
Percutek Therapeutics
Developer of Minimally Invasive Cardiovascular Treatment Devices

Today, I will introduce to youProfessor Gao Zhanfeng's Team from the Affiliated Hospital of Inner Mongolia Medical UniversityTwo brilliant cases of TEVAR surgery using V-18 guidewires for in-situ reconstruction of arch branches were presented. In both cases, the proximal end of the lesion had reached the root of the left subclavian artery (LSA), with a clearly insufficient proximal anchoring zone, necessitating the extension of the anchoring zone and reconstruction of the LSA. Given the short distance between the left common carotid artery (LCCA) and the LSA, selecting the optimal surgical plan became crucial for treatment. This required not only effective closure of the lesion but also efficient reconstruction of the left subclavian branch while ensuring the patient's long-term prognosis.
Professor Gao Zhanfeng's team, with rich clinical experience, successfully sealed the thoracic aortic lesion using the Percutek Therapeutics thoracic aortic stent graft. At the same time, the team innovatively employed a V-18 guidewire to efficiently complete the reconstruction of the LSA through in-situ fenestration technology. The patient recovered well after the surgery, fully demonstrating the superiority of the surgical plan and the team’s exceptional skills.
Gender:Male
Age:84 years old
History of Present Illness:Aortic arch aneurysm discovered during physical examination 7 days ago.
Past Medical History:Generally in good health.

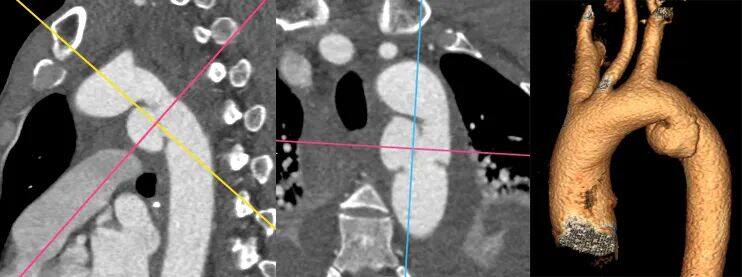
Preoperative Three-dimensional Reconstruction

Preoperative CTA Cross-Section
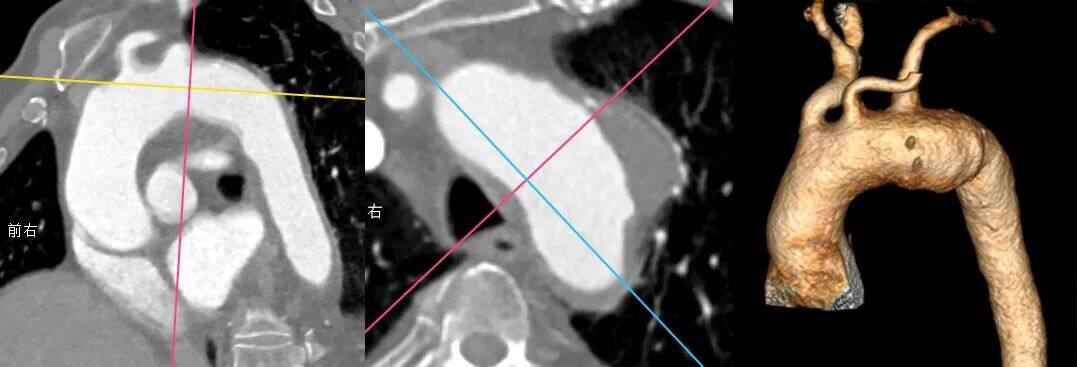
Condition of the aortic arch lesion
Pseudoaneurysm of the aortic arch, located on the anterior wall of the arch, with the proximal end already involving the root of the LSA, and an obvious insufficient proximal anchoring zone. The distance between LCCA and LSA is only 10mm, requiring proximal extension of the anchoring zone and reconstruction of the LSA.
The torsion angle of the thoracic aorta is large, and the LSA originates from the posterior wall of the aortic arch. Its ostium is large and "crater-shaped," which creates challenges for in-situ fenestration angle control during surgery. Additionally, common covered stents on the market are more difficult to fenestrate.
The pseudoaneurysm of the aortic arch is significantly dilated, requiring high proximal sealing performance for the thoracic aortic stent graft.
Multiple plaques at the root of the LSA should be handled with gentle care.
Surgical Plan Strategy
Thoracic Endovascular Aortic Repair with Direct Coverage of the Left Subclavian Artery: The procedure is simple and effective, but covering the left subclavian artery may lead to clinical manifestations of posterior circulation ischemia and upper limb ischemia in patients.
Endovascular Repair of Thoracic Aortic Stent Graft + Left Subclavian Artery Chimney Technique: The surgical procedure is relatively simple, but the left subclavian artery is tortuous and narrow, with a higher risk of endoleaks and occlusion, and the mid-to-long-term outcomes are suboptimal.
Endovascular Repair of Thoracic Aortic Stent Grafts with In Vitro Fenestration: Excellent sealing of lesions, preservation of original hemodynamic characteristics, but complex operation. Preoperative stent modification is required based on measurement results, which is time-consuming; intraoperative precise alignment and super-selective window positioning are required, posing higher risks.
Endovascular Repair of Thoracic Aortic Stent Graft + In-situ Fenestration: Effective sealing of the lesion, no need for preoperative stent modification. However, traditional in-situ fenestration of aortic stent grafts has high requirements for interventional devices, necessitating special membrane-piercing instruments such as in-situ fenestration needles, lasers, and biopsy needles.
The Hua Mai thoracic aortic stent graft can perform in-situ fenestration using the soft tip of a CTO guidewire. Considering the mid-to-long term treatment outcomes and the simplicity of intraoperative manipulation, after comprehensive evaluation, Professor Gao Zhanfeng's team chose Hua Mai • Tian Yi.®Endovascular repair of the thoracic aorta with a covered stent graft and reconstruction of the left subclavian artery using the in-situ fenestration technique.
Endovascular Repair of Thoracic Aortic Aneurysm with Stent Graft, In-situ Fenestration and Reconstruction of Left Subclavian Artery
01. The patient was placed in the supine position under local anesthesia, with routine disinfection and draping. The left brachial artery was punctured, and a 6F sheath and steerable catheter were inserted. The right femoral artery was punctured, two pre-set sutures were placed, and a 14F sheath was inserted. The angiography catheter was advanced to the ascending aorta, and angiography showed a pseudoaneurysm of the thoracic aorta located at the ostium of the LSA.

Preoperative Angiography
02. Insert the Percutek Therapeutics PTBS4238180 thoracic aortic stent at the posterior edge of the LCCA opening, slowly release 1-2 segments, and after confirming precise positioning with another angiography, release the main body.

Implantation of Percutek Thoracic Stent

Slow Release 2-Section Confirmation Positioning
03. The V-18 guidewire was exchanged through the left brachial artery, and the membrane was successfully punctured with the assistance of a steerable catheter, entering the aorta.

Angiography confirms the position and morphology of LSA.

V-18 Guidewire Successfully Penetrates Membrane
04. A single-bend catheter was inserted into the right femoral artery and used with a basket guidewire to capture the V-18 guidewire, which was then pulled out of the body to establish a track. Subsequently, a 5-150mm Saber and an 8-40mm EV3 balloon were used sequentially to dilate and create a fenestration.

Balloon Dilation Window Opening

Angle Adjustment Confirmation
05. The LSA guidewire was replaced, a 10-50mm Viabahn self-expanding covered stent was deployed, and post-dilation was performed using a 10-40mm Charger balloon.
Placement of Viabahn Stent
06. Angiography shows: The thoracic aortic stent is in good position and shape, with smooth blood flow. The aneurysm of the aortic arch is completely isolated without endoleak. All branches of the aortic arch are well visualized with unobstructed blood flow.

Final LAO Angiography

Final RAO Angiography
07. Withdraw all guidewires, catheters, and sheaths. Apply pressure dressing to each puncture site. Procedure completed.
Gender:Male
Age:50 years old
History of Present Illness:Two days ago, the patient suffered head and neck injuries, multiple bilateral rib fractures, and multiple systemic injuries due to a car accident. The local hospital provided emergency symptomatic treatment. CTA showed Stanford Type B aortic dissection.
Past Medical History:Generally healthy.

Preoperative Three-dimensional Reconstruction
Preoperative CTA Cross-Section
Condition of the aortic arch
Stanford Type B Aortic Dissection, the tear is located on the lesser curvature side, and the proximal end has already involved the aortic root of the LSA, with a clearly insufficient proximal anchoring zone. The distance between the LCCA and LSA is only 6mm, requiring proximal extension of the anchoring zone and reconstruction of the LSA.
LSA originates from the posterior wall of the aortic arch, with a large opening in the shape of a "volcano mouth," which presents challenges for controlling the angle during in-situ fenestration. Additionally, common covered stents on the market are relatively difficult to fenestrate.
Patients with Type III aortic arch require high stability, passability, and flexibility of the stent delivery system during endovascular exclusion procedures. Additionally, the stent itself must possess excellent sealing, compliance, apposition, and minimal elastic recoil.
Considering the medium- to long-term treatment outcomes and the simplicity of intraoperative procedures, after comprehensive evaluation, Professor Gao Zhanfeng's team once again chose Huamao•Tianyi.®Endovascular repair of the thoracic aorta with a covered stent graft and reconstruction of the left subclavian artery using in-situ fenestration technology.
Endovascular Repair of Thoracic Aortic Aneurysm with Stent Graft + In-situ Fenestration for Left Subclavian Artery Reconstruction
01. The patient was placed in the supine position. After successful general anesthesia, routine disinfection and draping were performed. Both femoral arteries were punctured, with 2 suturing devices preplaced, and a 6F sheath was inserted. The left brachial artery was punctured, and a 6F sheath was inserted. Angiography revealed a descending aortic dissection, with the entry tear located on the lesser curvature side, and the false lumen involving the root of the left subclavian artery (LSA).

Preoperative Angiography
02. The Percutek Therapeutics PTBS3228180 thoracic aortic stent system was placed at the posterior edge of the LCCA ostium. After precise positioning, the main covered stent was deployed, followed by the bare stent. The delivery system was then withdrawn.

Implantation of Percutek Thoracic Stent

Slow-Releasing Thoracic Stent
03. The V-18 guidewire was exchanged through the left brachial artery, and the single-curve catheter successfully punctured the membrane. A support catheter was then advanced into the lumen of the covered stent. A snare device introduced via the right femoral artery captured the V-18 guidewire and pulled it out of the body to establish a track. The fenestration was sequentially dilated using 5-150mm Saber, 8-40mm Mustang, and 12-40mm Charger balloons.

5-150mm Balloon Dilation

8-40mm Balloon Dilation

12-40mm Balloon Dilation
04. A 13-50mm Viabahn self-expanding covered stent was implanted in the LSA, and post-dilation was performed using a 12-40mm Charger balloon.

Placement of Viabahn Stent

Balloon-Expandable Branch Stent
05. Angiography shows: The thoracic aortic stent is in good position and shape, with smooth blood flow, excellent isolation of the dissection, no endoleak, and good visualization of each branch of the aortic arch with unobstructed blood flow.
Final Angiography
06. Withdraw all guidewires, catheters, and sheaths. Apply pressure dressing to each puncture site. Procedure completed.
Postoperative Review and Comparison with Preoperative

Preoperative/Postoperative 3D Reconstruction

Preoperative/Postoperative CTA Cross-Section
Postoperative review showed good recovery, with smooth blood flow in all branches, no signs of cerebral infarction or cerebral ischemia, complete isolation of the aortic arch dissection entry and false lumen, no endoleak, and good stent position and morphology.
Summary of Case Experience
In the two cases shared this time, the patients' aortic lesions both involved the root of the LSA, with a significantly insufficient proximal anchoring zone. How to effectively seal the lesion while ensuring the patients' long-term prognosis became the primary challenge of the surgery. Additionally, due to the extremely close distance between the LCCA and LSA, and the LSA originating from the posterior wall of the aortic arch with a large, "volcano-like" opening, precisely controlling the guidewire angle to successfully puncture the membrane posed another major challenge. Moreover, the patients had Type III aortic arches, and the thoracic aorta exhibited significant torsion angles, placing extremely high demands on the stability, deliverability, and flexibility of the stent delivery system. At the same time, the covered stent needed to possess excellent sealing ability, conformability, apposition, and minimal elastic recoil.
In response to these challenges, Professor Gao Zhanfeng's team implemented precise measures, opting for the Percutek Therapeutics Thoracic Aortic Stent Graft System for treatment. During the procedure, the team successfully performed fenestration using only a V-18 guidewire. The graft at the fenestration site was easily penetrable and expandable, allowing for the efficient and safe supra-aortic reconstruction of the LSA. Postoperatively, the stent showed excellent morphology with significant lesion sealing and no endoleaks. The patient had a favorable prognosis, and the supra-aortic reconstruction outcome fully met preoperative planning expectations, showcasing the team’s exceptional technical expertise and extensive clinical experience.
Expert Introduction

Professor Gao Zhanfeng
Chief Physician and Professor at the Affiliated Hospital of Inner Mongolia Medical University, Doctor of Medicine, Master's Graduate Supervisor. Chairman of the Second Vascular Surgery Branch of the Inner Mongolia Autonomous Region Physicians Association; Chairman of the First Youth Committee of the Vascular Surgery Branch of the Inner Mongolia Autonomous Region Medical Association; Standing Committee Member of the Fourth Committee of the Vascular Surgery Branch of the Inner Mongolia Autonomous Region Medical Association; Member of the Vascular Trauma Group of the First Committee of the Vascular Surgery Physicians Branch of the Chinese Physicians Association; Standing Committee Member of the Second Thrombosis Prevention and Treatment Committee of the Peripheral Vascular Disease Professional Committee of the Chinese Society for Microcirculation; Member of the Second Diabetic Foot Expert Committee of the Peripheral Vascular Disease Professional Committee of the Chinese Society of Integrated Traditional and Western Medicine; Standing Committee Member of the First Perioperative Management Expert Committee of the Peripheral Vascular Disease Professional Committee of the Chinese Society of Integrated Traditional and Western Medicine; Deputy Chairman of the Inner Mongolia Branch of the Asia-Pacific Vascular Union; Chairman of the Endovascular Treatment Specialized Committee for Main Iliac and Lower Limb Arteries of the Inner Mongolia Branch of the Asia-Pacific Vascular Union; Standing Committee Member of the China International Exchange and Promotion Association for Medical and Health Care; Member of the Editorial Board of the Journal of Vascular and Endovascular Surgery.

Department Introduction
The Affiliated Hospital of Inner Mongolia Medical University
The Vascular Surgery Department of the Affiliated Hospital of Inner Mongolia Medical University pioneered the establishment of a specialized vascular surgery outpatient clinic in the entire region in 1997. It has consistently been committed to the prevention and treatment of vascular diseases, routinely performing various types of vascular surgeries, filling multiple gaps within the region and the hospital. After more than a decade of development, the department now encompasses three main research and treatment directions: arterial diseases, venous diseases, vascular tumors, and lymphatic vessel diseases. It has formed an excellent team that integrates comprehensive development in endovascular interventional therapy, surgical operations, and standardized medication. Our department currently has a total of 29 staff members. The outpatient and emergency visits reach nearly 10,000 people, with over 1,300 inpatients treated annually. The team possesses extensive clinical experience in various vascular surgeries and endovascular interventions and has gained acclaim for its high-quality medical services and excellent vascular surgical techniques.
Business Scope: Treatment of various peripheral vascular arterial, venous, lymphatic diseases, and large vessel diseases. Currently, routine procedures include endovenous laser closure, minimally invasive rotary excision, and new foam sclerotherapy for varicose veins; treatment of deep vein thrombosis, insertion and removal of upper and lower vena cava filters, femoral vein incision for thrombectomy, and catheter-directed intravascular thrombolysis; thoracic and abdominal aortic dissection aneurysm stent-graft exclusion; abdominal aortic aneurysm resection with artificial vascular grafting and stent-graft exclusion; treatment of acute arterial ischemia, Fogarty catheter embolectomy, catheter-directed thrombolysis, and balloon angioplasty with stent placement; interventional exploration, balloon angioplasty, and stent implantation for lower limb arteriosclerosis obliterans and thromboangiitis obliterans, as well as bypass surgery with artificial vessels; carotid endarterectomy and carotid stenting for carotid artery stenosis or occlusive disease; endovascular and surgical treatment for subclavian artery steal syndrome; resection of large carotid body tumors; surgical and minimally invasive treatment of various types of hemangiomas; surgical and interventional treatment of Budd-Chiari syndrome and portal hypertension; surgical and interventional treatment of various congenital or secondary vascular malformations; arteriovenous fistula treatment or arteriovenous fistula surgery for hemodialysis; laser treatment for capillary telangiectasia; treatment of acute traumatic vascular diseases, etc. A variety of high-difficulty and complex surgeries in the field of vascular surgery are performed in sync with those in China, and treatment methods have expanded to a comprehensive system that includes traditional surgery, modern minimally invasive endovascular surgery, and non-invasive diagnostic and therapeutic approaches. At the same time, close academic exchanges and collaborative platforms exist with leading vascular surgery centers in China (e.g., Peking Union Medical College Hospital, Beijing Friendship Hospital, China-Japan Friendship Hospital, Xiyuan Hospital of China Academy of Chinese Medical Sciences, Affiliated Hospital of Hebei Medical University, etc.). National Natural Science Foundation projects and regional scientific research projects have been applied for; dozens of academic papers have been published in important domestic and international journals.

END
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints; it is solely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is intended for healthcare professionals to stay informed and should not replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and its authors shall not bear any related responsibility.Contact email for collaboration:vascular@edoctor.work。
