Drug Name/Dosage Form | Capivasertib Coated Tablets |
Specification | 160 and200mg |
Route of Administration | Oral |
Rx/OTC Classification | (Original Research)Rx |
Indications | RADENAME is used for the treatment of hormone receptor (HR) Positive, Human Epidermal Growth Factor Receptor2(HER2) Negative (defined asIHC 0Or1+, orIHC 2+/ISH-) in adult patients with locally advanced or metastatic breast cancer that has recurred or progressed after endocrine therapy. |
Applicant | AstraZeneca Pharmaceuticals LP |
Submission Date | 2023.3.28 |
Date Received | 2023.3.28 |
PDUFA Target Date | 2023.11.28 |
Review Department | Oncology Department |
Completion Time of Review | 2023.10.30 |
Common Name | Capivasertinib |
Proposed Trade Name | Trugap(capivasertib) |
Pharmacological Classification | Kinase Inhibitor |
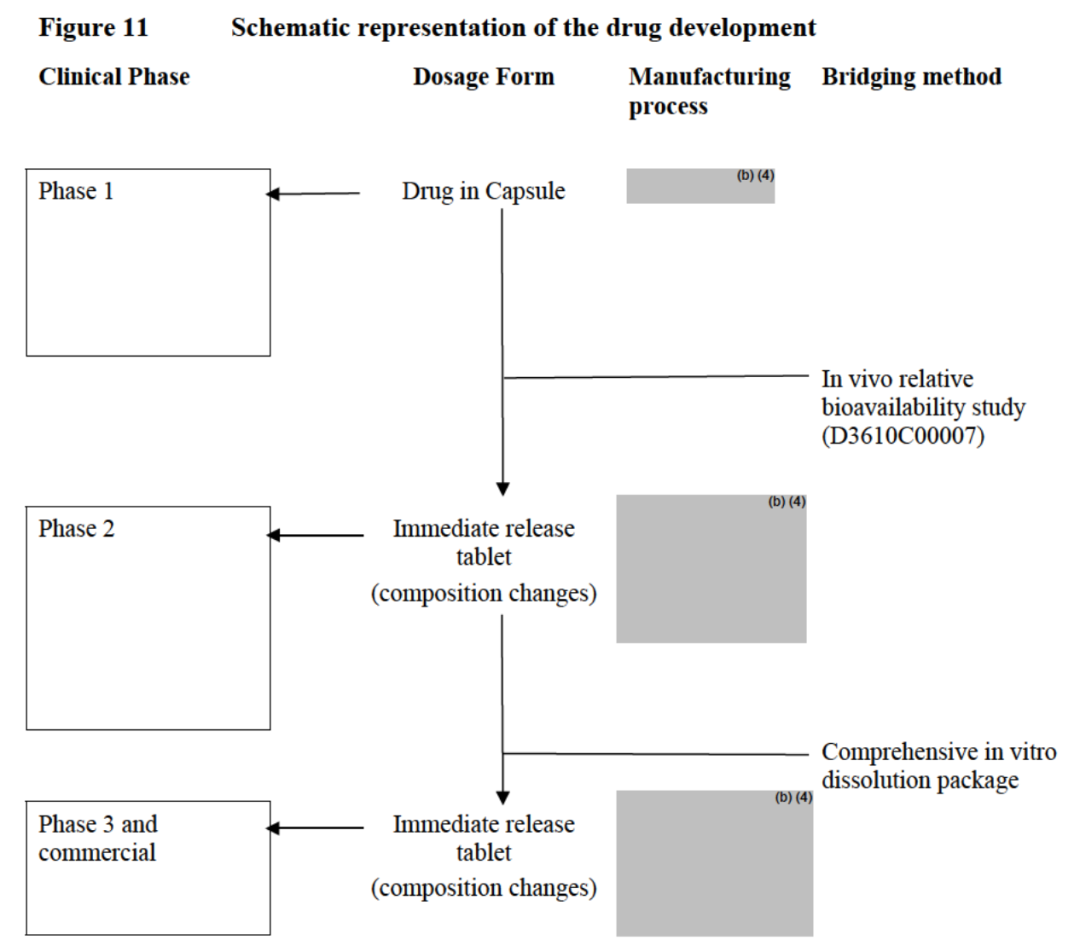
Bridging in Drug Development Phase (Changes in Formulation, Process, or Site)
During the development of the drug, three different immediate-release formulations were created:Phase 1 Clinical Capsule: For Phase I clinical studies and relative bioavailability studies (Study D3610C00007).Phase 2 Clinical Tablets: Phase 2 Clinical Study and Relative Bioavailability Study (Study D3610C00007).
Phase 3 Clinical/Commercial Tablets: Optimized tablets for Phase 3 clinical studies and food effect/PPI studies (Study D3614C00005). The commercial capivasertib tablets are identical to the Phase 3 clinical tablets in quality and quantity but are differentiated by the use of debossing. The clinical tablets are plain, while the commercial tablets are debossed, as described in section 3.2 P.1 and in the drug product components.
The production site of the Phase 3 clinical prescription is the same as the proposed commercial prescription production site.The capsule formulation in Phase 1 and the tablet formulation in Phase 2 showed significantly different in vitro dissolution behaviors. Compared with tablets, capsules exhibited a slower dissolution rate in various media.Therefore, the connection between these formulations was investigated through an in vivo relative bioavailability study (Study D3610C00007), showing comparable pharmacokinetic profiles and exposure.The results of the in vitro and in vivo bridging between the Phase 1 capsule and Phase 2 tablet showed that the in vivo exposure would not be significantly affected by the in vitro dissolution. Therefore, the slower in vitro dissolution profile exhibited by the Phase 1 capsule is considered clinically relevant and represents the "safe space" boundary for the in vitro performance of capivasertib tablets.Therefore, an alternative immediate-release formulation of capivasertib (with a faster release rate than the capsule) may have similar bioavailability to the Phase 1 clinical capsule, and similar bioavailability between them. Therefore, in vitro bridging was used to bridge between the Phase 2 clinical tablet and the Phase 3 clinical tablet.Bridging between Phase 1 capsules and Phase 2 tablets: The release rate of Phase 1 capsules in multiple media was slower compared to Phase 2 coated tablets, at pH values of 1.2, 4.5, and 6.8 (PDR, pages 22-24). Therefore, bioequivalence between Phase 1 capsules and Phase 2 tablets was bridged through in vivo relative bioavailability (PDR, page 25, Study D3610C00007).Transition between Phase 2 and Phase 3 Tablets: In terms of excipients, the composition of the Phase 3 coated tablets (PDR, page 13) is significantly different from that of the Phase 2 coated tablets (PDR, page 7).However, the in vitro and in vivo results bridging Clinical 1 Avril capsules and Clinical 2 phase tablets indicate that in vivo exposure is not significantly affected by dissolution. Therefore, the dissolution profiles in multiple media at pH 1.2, pH 4.5, and pH 6.8 were bridged between Clinical 2 phase tablets and Clinical 3 phase tablets. The bridging comparison between Clinical 2 phase tablets and Clinical 3 phase tablets showed rapid release (>85%, 15 minutes) at pH 1.2 and pH 4.5, and f2 > 50 at pH 6.8.Bridging of Phase 2 and Phase 3 Clinical Tablets: The proposed commercial capivasertib film-coated tablets are identical in quality and proportion to the Phase 3 clinical film-coated tablets (used in pivotal clinical studies), but are differentiated by the use of imprinting; the Phase 3 clinical tablets are conventional tablets, while the commercial tablets are imprinted. From a manufacturing process perspective, the imprinting on the commercial tablets represents a minor variation.Therefore, the company was required to provide dissolution data for the proposed commercial tablets of 160 mg and 200 mg strengths using QC's dissolution method during a teleconference held on September 27, 2013. The company provided the dissolution data of the printed tablets as required. Both strengths of the drug showed very rapid release (>85% within 15 minutes), indicating that printing had no effect on the drug dissolution."Interpretation"As can be seen from Figure 11 above, the clinical Phase 1 formulation is a capsule, while the clinical Phase 2 formulation is a tablet, indicating a significant change in dosage form. The company conducted a comparative study of the relative bioavailability in vivo, and the results showed no significant difference in the in vivo data between the two formulations. However, the dissolution rate of the capsule in vitro was significantly slower than that of the Phase 2 tablet. This indicates that the absorption of the formulation in vivo is not related to the dissolution rate in vitro. Therefore, the in vitro dissolution test can be used solely as a QC release method.Phase 3 and the proposed commercial formulation, based on the Phase 2 tablets, have been marked with engravings. Through dissolution comparisons at different pH levels, no significant differences were found, and the proposed dissolution method demonstrated very rapid dissolution (>85% within 15 minutes).Apart from the changes in the prescription, the company has not made any changes to the place of origin or key processes. Therefore, more comparative data is not shown in biopharmaceutics.Author's Excellent Original Collection
1、Common Difficulties in API Process and Communication in Innovative Drug Development
2、Common Difficulties of "Formulation Engineers" in Innovative Drug Development
3. Challenges Related to "Changes" in Innovative Drug Development
4、Key Challenges in "Quality Analysis and Control" in Innovative Drug Development (1)
5、Key Challenges in "Quality Analysis and Control" in Innovative Drug Development (2)
6、Analysis of Innovation Drug R&D Difficulties and Discussion on CMC Research Strategies
7、Analysis of "Questions and Answers on the Technical Guidelines for Research on Post-Approval Changes in the Chemistry of Listed Chemical Drugs (Trial) - API Changes"
8、FDA: Latest Perspectives on Nitrosamine Risk Assessment in Active Pharmaceutical Ingredients
9、Nitrosamine「Legend」: Five Years of Reflection in the Regulatory and Pharmaceutical Worlds
10、[Study Notes] 2023 CDE Review Report
11、FDA Review: Bridging the Pharmaceutical Changes of Pirtobrutinib (Complete)
12、CDE: Overview of the Implementation of ICH Guidelines in China
13、"Interpretation" FDA Review: Repotrectinib Capsules 5 CMC Meeting Contents
14、FDA: CMC Focus Points in the IND Phase
15、Difficulties and Suggestions in Drug Registration Inspection
With nearly 20 years of experience in drug development, specializing in new drug R&D and registration submission. In the past five years, successfully submitted nearly ten small molecule new drugs for IND applications in both China and the US, and achieved successful marketing application for two Class 1 anti-tumor new drugs. Previously held positions at a large CRO pharmaceutical R&D company, USP Greater China R&D Center, and a Hong Kong-funded API factory, leading MNC quality research projects, USP monograph updates, and guiding pharmaceutical QC laboratories to pass national GMP inspections and WHO audits.Invited by the China Chamber of Commerce for Import and Export of Medicines and Health Products, I led the planning of the salon on "Quality Research and Registration Strategies for Small Molecule Innovative Drugs" at the 22nd CPHI China World Pharmaceutical Ingredients Exhibition and delivered a keynote speech. Meanwhile, I was also invited by professional pharmaceutical forums to give more than ten keynote speeches, including "Key Points and Case Analysis of Quality Research for Innovative Drugs," "Common Issues and Case Analysis in Communication and Exchange during New Drug Applications in China and the US," "FDA and EMA Control Strategies for Nitrosamine Impurities," "Statistical Evaluation of Analytical Method Development, Validation, and Transfer," and "Case Analysis of Cleaning Validation in FDA 483." For more exciting content, please follow:▲ Follow the Wenliang Channel, Explore the Unknown World