"Robbing Peter to Pay Paul": Harvesting Bone from the Femoral Condyle to Fill Tibial Defects in Tibial Plateau Fractures—A Feasible Minimally Invasive Technique

Acumed
Medical Device Manufacturer

Proximal Tibial Fractures are Common in Postmenopausal Women and Young Men, and These Fractures are Often Associated with Articular Surface Collapse. The Goal of Surgery is to Restore Limb Alignment and Articular Surface Integrity to Maintain Long-Term Joint Function. After Reduction, Defects are Left at the Epiphyseal Bone Where the Articular Fragments are Located, Which are Best Filled with Bone or Bone Substitutes for Two Reasons: First, Bone Grafting Helps Maintain the Stable Position of Articular Fragments Before Final Internal Fixation and During the Healing Process; Second, Bone Grafting Exhibits Excellent Osteogenic and Osteoinductive Properties. Additionally, the Graft Can Also Fill the Gap Between the Screws and the Remaining Subchondral Bone Beneath the Articular Fragments.
Material options for filling defects include autologous bone grafts (most commonly harvested from the iliac crest), allogeneic bone grafts from bone banks, and synthetic bone substitutes, which are also a common choice. The decision among the available options mainly depends on the surgeon's preference, but is also influenced by factors such as the size of the defect to be filled, the availability of the graft, patient-related factors, and cost. When the estimated volume of the defect to be filled is small (<20cc), we findThe technology described in this article is both economical and time-saving compared to other existing options.. In addition,This technique avoids additional surgical incisions for the patient.Previous reports of similar techniques did not use CT to evaluate postoperative cortical or cartilage penetration, nor did they assess new bone formation at the donor and recipient sites.
We describe a minimally invasive technique using the Acumed Bone Graft Harvesting System to harvest bone graft material from the lateral femoral condyle for the treatment of proximal tibial fractures with articular surface collapse, and report the outcomes of 12 patients treated with this technique.
All patients received general anesthesia and were prepped and draped according to institutional standards. On the operating table, the patient was placed in a supine position, with the femur fixed in an arthroscopic leg holder. All patients underwent an anterolateral straight incision centered on the Gerdy's tubercle for internal fixation of the fracture (Figure 1).
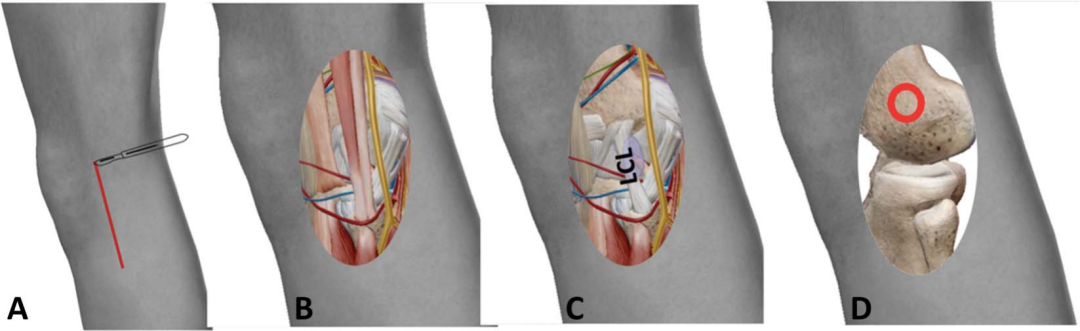
Figure 1 Schematic diagram of the surgical approach: The incision is centered on the Gerdy tubercle (A), and the iliac fascia is cut to enter the joint (B and C). Above the origin of the lateral collateral ligament (LCL), the cortical bone of the lateral femoral condyle is accessed through the entry point (red circle) to obtain cancellous bone from the distal femoral metaphysis (D).
Through the proximal part of this incision, the joint capsule is incised anterior to the lateral femoral condyle to expose the femoral condyle, while taking care to preserve the origin of the lateral collateral ligament (Figure 1). If necessary, the incision can be extended proximally to improve exposure of the femoral condyle. Using a 12mm bone graft drill, and referencing the Blumensaat line, drill into the cancellous bone from the same entry point in alternating directions (Figure 2). This procedure is repeated up to four times until sufficient bone graft material is obtained (Figure 3). The amount of cancellous bone collected ranges between 20-40cc, which is sufficient to fill the defect after reduction of the displaced articular fragments. In some cases, absorbable hemostatic gelatin sponge may be placed at the bone harvesting site for hemostasis. The cortical drill holes are irrigated with sterile saline, followed by suturing of the joint capsule. Subsequently, the harvested bone graft material is packed and shaped into the defect beneath the reduced articular fragments using a tamp or syringe.
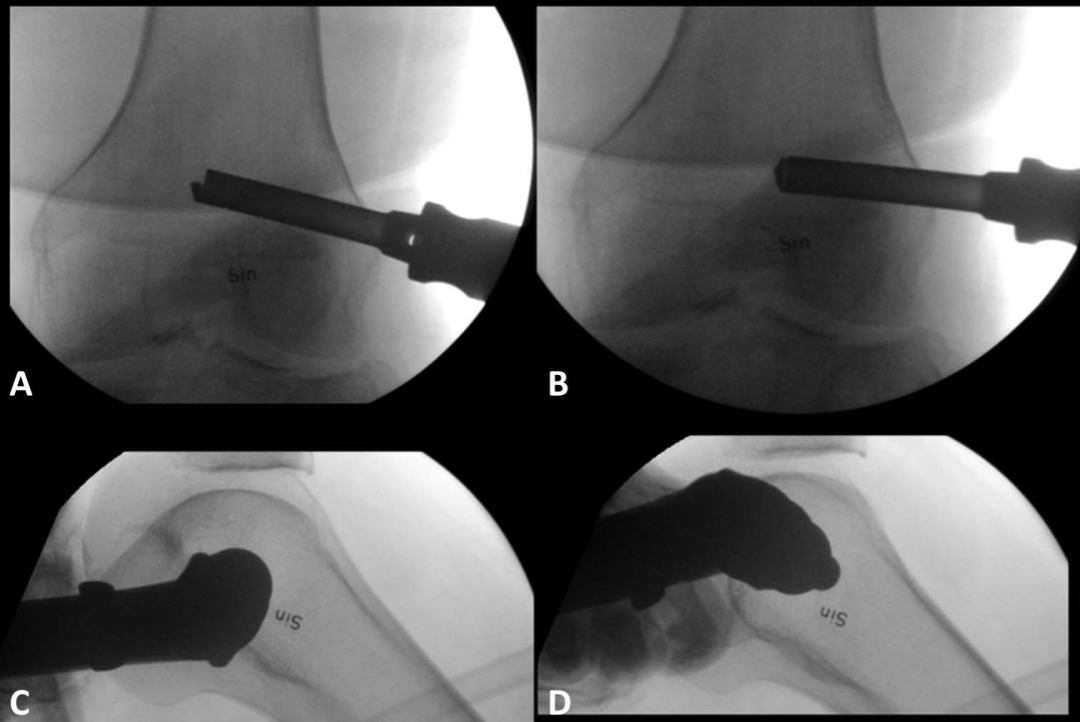
Fig. 2 Anteroposterior (A, B) and lateral (C, D) X-ray films showing bone harvesting devices in different directions.
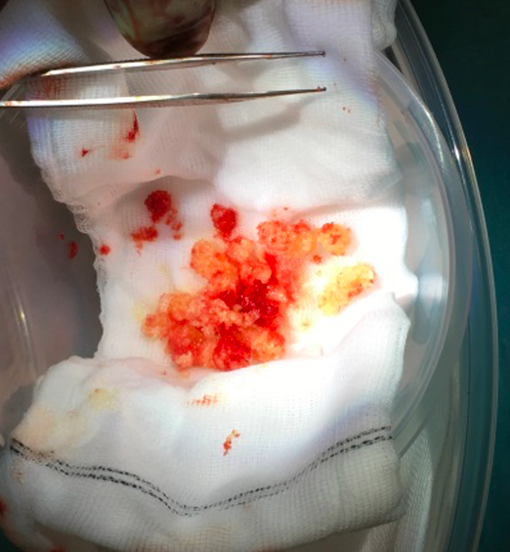
Figure 3 Bone graft extracted using a 12 mm drill bit.
Postoperatively, patients follow the lead surgeon's recommendations for activity, typically avoiding weight-bearing for 6 to 8 weeks. After the wound heals well, full range of joint motion exercises can be performed. Patients undergo CT examination and clinical follow-up at least 12 months postoperatively.
Fracture healing was assessed by observing the appearance of the fracture line, callus formation, bridging of the involved cortex, and overall fracture healing. At all time points, the degree of articular surface collapse at the center of the main fracture fragment was measured on coronal CT scans. The measurement of articular surface collapse was defined as the distance from the plane of the intact tibial articular surface (parallel to the femoral condyles) to the point of maximum articular collapse (Figure 4). Bone defect healing at the bone graft site was evaluated according to the following criteria: no visible signs of bone remodeling, initial bone remodeling with periosteal bridging, bone remodeling with non-oriented trabecular structure, or complete bone remodeling with oriented trabecular structure. On non-weight-bearing follow-up CT, osteoarthritis was assessed based on the presence of one or more of the following features: joint space narrowing, subchondral sclerosis, subchondral cystic changes, or articular surface erosion.

Figure 4 Preoperative coronal CT reconstruction measuring articular surface depression. A line parallel to the femoral condyle is translated distally along a line C, which is perpendicular to the plane of the intact tibial articular surface (B), to measure the distance to the point of maximum articular collapse (dotted line A).
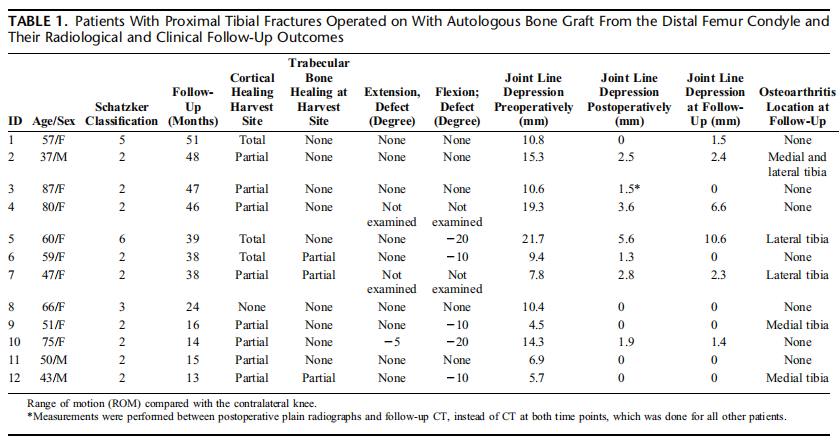
At follow-up, patient-reported function was assessed using the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the Lower Extremity Functional Scale (LEFS) (Table 1). During outpatient visits, a brief history was recorded, with specific inquiry about tenderness at the distal femoral bone graft site. Pain, range of motion, and ligament stability of both the affected and contralateral knee joints were examined, along with performing Apley's test and McMurray's test.
Between 2012 and 2018, 23 patients were continuously treated using the aforementioned technique. Among them, 14 patients had a possible follow-up period exceeding 12 months and were invited for follow-up. Of these 14 patients, 12 underwent at least one year of postoperative radiological follow-up at the time of data collection (Table 1). Ten patients underwent clinical examination, and eight completed the KOOS and LEFS assessments. The remaining two patients did not respond to the follow-up invitation.
At the time of injury, the median age of the patients was 58 years.The median of articular surface collapse was 10.5mm preoperatively and 1.4mm postoperatively.When comparing the postoperative and final follow-up CT scans, joint surface collapse exceeding 2mm was observed in two patients (Table 1). The preoperative joint surface collapse in these two patients was approximately 2cm each, with one of the patients being 80 years old (Table 1).
Postoperative CT showed no signs of cortical or articular penetration in the drill channels at the bone harvesting sites.One bone harvesting site showed no signs of cortical healing, eight sites showed partial cortical healing, and three sites showed complete cortical healing. At follow-up, compared to the immediate postoperative CT, nine patients showed no signs of trabecular healing or increased resorption at the femoral condyle bone harvesting site, while three patients showed partial trabecular healing (Figure 5). Follow-up CT showed that the fracture lines of five fractures were no longer visible, while the remaining fractures showed sclerotic or blurred fracture lines in most areas of the fracture system. All fractures demonstrated minimal periosteal callus formation, and all involved cortices were bridged, indicating fracture healing. The median difference in articular surface collapse between follow-up and postoperative measurements was 0.0 mm. Radiographic signs of osteoarthritis were observed in five patients (one with involvement of both joint compartments, two with lateral compartment involvement, and two with minor signs in the medial tibial condyle). One patient underwent total knee arthroplasty four years after the fracture due to post-traumatic osteoarthritis. No pathological changes related to the bone harvesting procedure were detected in the femoral condyles.
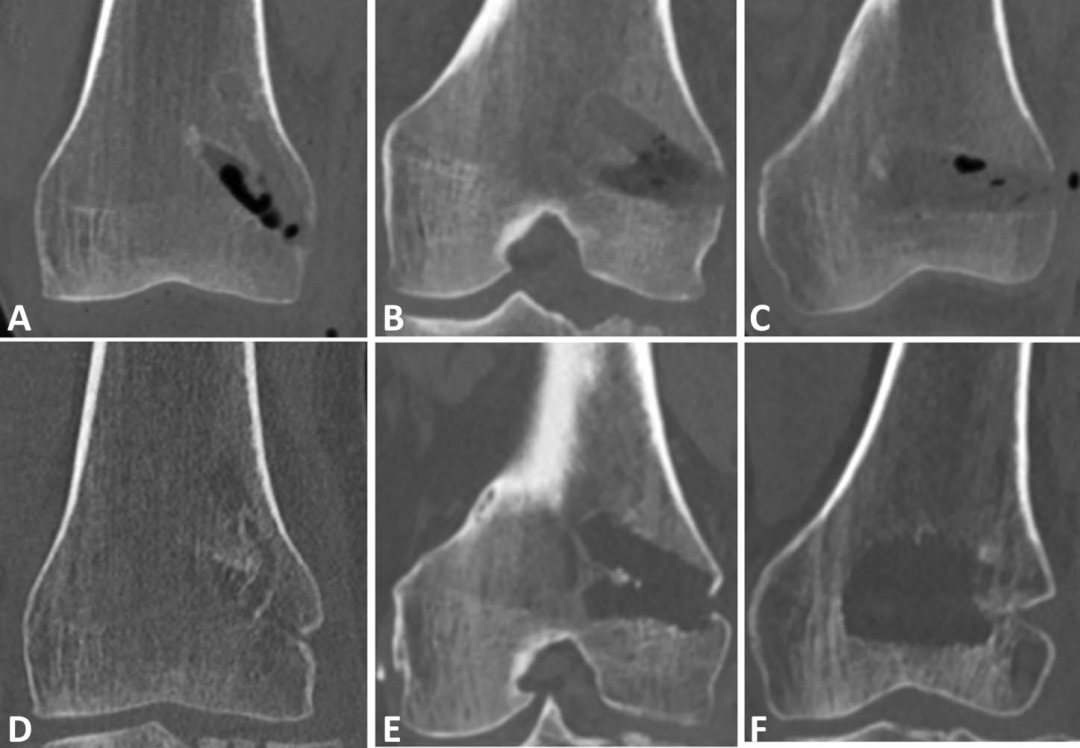
Figure 5 Comparison of bone harvesting site healing (Postoperative CT and Follow-up CT): A, B, C are postoperative CT, D, E, F are follow-up CT. A, D show metaphyseal remodeling at 13 months follow-up (Case 12). B, E show no remodeling at 48 months follow-up (Case 2). C, F show a larger metaphyseal defect at 15 months follow-up compared to postoperative CT (Case 11).
No patients complained of pain at the bone harvesting site, and there were no signs of direct neurovascular injury related to the bone harvesting procedure.One patient experienced sensory disturbance on the anterolateral side of the calf, and one patient experienced plantar sensory disturbance. One patient with a Schatzker type 6 fracture underwent fasciotomy during initial external fixation. During secondary plate fixation, skin grafting was performed on the fasciotomy wound, which healed well. In the KOOS scoring, the median for pain was 96; the median for symptoms was 90; the median for activities of daily living was 92; the median for sports and recreation was 44; and the median for quality of life was 53. In the KOOS scoring, 0 represents the worst outcome and 100 represents the best outcome. The median LEFS score was 59. In the LEFS scoring, 0 is the worst outcome and 80 is the best outcome.
Through the existing incision when treating proximal tibial fractures, using a drill to harvest cancellous bone grafts from the femoral condyle can provide sufficient bone volume to support the reduced articular fragments without posing risks of perioperative or long-term complications. Our research shows that patients treated with this technique exhibited good radiological and clinical outcomes at mid-term follow-up, similar to the results reported in previous studies using the traditional cortical bone window technique. The volume of harvested cancellous bone was approximately 20cc, which, although not precisely measured, is comparable to the harvest volumes from other donor sites.
Autologous bone grafting has been successfully applied in the reconstruction of fracture-related bone defects, but it also carries risks and complications, especially when bone is harvested from the iliac crest. Advances in the pharmaceutical industry have shown that calcium phosphate-based bone substitutes can serve as treatment options. However, these formulations may be expensive.
Advantages of using the distal femoral condyle as a bone graft site include: the surgical incision is located within the surgical area of fracture fixation, without traversing any muscular planes or areas of significant sensory nerve innervation. Due to minimal tissue retraction required, the incidence of postoperative pain and chronic pain syndrome is also lower. Bleeding complications, hematomas, nerve injuries, or iatrogenic supracondylar femoral fractures appear to be uncommon.Currently, we have used this technology to treat more than 50 patients and for other indications. Consistent with other reports using similar techniques, we did not observe any acute femoral fractures or stress fractures. A biomechanical study on composite femur models showed that no fractures occurred when supraphysiological loads were applied after creating a cortico-cancellous bone defect (3-24 cm) in the medial femoral condyle, further confirming the safety of the distal femur as a donor site.Our technique is slightly different from others using the cortical bone window technique, potentially more minimally invasive, thus reducing the risks of infection, bleeding, and postoperative pain.
According to the KOOS and LEFS assessments, there is a significant discrepancy in patients' self-perception of treatment outcomes. However, the higher median scores indicate that knee function in daily activities is acceptable for the patients. The results of this technique are consistent with previous studies, which show that joint recovery is positively correlated with higher KOOS scores and lower pain scores. Nevertheless, patients' quality of life may still be limited due to difficulties in completing physical activities, as restrictions in leisure activities appear to be relatively common. These limitations in quality of life and physical activities are well-known long-term complications of proximal tibial fractures and are unlikely to be related to bone grafting surgery. Previous studies have shown no significant difference in long-term pain scores (VAS) between patients undergoing autologous bone graft surgery and those treated with calcium sulfate bone cement. It is important to note that age has been found to be independently associated with pain and disability in various components of the KOOS score. Similarly, age is also significantly correlated with the LEFS score; the median LEFS score in our study is similar to the standard score for healthy populations aged 65 and above.
Previous case reports have shown that, in addition to tibial plateau fractures, the distal femur as a site for cancellous bone graft harvesting also has potential in the treatment of other conditions, including reconstruction after intralesional excision of talus chondroblastoma, tibial nonunion, and patellar reconstruction. This study has a small sample size and no control group, so it is unable to be compared with other established methods.
The results show that this technique has a success rate similar to other reported alternative methods and no severe complications occurred. We will continue to use this technique for obtaining autogenous bone grafts from the distal femur to assist in treating proximal tibial fractures. Future research should further explore the application of distal femoral grafts and evaluate the possibility of using the femoral condyle as a source for autogenous bone grafts in other indications.
Scan to Add
Orthopedic Assistant
Join the Academic Exchange Group


Submission Content
The themes of the call for papers are diverse, including but not limited to the latest research progress, achievements of scientific research teams, clinical medication experiences, in-depth analysis of typical cases, and practical experiences in disease diagnosis and treatment.
Submission Method
Submission WeChat: Mr. Gao 17611707166
Submission Email: gujinzw@163.com
Academic Promotion and Business Cooperation: Ms. Zhan 18612896281
Statement:The information in this article cannot replace professional medical guidance in any way, nor should it be regarded as clinical advice. It is for reference by medical professionals only and does not represent the views of the Gujinzhongwai platform. Readers are encouraged to make rational judgments and apply the information in a targeted manner.Please contact to delete if there is any infringement.