A New Era in Tricuspid Valve Therapy: Transcatheter Approaches Drive Procedural Volume Growth
Abbott
Diagnostic and pharmaceutical product manufacturers
Edwards Lifesciences
Cardiovascular Surgical Equipment Provider
In the medical field, every technological breakthrough has the potential to bring new life to countless patients. Today, we are going to talk about a new technology that is expected to change the treatment landscape for tricuspid valve disease — transcatheter tricuspid valve treatment.
1. The Rise of Transcatheter Tricuspid Valve Treatment
In recent years, transcatheter tricuspid valve treatment technologies have gradually emerged, including transcatheter edge-to-edge repair (TEER) and full valve replacement options. The emergence of these new technologies not only brings new treatment hope to patients with tricuspid valve disease but may also drive the growth of surgical volume.
More than a decade ago, the introduction of transcatheter aortic valve replacement (TAVR) unexpectedly increased surgical volumes. At that time, as the number of patients referred for TAVR grew, it was discovered that these patients were actually better surgical candidates. Moreover, in the early days of TAVR programs, the return on investment from launching transcatheter valve programs also drove additional surgeries. Today, a similar trend is emerging in some centers performing tricuspid interventions.
Take the team led by Dr. Gilbert H. Tang, a professor of cardiovascular surgery at the Icahn School of Medicine and the surgical director of the structural heart program at Mount Sinai Health System, as an example. They have been involved in the TRILUMINATE IDE trial from the beginning and now, with the FDA-approved Evoque transcatheter valve replacement device, their volume of tricuspid valve surgeries has significantly increased. They first screen most patients for transcatheter treatment.
2. Patient Selection and Evaluation
Patient selection and evaluation are crucial before implementing transcatheter tricuspid valve treatment.
If patients are ineligible for transcatheter repair or replacement due to anatomical structures, age, or surgical risks, a comprehensive evaluation by the cardiac surgeon of the heart team is required. All patients referred to the valve center will undergo CT scans to assess the anatomy and determine their suitability for transcatheter repair.
Taking TAVR as an example, if the patient is 65 years old or younger, surgery is usually recommended due to durability issues. This is because if the patient is expected to live another 20 to 30 years, they may require a second valve replacement. Although patients can avoid surgery through TAVR-in-TAVR, each valve will become smaller with the addition of extra hardware, and surgical replacement may eventually be necessary. Given that younger patients tend to tolerate surgery better, it is recommended that younger patients undergo surgery first and then receive minimally invasive TAVR later in life. Similar considerations may apply to tricuspid valve cases.
3. Tricuspid Valve Interventions in the New Era
In the past, tricuspid valve interventions were often considered high-risk or a last resort due to the complexity of the tricuspid anatomy and the typically referred patient population. However, the introduction of transcatheter therapies has begun to change this paradigm.
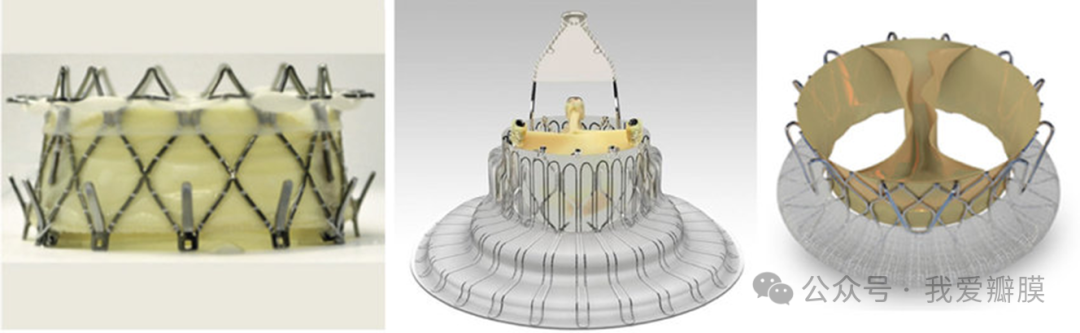
These new transcatheter options, such as the Abbott TriClip Transcatheter Edge-to-Edge Repair (TEER) system and the Edwards Lifesciences Evoque Tricuspid Transcatheter Valve Replacement (TMVR) system, primarily target patients facing moderate or high surgical risk. They allow for minimally invasive treatment of the valve, thereby improving organ preservation and accelerating patient recovery time.
Once, the tricuspid valve was called the "forgotten valve" because there were few options for patients and surgical outcomes were unsatisfactory. Most tricuspid valve patients were not referred for surgery, or they expressed that they did not want open-heart surgery. Some surgeons believe that previous studies might have indicated poor outcomes, but the trials mostly included severely ill patients. However, with the advent of minimally invasive options, this situation may change, and in the future, more patients than expected might start being referred to structural heart centers.
4. Team Collaboration and Patient Communication
When deciding whether to proceed with transcatheter tricuspid valve treatment, a team-based, holistic approach is required to determine which option is best among the transcatheter choices, or whether repair or replacement is more suitable. This decision typically depends on the patient's anatomy and imaging results.
For example, if imaging shows complex anatomy, valve replacement may be considered, but this may also increase certain risks and lead to longer hospital stays for the patient. These are some of the trade-offs that the heart team must consider and discuss in an open dialogue with the patient and referring cardiologist.
To help these discussions and better select patients, the Society of Thoracic Surgeons (STS) released the Tricuspid Valve Surgery Risk Score in April 2024. This is a benchmark based on decades of previously collected data. Additionally, the TRI-SCORE, released in Europe, also studied the same type of patients, attempting to stratify their risks according to different comorbidities or characteristics to determine which options might be best from a surgical perspective.
Overall, these innovations have the potential to reshape the management of tricuspid valve disease in the United States, where surgical intervention for the tricuspid valve has historically been less common. With the continuous development and refinement of transcatheter tricuspid valve treatment technologies, there is good reason to believe that more patients with tricuspid valve disease will benefit from these minimally invasive treatment options in the future, thereby improving their quality of life and prognosis.
A New Era of Tricuspid Valve Treatment Has Arrived – Let’s Look Forward to Transcatheter Therapies Bringing More Benefits to Patients!