
Percutek Therapeutics
Developer of Minimally Invasive Cardiovascular Treatment Devices

Today, I will introduce a case byProfessor Feng Jiaxuan, Department of Vascular Surgery, Ruijin Hospital, Shanghai Jiao Tong University School of MedicineChallenging Case Sharing: In Vitro Six-Window Endovascular Repair for Thoracoabdominal Aortic Dissection Involving Visceral Multibranch Arteries. In this case, the thoracoabdominal aortic dissection tear is level with the left renal artery, with proximal retrograde involvement extending to the celiac trunk artery and distal involvement reaching the left external iliac artery. Additionally, the right kidney has three accessory renal arteries. What surgical plan can safely and effectively treat this patient? Which covered stent can effectively seal the dissection lesion? And what technique should be used for visceral multibranch reconstruction while ensuring long-term prognosis? Professor Feng Jiaxuan's team implemented a precise treatment strategy, skillfully utilizing Percutek Therapeutics' aortic covered stents. Through the in vitro pre-fenestration technology, they successfully completed the surgery, and the patient had a good postoperative outcome.
Gender:Male
Chief Complaint:Sudden onset of abdominal pain and back pain for one week, persisting without relief.
Past Medical History:General health condition, with an 8-year history of hypertension. Two years ago, underwent "partial resection of the ascending aorta with artificial vessel replacement + aortic sinus repair".
Preoperative Diagnosis:Thoracoabdominal Aortic Dissection, Hypertension Grade 3 (High Risk).
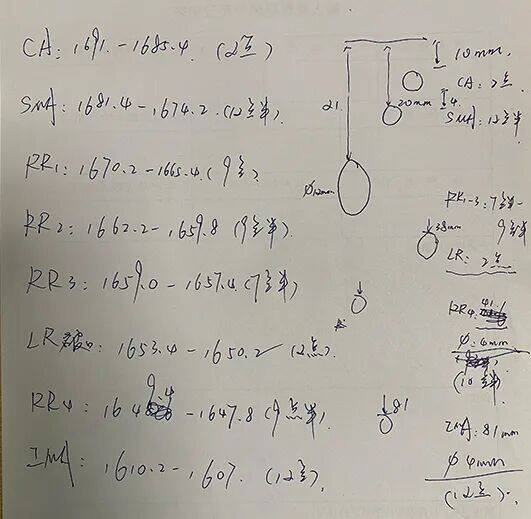
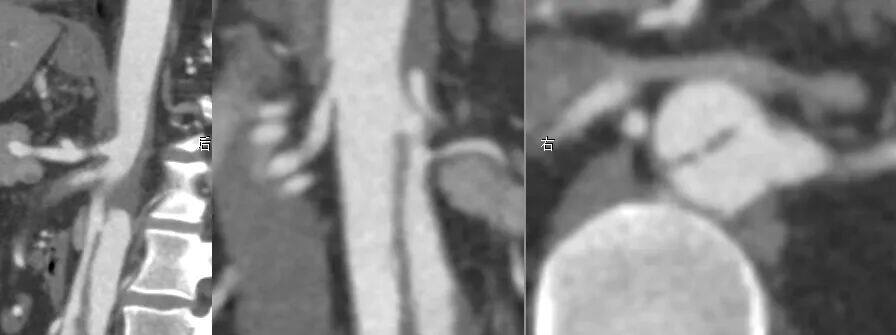
Detailed Explanation of CTA:Thoracoabdominal aortic dissection, with the tear aligned with the left renal artery (LRA) and supplied by the false lumen; retrograde dissection of the false lumen involves the celiac artery (CA) and superior mesenteric artery (SMA); SMA is supplied by both true and false lumens, with mural thrombus formation and mild stenosis of the lumen; four right renal arteries (RRA) are supplied by the true lumen; the inferior mesenteric artery (IMA) is supplied by the false lumen. The dissection extends distally to the left external iliac artery. The abdominal aorta has a small true lumen and a large false lumen, with the smallest part of the true lumen measuring only 18*6.7mm. The diameter of the proximal aorta near the CA is 22.5*17.6mm, the CA ostium is 6mm, and the SMA ostium.7mm, RRA1-RRA3 distance 12mm, left renal dissection orifice 6.5mm, CA distance from IMA opening 71mm. Small amount of pericardial effusion.

Preoperative Three-dimensional Reconstruction

Preoperative CTA Cross-Section
Treatment Strategy
The patient has a thoracoabdominal aortic dissection, involving multiple visceral branches including the CA, SMA, RRA, three accessory renal arteries, LRA, and IMA. The SMA is supplied by both true and false lumens, while the LRA is supplied by the false lumen. It is necessary to select a position above the CA as the proximal anchoring zone and reconstruct the SMA and LRA.
The distance from the proximal opening of the CA to the opening of the IMA is 71mm, plus a 10mm extension anchoring zone at both the proximal and distal ends, making the available abdominal aortic main body stent grafts in the market insufficient in length. Additionally, the true lumen of the abdominal aorta is small, while the false lumen is large, with an overall tapering shape. Considering these factors, it is advisable to select an aortic stent graft with a bare stent at the leading end and a significant taper for treatment.
The distal end of the dissection extends to the left external iliac artery, with stenosis of the true lumen, requiring reconstruction of the left iliac limb.
The chimney surgery is relatively simple to perform, but it may have significant endoleaks and unsatisfactory isolation effects, with suboptimal mid- to long-term outcomes; although in-situ fenestration provides good isolation and does not require preoperative stent modification, it demands advanced interventional equipment; ex-situ fenestration, while challenging the operator's surgical skills, offers excellent dissection isolation and can best preserve the original hemodynamic characteristics.
Thoracic and abdominal aortic stent graft endovascular exclusion, left iliac artery stent graft implantation, superior mesenteric artery stent implantation, left renal artery stent implantation, inferior mesenteric artery stent implantation, abdominal aortic balloon angioplasty.
01. The patient was in the supine position, under general anesthesia, disinfected and draped. The left brachial artery was dissected, and the left brachial artery was isolated and suspended for backup. Bilateral femoral arteries were successfully punctured using the modified Seldinger technique. Two suturing devices were pre-embedded, and 8F short sheaths were placed respectively. A marker pigtail catheter was introduced through the right femoral artery to above the CA, and angiography revealed a thoracoabdominal aortic dissection.

Preoperative Angiography
02. In vitro release of Percutek Therapeutics PTBS2620150 stent graft. Based on preoperative CTA measurement data, perform in vitro pre-fenestration at the CA, SMA, RRA1-3, LRA, RRA4, and IMA positions respectively, and suture window markers for standby after reassembly.




In Vitro Fenestration Modification of Percutek Therapeutics Covered Stent
03. A marker pigtail was introduced through the left femoral artery, and the aforementioned Percutek Therapeutics stent graft, pre-fenestrated externally, was introduced through the right femoral artery. The proximal end was positioned 1 cm above the celiac artery, and the fenestration markers were aligned with each branch according to the preoperative planning scheme, followed by gradual deployment of the stent.

Implantation of Percutek Pre-opened Fenestrated Stent Graft

Slow Release 1-3 Percutek Stents
04. A 9F long sheath was introduced into the visceral region of the abdominal aorta through left brachial artery puncture. The superior mesenteric artery (SMA) was super-selected, and a Viabahn stent was delivered. After confirming accurate positioning, the stent was deployed. The right renal artery (RRA) and the right accessory renal artery were then super-selected. After ensuring the fenestrated stent graft from Percutek Therapeutics was accurately aligned with the window, bare stents were implanted in each location.

Successful Superselection of SMA

SMA Placement and Viabahn Release

SMA Angiography

Successful Superselection of RRA
05. A modified pigtail catheter was introduced through the left brachial artery, passing through the LRA plane rupture to super-selectively enter the LRA. A Viabahn stent was then advanced across the false lumen, and after confirming accurate positioning, the stent was deployed.

Successful Superselection of LRA

LRA Placement of Viabahn and Angiographic Confirmation

LRA Releases Viabahn

Angiography Confirmation
06. Continue to release the distal end of the pre-opened Fenestrated Hu Mai Stent, after successfully super-selecting the IMA, introduce the Viabahn stent, and release it after confirming the accurate position of the stent.

RAO Angiography

LAO Angiography

Successful Superselection of IMA

Angiography Confirmation
07. Release the proximal bare stent of the pre-opened window Hu Mai covered stent, and confirm with angiography that each stent has a good shape and blood flow in each branch is unobstructed.

Release of Percutek Therapeutics' Proximal Bare Stent

Abdominal Aortography
08.The pre-opened fenestrated Percutek iliac limb PAIL1610095 was introduced via the left femoral artery, with the fenestration marker aligned with the left internal iliac artery as planned. After accurate positioning, it was deployed. Angiography showed significant false lumen opacification due to a distal dissection in the left iliac limb. A Viabahn stent was placed at the distal end, and a compliant balloon was used to dilate the proximal and distal ends of the left external iliac artery, as well as areas of stenosis and overlap.

True lumen of the left femoral artery placed into the iliac branch

Adjust Window Positioning

Reconfirm the position after the iliac branch release.

Superselective angiography confirmation

Obvious opacification of the distal false lumen in the left iliac artery

After placing a stent in the left external iliac and performing balloon dilation
09.Final angiography showed that each stent was in good shape, the entry tear and false lumen of the thoracoabdominal aortic dissection were completely isolated, and the visceral branch arteries and bilateral iliac arteries were well visualized.

Final Angiography

Distal End of Iliac Limb
10.Withdraw the guidewire and catheter, apply local pressure dressing at the puncture site. The operation proceeded smoothly.


Postoperative 3D Reconstruction

Postoperative CTA Cross-Section
Summary of Case Experience
This patient has a thoracoabdominal aortic dissection, which has involved the CA, SMA, RRA, LRA, and multiple right accessory renal arteries, as well as the SMA. The LRA is supplied by the false lumen, while the SMA and IMA are supplied by both true and false lumens. Due to insufficient proximal anchoring zone, it is necessary to extend the anchoring zone upward and reconstruct the branch arteries. Additionally, the dissection extends distally to the left external iliac artery, with stenosis of the true lumen, requiring reconstruction of the left internal iliac artery. The distance between the CA and IMA is approximately 71mm. Considering the required length of the proximal and distal anchoring zones, the length of commercially available aortic abdominal main body covered stents is insufficient. Therefore, this treatment selected an aortic covered stent with a bare stent at the head end and a large taper for the procedure.
Percutek TherapeuticsAortic Stent GraftIt is the only aortic stent graft in China that has conducted a controlled clinical trial before market approval so far. It has an excellent one-year complete false lumen thrombosis rate, with a complete thrombosis rate of 96%, surpassing similar imported products, and has the following advantages:
01.Proximal bare stent design ensures firm anchoring, with a post-release design for the bare stent;
02.The proximal "ə" and "O"-shaped markers are clearly visible, accurately positioned, and can serve as a guide for fenestration placement.
03.Dual-mini height stent ring design, with shorter metal stent wires for easier fenestration operation;
04.The stent ring changes in diameter, height, and number of peaks, providing excellent sealing effect, better wall apposition, and easily conforming to three-dimensional tortuous aortic lesions.
05.The overall stent graft is tightly woven, and the fibers are not prone to slipping after fenestration;
06.Delivery device with a nickel-titanium alloy core, flexible and powerful, easily conquering Type III arch.
Professor Feng Jiaxuan's team ultimately chose the Percutek Therapeutics aortic stent graft to complete this patient's surgery. The surgical process went smoothly and met expectations.
Expert Introduction

Professor Feng Jiaxuan
Associate Chief Physician and Associate Professor of the Department of Vascular Surgery at Ruijin Hospital, Shanghai Jiao Tong University School of Medicine; Medical Doctor; Recipient of Shanghai's "Oriental Talent," Shanghai Science and Technology Rising Star, and Outstanding Military Doctoral Dissertation Awards. Clinical expertise includes minimally invasive diagnosis and treatment of various vascular diseases, with particular strengths in critical and complex aortic diseases, visceral artery diseases, arteriosclerosis obliterans caused by geriatric metabolic diseases, venous thromboembolism, hereditary vascular diseases, comprehensive treatment, and rapid rehabilitation. Academic positions: Member of the Endovascular Specialty Committee of the Chinese Medical Doctor Association, Youth Committee Member of the Vascular Surgery Specialty Committee of the National Cardiovascular Disease Expert Committee, Deputy Secretary General of the Youth Committee of the Peripheral Vascular Disease Specialty Committee of the Chinese Society of Microcirculation, Member of the Visceral Artery Disease Specialty Committee of the Vascular Surgery Branch of the Chinese Medical Doctor Association, International Member of the American Society for Vascular Surgery (SVS), International Member of the European Society for Vascular Surgery (ESVS), and Member of Faculty of 1000 (an authoritative international peer-review academic institution).

Professor Sun Yudong
Deputy Chief Physician and Associate Professor of the Department of Vascular Surgery at Ruijin Hospital, affiliated with the Shanghai Jiao Tong University School of Medicine; Medical Doctor, Postdoctoral Fellow, and Master's Supervisor. Long-term engagement in clinical and pathological mechanism research on vascular surgical diseases such as abdominal aortic aneurysms, aortic dissections, carotid artery stenosis, lower extremity arteriosclerosis obliterans, venous thrombosis, and varicose veins. Has published 15 SCI papers as the first/corresponding author. Contributed to the editing of 9 monographs, serving as the associate editor for one. Holds 24 authorized patents, including 4 invention patents. Principal investigator for one National Natural Science Foundation of China project and participant in six others. Academic positions: Member of the Endovascular Specialty Committee of the Chinese Medical Doctor Association, Member of the Vascular Surgery Group of the Jiangsu Branch of the Chinese Medical Association, Member of the Youth Expert Committee on Peripheral Vascular Diseases of the Chinese Society for Microcirculation, and Member of the Youth Committee of the International Union of Angiology (China Chapter). Serves as editorial board member for the "Chinese Journal of Vascular Surgery (Electronic Edition)," "Chinese Journal of Vascular Surgery," and "Journal of Clinical Surgery," as well as a youth editorial board member for the "Medical Journal of the Chinese People's Liberation Army" and the "Chinese Journal of Traumatology."

Professor Guanglang Zhu
Vascular Surgeon at Ruijin Hospital, affiliated with the Medical College of Shanghai Jiao Tong University, holding a Doctor of Medicine degree. Specializes in endovascular minimally invasive treatments for various vascular diseases, including aortic dissection, aortic aneurysm, carotid artery stenosis, lower extremity arterial sclerosis occlusion, deep vein thrombosis of the lower extremities, and pulmonary embolism. Has published 9 SCI papers as the first or co-first author, holds 3 authorized invention patents and 10 utility model patents, one of which has been successfully applied. Serves as the Secretary of the Main Iliac Artery Disease Committee under the Endovascular Specialty Committee of the Chinese Medical Doctor Association, the Youth Editorial Board Member of the English journal Translational Surgery, and the Youth Editorial Board Member of the Chinese Journal of General Surgery. Honored with titles such as Outstanding Graduate of Shanghai and Outstanding Resident Physician of Shanghai.

Department Introduction
Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine
General Surgery Vascular Surgery

Ruijin Hospital Vascular Surgery Department Regularly Accepts Visiting Physicians
Contact: Dr. Sun 18818263589
The scope of diagnosis and treatment of the department covers all vascular diseases, including aortic, lower limb arterial, carotid artery, visceral artery, venous thrombosis, and varicose veins in the lower limbs. In particular, it has developed comprehensive treatment characteristics that combine endovascular minimally invasive techniques with open surgery for complex aortic dissections, aortic aneurysms, and other large artery diseases, as well as peripheral artery diseases such as lower limb arteries and carotid arteries. Each year, it attracts trainees from across China for further study and hosts specialized academic conferences, cultivating professional talent for the field of vascular surgery in China.

END
Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in related disease areas. The information content published on this platform does not imply agreement with its descriptions or viewpoints, but is only for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will handle it as soon as possible. This information is intended solely for medical and health professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be regarded as medical advice. If such information is used for purposes other than staying informed, this platform and the author shall not bear any related responsibilities.Contact email for cooperation:vascular@edoctor.work。
