
Percutek Therapeutics
Developer of Minimally Invasive Cardiovascular Treatment Devices

Today, I will introduce to youJin Yiqi / Professor Xu Guoxiong Team, Suzhou Municipal HospitalTwo Brilliant Cases of In-situ Reconstruction TEVAR Surgery for Arch Branches Using Balloon Tip and 250T Guidewire In-situ PunctureTwo brilliant cases of in-situ reconstruction TEVAR surgery for arch branches using a balloon tip and 250T guidewire in-situ puncture were presented. One patient had Stanford Type B aortic dissection with the proximal end already involving the root of the LSA, while the other had Stanford Type B intramural hematoma with the proximal end already involving the root of the LCCA. Both cases had insufficient proximal anchoring zones and required proximal extension of the anchoring zone; the former needed LSA reconstruction, and the latter required double reconstruction of both LCCA and LSA. This not only demanded effective closure of the lesion but also efficient reconstruction of the arch branches while ensuring the long-term prognosis of the patients. Relying on their extensive clinical experience, the team led by Professor Jin Yiqi and Xu Guoxiong successfully closed the thoracic aortic lesions using the Percutek Therapeutics thoracic aortic stent graft. Meanwhile, the team innovatively employed the balloon tip and 250T guidewire in-situ puncture to efficiently complete the reconstruction of the arch branches through the in-situ fenestration technique. The patients recovered well post-operation, fully demonstrating the superiority of this surgical plan and the team's superb skills.
Gender:Male
Age:88 years old
History of Present Illness:One week ago, the patient underwent thoracic cavity occlusion and drainage surgery at another hospital for "tuberculosis." This morning, the patient suddenly experienced chest tightness and discomfort located in the posterior back, along with arrhythmia. After a sudden loss of consciousness, the patient spontaneously recovered. Examinations revealed a dissecting aneurysm of the descending thoracic aorta, intracerebral hemorrhage, and tuberculous pleurisy.
Past Medical History:Generally in poor health, with hypertension poorly controlled.

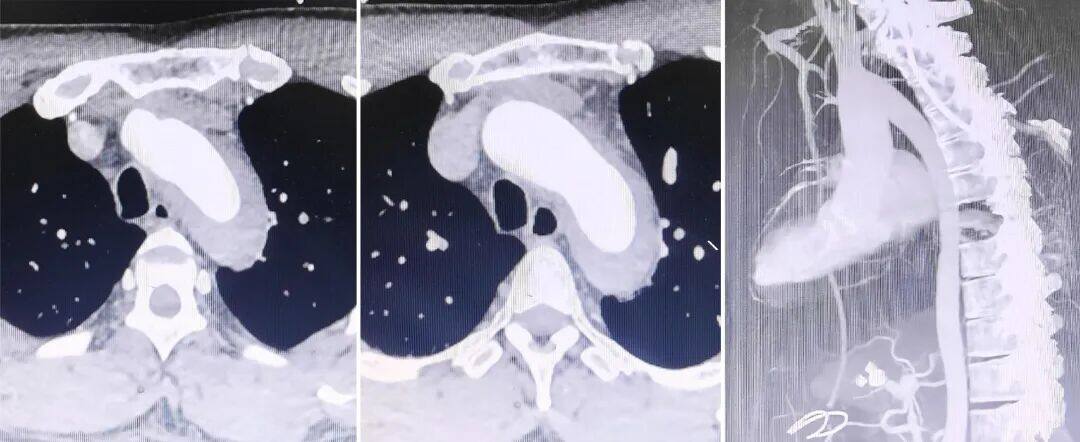
Preoperative Three-dimensional Reconstruction

Preoperative CTA Cross-Section
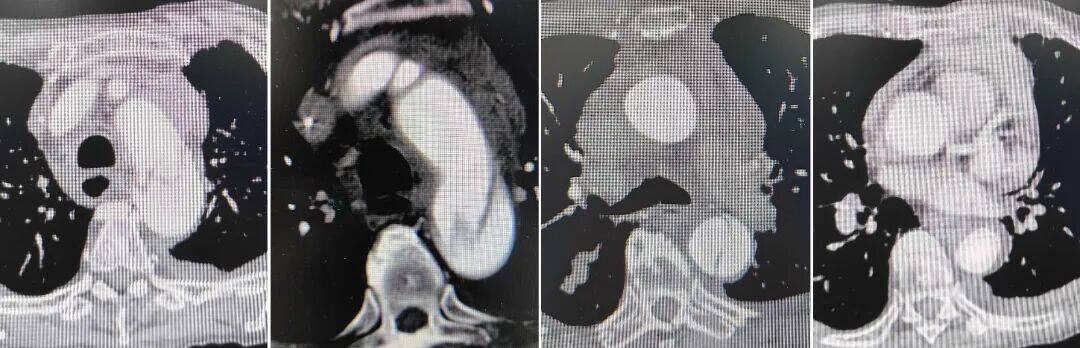
Condition of the aortic arch
The patient's condition is severe, with a risk of further rupture of the dissection. Surgery is needed as soon as possible to complete the operation safely and efficiently.
The larger the dissection opening, the higher the requirement for the proximal sealing of the thoracic aortic stent graft.
Stanford Type B Aortic Dissection, with the proximal lesion involving the root of the LSA and a significantly insufficient proximal anchoring zone. The distance between the LCCA and LSA is only 8mm, requiring proximal extension of the anchoring zone and reconstruction of the LSA.
The LSA originates from the posterior wall of the aortic arch, with tortuosity and stenosis, forming an acute angle with the aortic arch. Its ostium is large and presents a "volcano-like" morphology, posing challenges for in-situ fenestration angle control during surgery. Additionally, common covered stents on the market present significant difficulties for fenestration.
Patients with Type III aortic arch require high stability, passability, and flexibility of the stent delivery system during endovascular exclusion procedures. Additionally, the stent itself must possess excellent sealing, compliance, apposition, and minimal elastic recoil.
Surgical Plan Strategy
Thoracic Endovascular Aortic Repair with Direct Coverage of the Left Subclavian Artery: The procedure is simple and effective, but covering the left subclavian artery may lead to clinical manifestations of posterior circulation ischemia and upper limb ischemia in patients.
Endovascular Repair of Thoracic Aortic Stent Graft + Left Subclavian Artery Chimney Technique: The surgical procedure is relatively simple, but the left subclavian artery is tortuous and narrow, with a higher risk of endoleak and occlusion, and the mid- to long-term outcomes are suboptimal.
Endovascular Repair of Thoracic Aortic Stent Grafts with In Vitro Fenestration: Excellent sealing of the lesion, preservation of original hemodynamic characteristics is possible, but the procedure is complex. Preoperative stent modification based on measurement results is required, which is time-consuming; intraoperative precise alignment and ultra-selective window positioning are necessary, posing higher risks.
Endovascular Repair of Thoracic Aortic Stent Graft + In-situ Fenestration: Effective sealing of the lesion, no preoperative stent modification required. However, traditional in-situ fenestration of aortic stent grafts demands advanced interventional equipment, such as in-situ fenestration needles, lasers, biopsy needles, and other specialized membrane-piercing devices.
Percutek Therapeutics' Thoracic Aortic Stent Graft can perform in-situ fenestration using the soft tip of a CTO guidewire. Considering the medium- to long-term treatment outcomes and the simplicity of intraoperative manipulation, after comprehensive evaluation, Professor Jin Yiqi/Xu Guoxiong's team chose Percutek Therapeutics' Tianyi.®Endovascular repair of the thoracic aorta with a covered stent graft and reconstruction of the left subclavian artery using the in-situ fenestration technique.
01. The patient was placed in the supine position. After satisfactory general anesthesia, routine disinfection and draping were performed. The right femoral artery was punctured and sheathed, with 2 pre-placed sutures. A 10F sheath and a gold marker catheter were inserted and advanced into the aortic arch. Angiography revealed a Stanford Type B aortic dissection.
02. A 4cm longitudinal incision was made in the left upper limb to expose the brachial artery. A 6F sheath and catheter were inserted into the ascending aorta, then exchanged for an 8F steerable sheath, while retaining the catheter and Amplaz guidewire.
03. A gold marker catheter was introduced into the ascending aorta via the right femoral artery. Angiography revealed the rupture located distal to the LSA ostium, marking the three branches above the aortic arch. After exchanging for an ultra-stiff guidewire, a Percutek Therapeutics thoracic aortic stent graft (PTBS3430180) was deployed with its proximal end aligned distal to the LCCA ostium, precisely released to cover the LSA. Subsequently, one additional covered stent and one bare stent were placed distal to the Percutek stent to expand the true lumen. Angiography showed no significant endoleak.

Implantation of Percutek Therapeutics Thoracic Stent
04. The Connect 250T guidewire was advanced through the left upper limb, in conjunction with a steerable sheath, to adjust the angle and successfully puncture the membrane to enter the aorta.

Connect 250T Guidewire Successfully Penetrates Membrane
05. Sequentially use 6*40mm balloon, 8*80mm balloon to expand the fenestration, and smoothly place the steerable sheath into the aortic arch stent graft through the balloon-assisted sheath technique.

Balloon dilation after balloon placement

Balloon dilation after balloon placement

Balloon-expandable window

Sheathed Membrane Insertion
06. A single-bend catheter was inserted through the left brachial artery, and an Amplaz guidewire was exchanged. An 11*39mm balloon-expandable covered stent was implanted in the LSA, followed by dilation with an 8*60mm balloon. The final morphology was satisfactory.

LSA Stent Placement

Balloon-expandable branch stent

LSA Branch Stent
07. The final angiography showed that the position and shape of each stent were good, the aortic blood flow was unobstructed, and there was no significant endoleak; the blood flow within the LSA branch stent was unobstructed, with good antegrade blood flow in the LSA, and good imaging of bilateral carotid arteries and vertebral arteries, as well as good imaging of intracranial arteries. The false lumen was satisfactorily isolated.

Postoperative Angiography
08.Withdraw all guidewires, catheters, and sheaths. Suture the incision and apply local compression dressing. Procedure completed.
Gender:Male
Age:42 years old
History of Present Illness:Sudden onset of chest and back pain for 4 hours, severe pain accompanied by profuse sweating, significant chest tightness and shortness of breath, unable to be relieved. CTA examination at the local hospital suggested aortic dissection, and subsequently, the patient was admitted to our emergency department.
Past Medical History:Has undergone gastrointestinal bleeding surgery.

Preoperative Three-dimensional Reconstruction
Preoperative CTA Cross-Section
Condition of the aortic arch
Stanford Type B aortic intramural hematoma, with the proximal lesion extending to the root of the LSA and LCCA, showing a significant lack of proximal anchoring zone. The distance between the IA and LCCA is only 8mm, necessitating the expansion of the proximal anchoring zone and the reconstruction of the LCCA and LSA.
LSA originates from the posterior wall of the aortic arch, with a large opening in a "volcano crater" shape. It is tortuous, narrow, and angled, posing challenges for controlling the angle during in-situ fenestration. Additionally, common covered stents on the market present significant difficulties for fenestration.
Patients with Type III aortic arch require high stability, deliverability, and flexibility of the stent delivery system during endovascular exclusion procedures. Additionally, the stent itself must possess excellent sealing, conformability, apposition, and minimal elastic recoil.
Considering the medium- to long-term treatment outcomes and the simplicity of intraoperative procedures, after comprehensive evaluation, Professor Jin Yiqi/Xu Guoxiong's team once again chose Percutek Therapeutics.®Endovascular repair of the thoracic aorta with a covered stent graft, and reconstruction of the left common carotid artery and left subclavian artery using in-situ fenestration technology.
01. The patient was placed in the supine position under general anesthesia, with routine disinfection and draping. The right femoral artery was punctured and sheathed, with 2 suturing devices pre-installed, and a pigtail catheter was advanced into the abdominal aorta.
02. An incision was made above the left elbow joint, the brachial artery was isolated and suspended with a rubber band, and then punctured. A 5F sheath was inserted, followed by the insertion of a catheter and guidewire. An adjustable bending sheath was exchanged into the ascending aorta, and the catheter and stiff ultra-smooth guidewire were retained. Under ultrasound guidance, the LCCA was punctured and an 8F sheath was inserted.
03. A gold marker catheter was advanced into the ascending aorta via the right femoral artery. Angiography revealed an intramural hematoma involving the root of the left common carotid artery (LCCA). The three branches of the aortic arch were marked, and a super-stiff guidewire was exchanged. A Percutek Therapeutics thoracic aortic stent graft (PTBS3228180) was then deployed flush with the posterior edge of the innominate artery (IA), completely covering the LCCA and the left subclavian artery (LSA).
04. A 7*40mm balloon was delivered via LCCA, with the balloon tip successfully penetrating the aortic stent graft membrane into the ascending aorta. After balloon dilation to create an opening, a 12*38mm balloon-expandable covered stent was placed and post-dilated upon deployment.

LCCA Balloon Tip Successfully Breaks Membrane

LCCA Balloon Dilation Window

Balloon-Expandable Covered Stent
05. A Connect 250T guidewire was advanced through the left brachial artery, in conjunction with a steerable sheath, successfully penetrating the aortic stent graft membrane into the ascending aorta. Fenestrations were created using 7*40mm and 8*40mm balloon dilations sequentially, followed by the deployment of a 12*38mm balloon-expandable covered stent, which was then post-dilated upon release.

Balloon Placement After LSA Puncture

Balloon Dilation Window Opening

LSA Stent Placement

Balloon-Expandable Branch Stent
06. Final angiography showed that the aortic stent, LCCA, and LSA branch stents were in good position and morphology. The blood flow in the aorta and its branches was unobstructed, with no significant endoleak. The lesion was satisfactorily isolated.

Postoperative Angiography
07. Final angiography showed that the aortic stent, LCCA, and LSA branch stents were in good position and morphology, with smooth blood flow in the aorta and its branches, and no significant endoleak. The lesion was satisfactorily isolated.
Intraoperative Procedures

Summary of Case Experience
The two cases shared in this presentation involve a patient with Stanford Type B aortic dissection whose proximal end has already affected the root of the LSA, and another patient with Stanford Type B intramural hematoma whose proximal end has reached the root of the LCCA. Both cases have insufficient proximal anchoring zones; the former requires reconstruction of the LSA, while the latter necessitates double reconstruction of both the LCCA and LSA. Therefore, how to effectively seal the lesion while ensuring the long-term prognosis of the patients becomes the primary challenge of the surgery. Additionally, the LSA originates from the posterior wall of the aortic arch, with a large opening shaped like a "volcano mouth," making precise control of the guidewire angle for successful membrane puncture another significant challenge. Moreover, both patients have Type III aortic arches with a significant torsion angle in the thoracic aorta, posing extremely high demands on the stability, deliverability, and flexibility of the stent delivery system. At the same time, the covered stent must exhibit excellent sealing ability, conformability, apposition, and minimal elastic recoil.
In response to these challenges, the Jin Yiqi/Xu Guoxiong professor team implemented precise measures by choosing the Percutek Therapeutics Thoracic Aortic Stent Graft System for treatment. During the procedure, the team successfully performed fenestration with ease using the balloon tip and a 250T guidewire. The stent graft’s membrane at the fenestrated area was easily penetrable and expandable, enabling efficient and safe supra-aortic reconstruction of the LSA and LCCA. Post-operation, the stent showed excellent morphology, significant sealing of the lesion, no occurrence of endoleak, and the patient had a favorable prognosis. The supra-aortic reconstruction outcome fully met the preoperative planning expectations, showcasing the team's exceptional technical expertise and extensive clinical experience.
Expert Introduction

Professor Jin Yiqi
Director of the Interventional Vascular Department at Suzhou Municipal Hospital, Chief Physician, and Master's Supervisor. Member of the Vascular Surgery Branch of the Jiangsu Medical Association and Deputy Leader of the Aortic Disease Study Group, Member of the Vascular Surgery Branch of the Jiangsu Physician Association, Member of the Comprehensive Study Group of the Interventional Medicine Branch of the Jiangsu Medical Association, and Member of the Vascular Surgery Study Group of the Suzhou Medical Association. In the past five years, published over 10 SCI papers, obtained 3 utility model patents, won two Second Prizes for the Introduction of New Medical Technologies in Suzhou, one Special Project for the Diagnosis and Treatment of Key Clinical Diseases in Suzhou, and received the Golden Finger Award for Surgery on the 2024 Doctor's Day at Suzhou Municipal Hospital. Specializes in the diagnosis and treatment of aortic diseases, minimally invasive treatment of traumatic thoracic-abdominal aortic injuries and pelvic fractures, and is especially a domestic leader in endovascular branch minimally invasive reconstruction for complex large vessel diseases.

Professor Guoxiong Xu
Deputy Director of the Interventional Vascular Department at Suzhou Municipal Hospital, Chief Physician. Member of the Lower Extremity Arterial Disease Committee of the Vascular Surgery Branch of the Jiangsu Medical Association, Member of the Aortic Disease Committee of the Vascular Surgery Branch of the Jiangsu Medical Association, and Deputy Chairman of the Interventional Therapy Committee of the Suzhou Integrated Traditional Chinese and Western Medicine Association. In the past five years, he has published over seven SCI papers, obtained two utility model patents, and received two second prizes for the Introduction of New Medical Technologies in Suzhou. He was named one of the Most Beautiful Workers of Suzhou in 2020 and received the Surgical Elite Award during the 2024 Physician's Day at Suzhou Municipal Hospital. Graduated from the Seven-Year Program (Bachelor-Master continuous) at the Medical College of Soochow University in 2008, and completed advanced training in vascular surgery at Zhongshan Hospital of Fudan University, Shanghai in 2013. Specializes in vascular surgery with extensive experience in the diagnosis and treatment of various peripheral vascular diseases. Skilled in open vascular treatments: carotid endarterectomy, various types of vascular bypass surgeries, artificial blood vessel replacement for abdominal aortic aneurysms, etc.

Department Introduction
Interventional Vascular Department, Suzhou Municipal Hospital

Currently, the Interventional Vascular Department of Suzhou Municipal Hospital has 62 beds and a total of 20 physicians, including 4 chief physicians and 6 deputy chief physicians. The department is well-equipped with advanced facilities, such as 2 color vascular ultrasound machines, 4 large vascular machines (DSA), CT vascular 3D imaging, peripheral vascular detectors, and various other vascular diagnosis and treatment equipment, striving to provide high-quality medical services to the general public.
Throughout the year, the team has cumulatively completed 150 minimally invasive surgeries for aortic dissection and aortic aneurysms, taking the lead in introducing and carrying out many new technologies with unique characteristics, including complex endovascular reconstruction techniques for branched aneurysms and fenestration techniques for the three branches of the aortic arch.
The diseases diagnosed and treated in our department also include the treatment of various massive or complex bleeding, such as epistaxis, hemoptysis, postpartum hemorrhage, and bleeding from esophageal and gastric varices due to liver cirrhosis; establishment and maintenance of hemodialysis access for uremic patients; central venous catheterization: including implantation of various central venous catheters, implantation of infusion ports, and implantation of temporary/semi-permanent hemodialysis catheters. Tumor interventions include percutaneous arterial infusion chemotherapy + embolization, including transcatheter arterial chemoembolization (TACE) for liver cancer and bronchial artery chemoembolization for lung cancer, etc.; microwave ablation and radiofrequency ablation of tumors; organ tissue biopsy, renal pelvis puncture drainage, external biliary drainage, gastrostomy, etc.

END
Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in related disease areas. The information content published on this platform does not imply agreement with its descriptions and viewpoints, but is only for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will handle it as soon as possible. This information is intended solely for medical and health professionals to stay informed, and such information cannot replace professional medical guidance in any way, nor should it be regarded as diagnostic or treatment advice. If such information is used for purposes other than staying informed, this platform and the author shall not bear any related responsibility.Contact Email for Cooperation:vascular@edoctor.work。
