifications in both "open surgery + intervention." In particular, its diagnostic and treatment technologies for lower extremity arterial occlusive disease, aortic dissection, deep vein thrombosis, abdominal aortic aneurysm, visceral artery diseases, TIPS for portal hypertension, tumor interventions, and cervical and lumbar disc herniation are among the leading in China. The department completes over 6,000 interventional surgeries annually, making it the largest interventional and vascular surgery center in Western China with the most comprehensive sub-specialties and the highest annual surgical volume. In recent years, the department has successfully completed more than ten internationally and domestically innovative high-end surgeries, including the world’s first "rapid minimally invasive repair of complete arterial disconnection" and the world’s first "retrograde carotid artery aortic dissection repair," filling technical gaps in the fields of interventional therapy and vascular surgery.
The department began to enroll master's degree candidates in interventional radiology in China as early as 1991. Over the years, it has trained more than 100 outstanding academic leaders in interventional-related specialties for both military and civilian sectors. The department boasts a strong research atmosphere, having secured 14 National Natural Science Foundation projects, over 20 provincial-level key research and development projects (including those from Shaanxi Province), one Ministry of Health research fund, and two collaborative research funds. It has published over 300 journal articles, more than 20 teaching papers, and over 200 SCI papers. Additionally, the department has obtained more than 40 patents, authored over 20 monographs, produced two audio-visual teaching materials for the Ministry of Health, and won one third prize for medical achievements from the military. In 2000, Professor Wang Zhimin founded the Western Interventional Radiology Conference and became the leading unit. This conference has since grown into one of the largest interventional conferences in China. In recent years, the department has hosted multiple national and military academic conferences. It has also sent many individuals to top international institutions specializing in interventional radiology, pain management, and vascular surgery to expand international academic exchanges and enhance the global influence of the discipline.

END
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints; it is solely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is intended for healthcare professionals to stay informed and should not replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and its authors shall not bear any related responsibility.Contact email for cooperation:vascular@edoctor.work。
