
H&H Healthcare
R&D and Producer of Interventional Medical Devices for Heart Disease

IntroductionIntroduction
Endovascular repair has been routinely used for the treatment of thoracoabdominal aortic diseases, with some patients' lesions involving important visceral branch arteries.The distance between the mouth is too short, requiring reconstruction of the blood supply. The fenestration technique is one of the commonly used methods for revascularization and is divided into in vitro pre-fenestration and in-situ fenestration. The main difficulty of the in vitro fenestration technique lies in the precise alignment of the window with the target artery, ensuring no forward jumping, backward movement, or rotation during stent deployment; the main challenge of in-situ fenestration lies in smoothly reaching the fenestration site and achieving high-quality fenestration, that is, forming the optimal fenestration angle (90°).
HuiHe Healthcare Fully Independent Research and DevelopmentS-wan Bipolar Adjustable SheathIt is currently the only sheath tube with dual-point bending control function in the same plane in China. It can easily adjust the bending angle, stably deliver instruments to the target point, help doctors improve surgical efficiency and reduce surgical complexity, and easily complete complex operations such as fenestration, mountain flipping, and branch artery superselection.
Recently, the Second Affiliated Hospital of Nanchang UniversityProfessor Zhou WeiminHighly appreciated after using Swan for in-situ fenestration and super-selective branch artery catheterization: S-wan, in addition to its unique S-shaped dual-point bending control function, also features excellent maneuverability and support performance. While ensuring surgical safety, it also improves operational efficiency. HuiHe Healthcare has created another outstanding product!
Case 1
Case One
· Basic Information
Patient:Male, 49 years old.
Chief Complaint:Sudden tearing-like pain in the chest and back for more than 10 days.
· Preoperative Diagnosis
Aortic dissection aneurysm, hypertension grade 2, varicose veins of the lower extremities.
· Surgical Plan
Thoracic Aortic Branched Stent Graft Implantation + Left Subclavian Artery In-situ Fenestration and Stent Implantation + Left Subclavian Artery Balloon Angioplasty.
Functions Achieved by S-wan Bipolar Steerable Sheath:Precise Angle Adjustment and Positioning of In-situ Fenestration in Left Subclavian Artery, Supporting Delivery Balloon and Stent and Other Instruments.
· Surgical Procedure
Puncture to establish access and preoperative angiography
STEP1. Puncture the right femoral artery, pre-place two suture devices (ProGlide), then insert an 8F sheath for backup. Import the yellow-label catheter and perform angiography at LAO50° above the aortic arch, which shows: dissection visible in the aorta, with the dissection extending to the distal end of the subclavian artery, approximately 1 cm away from the left subclavian artery and the left common carotid artery.
Implantation of Aortic Stent
STEP2. Replace the right femoral artery with a 24F-33CM Swift Lead vascular sheath, introduce the AnkuraII aortic covered stent system (TAA3022B20) along the super-hard guidewire to the ascending aorta, position it at the posterior edge of the left common carotid artery under fluoroscopy, and release after precise positioning.

In-situ Fenestration of the Left Subclavian Artery
STEP3. Under direct vision, puncture the lateral humeral artery, insert the Amplatz guidewire, and place it.S-wan (8F*55mm) Bipolar Adjustable Sheath Catheter (HuiHe Healthcare)Reaching the root of the left subclavian artery, used for adjusting the fenestration angle and instrument delivery.
STEP4. Adjust the S-wan bipolar steerable sheath to achieve perpendicular contact of the fenestration device tip with the stent. After confirming accurate positioning, perform in-situ fenestration of the aortic stent graft at a vertical angle.

STEP5. After the membrane rupture, under the guidance of the guidewire, sequentially introduce the MUSTANG (4.0*40mm) balloon, (6.0*40mm) balloon, and EverCross 8.0*60mm balloon catheter to dilate the fenestration site of the thoracic aortic stent (left subclavian artery branch).
Left Subclavian Artery Stent Implantation
STEP6. Import one vascular covered stent (FVL10040, Bard) and precisely release it under fluoroscopy. Subsequently, import a MUSTANG (10*40mm) balloon for post-dilation. Angiography indicates that the left subclavian artery is patent.
Postoperative Angiography
STEP7. Angiography with a pigtail catheter above the aortic arch showed: accurate stent positioning, completely covering the rupture; the three branches above the aortic arch were patent; there was an endoleak between the stent and the aorta, but no contrast agent extravasation. The catheter and guidewire were withdrawn, the suture of the right femoral artery was tightened, and the left brachial artery and the skin at the left elbow fossa were sutured.
Summary
The in-situ fenestration technique for aortic arch lesions remains highly challenging. The alignment of the in-situ fenestration with the ostium of the branch arteries requires skill, and places high demands on the operator's technique as well as the fenestration equipment. The main clinical pain points of this case of thoracic aortic stent in-situ fenestration are as follows:
Angle:The angle at which the LSA arises from the aortic arch is relatively sharp and tortuous, especially for vessels with an angle of less than 30°, making it difficult to achieve a satisfactory puncture angle. This can lead to consequences such as main stent displacement, vascular injury, and poor fenestration quality.
Damage:Vessel tortuosity and complex variations make it difficult to achieve a perpendicular puncture angle, hard to precisely control the puncture depth, and mis-puncture can cause vascular injury;
Support:The high blood pressure in the aortic arch and the high-speed impact of blood flow make it difficult to accurately position the covered stent during release, and the branch stent is also challenging to precisely position.
The distal end of the S-wan bipolar adjustable sheath can be controlled to form an S-shaped curve, allowing for perpendicular fenestration even in target vessels with angulation below 30°, reducing the risk of vascular injury. Additionally, when the sheath is curved into an S-shape to support the vessel, it provides extra support to ensure stable delivery of fenestration devices, minimizing the risk of slippage or displacement of therapeutic instruments, thereby improving surgical efficiency and safety.
Single-bend Sheath Difficult to Adjust Angle for Vertical Fenestration VS S-bend Sheath Adjust Angle for Vertical Fenestration
Case 2
Case Two
· Basic Information
Patient:Male, 65 years old.
History of Present Illness:Abdominal aortic aneurysm found 4 days ago.
· Preoperative Diagnosis
Abdominal aortic aneurysm, hypertension grade 2, chronic renal insufficiency.
· Surgical Plan
Endovascular Repair of Abdominal Aortic Aneurysm with Stent Graft + Renal Artery Stent Placement + Iliac Artery Stent Graft Placement.
S-wan Bipolar Adjustable Bend Sheath Functionality:Precisely super-select the left renal artery at the optimal angle, ensuring stable support for instrument delivery and release.
· Surgical Procedure
Puncture to establish access and preoperative angiography
STEP1. After puncturing the bilateral common femoral arteries, pre-place 6F vascular sheaths, reserve 2 sutures, replace with a 14F sheath, and inject heparin. High-pressure angiography shows: The infrarenal abdominal aorta is basically normal, and the aneurysm neck is less than 1 cm.
STEP2. In vitro release of the large artery stent graft system (XJZD24080): Pre-open bilateral renal artery windows, then retrieve and introduce the stent delivery system below the superior mesenteric artery level; deploy the stent in a constrained diameter mode.
STEP3. Through the right brachial artery approach, sequentially introduce a 4mm*40mm EverCross balloon catheter to dilate the bilateral pre-opened renal artery windows, and fully release the aortic stent graft system (XJZD24080).
STEP4. Through the right arterial approach, the peripheral self-expanding stent system (PRP35-06-040-120, ev3) was introduced and accurately deployed in the right renal artery.
STEP5. The left femoral artery was replaced with a Swift Lead 18Fr*33cm, and a steerable sheath (SVA6F-550) was introduced. After successfully selecting the left renal artery using a single-curve catheter with a guidewire, the guidewire was replaced with an Aplatz guidewire. Subsequently, a 0mnilink Elite (7mm*29mm) was introduced and precisely deployed.
STEP6. Import the Ankura Aortic Stent Graft System (XJZDF30120) below the level of the bilateral renal arteries and accurately deploy the stent. Angiography confirms the patency of the bilateral renal arteries.
STEP7.The Yuranos abdominal aortic stent graft system (IE-1414-080) was advanced along the guidewire in sequence and docked with the main body, with the distal end of the stent positioned in the left common iliac artery. The long leg of the main body stent was fully deployed, followed by the connection of the Yuranos abdominal aortic stent graft system (IE-1412-080), which was docked with the main body, and the distal end of the stent was positioned in the right common iliac artery.
STEP8.The compliant balloon was used to dilate the proximal end of the stent and the overlapping section of the stent. Final angiography showed: poor visualization of the left renal artery, but clear visualization of the mesenteric and right renal arteries; the stent was well-expanded with accurate placement, and no contrast leakage was observed.
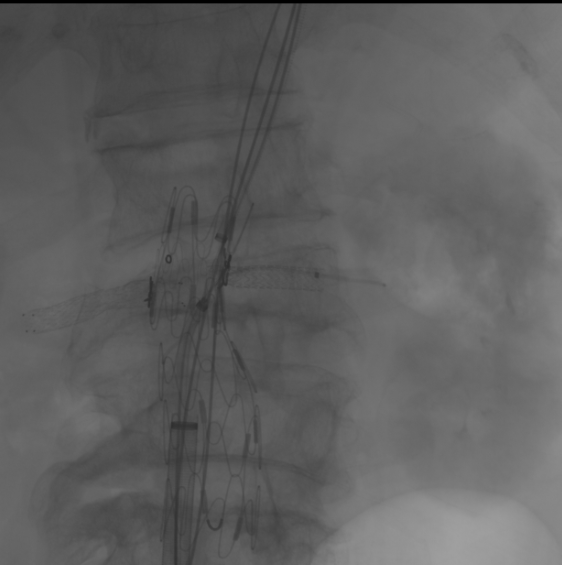
STEP9.Through the left femoral artery approach, a steerable sheath (SVA6F-550) was introduced and used in conjunction with a mucus catheter, but multiple attempts still failed to successfully super-select into the left renal artery.


STEP10.Later ReplacementS-wan (6F*55mm) Bipolar Adjustable Sheath Catheter (HuiHe Healthcare), Adjust the S-bend angle and provide stable support. After smoothly selecting the left renal artery with the adjustment of the mudskipper, introduce the Amplatz guidewire, then introduce the peripheral self-expanding stent system (PRP35-06-040-120) into the left renal artery. The stent was successfully placed after precise positioning. Angiography showed improved visualization of the left renal artery compared to before.
Summary
S-wan Bipolar Adjustable Bend Sheath, as the first S-shaped bend sheath, has the following characteristics when used in super-selective branch arteries:
S-shaped bidirectional bend:Adjustable S-bend reduces bending radius, suitable for target vessels with smaller diameters or forming acute angles with main vessels, as well as other tortuous and complex vascular interventional scenarios;
Super Selective Freedom:S-wan Tip 0-270° Adjustable, with Dual Curved Ends for Different Vessel Morphologies, Diameters, and Superselective Catheterization of Intraluminal Arteries or Carotid Arteries; Features Flexible Control and High Success Rate in Superselection.
Strong Support:S-wan features its self-developed FREEKNIT variable knitting technology, providing strong support through the instrument while ensuring the sheath does not rebound.
This case involves stenosis at the origin of the left renal artery. The S-wan bipolar steerable sheath was used to achieve a precise entry angle into the renal artery ostium, reducing the time required to identify the target vessel's origin and direction. It also provided stable support for stent delivery, enhancing operational safety and procedural efficiency, significantly lowering the difficulty of super-selective catheterization, and playing a pivotal role in the success of the surgery.
S-Wan Different Bend Types Coordination Diagram
Expert IntroductionExpert Introduction

Zhou WeiminProfessor
The Second Affiliated Hospital of Nanchang University
Swipe up to view
Professor, Chief Physician, Doctor of Medicine
Ph.D. Supervisor and Master's Supervisor
Director of the Department of Vascular Surgery, Second Affiliated Hospital of Nanchang University
Director of the Peripheral Vascular Intervention Training Base (Jiangxi) Office, National Health Commission
Standing Committee Member of the Vascular Surgery Group, Surgery Branch, Chinese Medical Association
Standing Committee Member of the Vascular Surgery Expert Committee, Cross-Straits Medical and Health Exchange Association
Standing Committee Member of the Vascular Disease Professional Committee of the Chinese Society of Microcirculation
First Standing Committee Member of the Interventional Medicine Professional Committee of the Chinese Research Hospital Association
National Committee Member of the Vascular Surgery Professional Committee and Standing Committee Member of the Hemodialysis Access Group, China International Exchange and Promotive Association for Medical and Health Care
National Committee Member of the Vascular Expert Committee of the Geriatric Medicine Committee of the Chinese Gerontology Society
National Committee Member of the Endovascular Surgery Professional Committee of the Chinese Medical Doctor Association and Member of the Aortic Dissection Expert Committee
Chairman of the Vascular Surgery Group, Surgery Branch, Jiangxi Medical Association
Chairman of the First Committee of the Vascular Medicine Branch of Jiangxi Province Research Hospital Association
Vice President of the First Sino-Japanese Medical Exchange Association, Vascular Surgery Branch
Principal Investigator of 3 National Natural Science Foundation projects and 3 provincial major research projects, with over 140 academic papers published, including more than 40 SCI-indexed papers (the highest single-article impact factor being 41.787). Recipient of 6 provincial science and technology progress awards, contributor to 11 guidelines and expert consensus documents, and mentor to over 40 doctoral and master’s students. Recognized as a leading mid-career expert in Jiangxi Province’s healthcare sector for outstanding contributions, and ranked among the top 50 vascular surgery experts in China in 2021. Specializes in the diagnosis, surgical treatment, and minimally invasive therapy of complex and difficult vascular surgical diseases, having led over 5,000 complex vascular surgeries. Editorial board member and special review expert for several core journals, including the Chinese Journal of Vascular Surgery, and SCI journals. Executive Chair of the 15th National Academic Annual Conference on Vascular Surgery of the Chinese Surgical Association. Has visited and studied at multiple medical centers in Germany, the United States, Japan, Singapore, and Taiwan, China.

Zeng QingfuProfessor
The Second Affiliated Hospital of Nanchang University
Nanchang University Second Affiliated Hospital, Department of Hematology, Associate Chief Physician
M.D., Master's Supervisor
Winner of the National Clinical Skills Competition
Member of the Youth Expert Committee, China Branch, International Vascular Union
Standing Committee Member of the Vascular Surgery Branch of Jiangxi Province Medical Association
Standing Committee Member and Secretary of the Vascular Medicine Specialized Committee of the Research-Oriented Hospital Association

Xu YingqiProfessor
The Second Affiliated Hospital of Nanchang University
The Second Affiliated Hospital of Nanchang University
Vascular Surgery, Attending Physician, Doctor of Medicine
University Lecturer
Youth Committee Member of the Vascular Medicine Branch of Jiangxi Province Research Hospital Association
Member of the Vascular Surgery Physician Branch of the Jiangxi Province Medical Association
Young Committee Member of the International Vascular Union

Fang HuaqiangProfessor
The Second Affiliated Hospital of Nanchang University
The Second Affiliated Hospital of Nanchang University
Vascular Surgery, Attending Physician, Doctor of Medicine
Capable of comprehensive diagnosis and treatment of common peripheral vascular diseases
Published multiple SCI and Chinese papers in recent years.
Participated in multiple national and provincial/ministerial level research projects
Shanghai Huihe Healthcare Technology Co., Ltd.
Official Account:HuiHe Healthcare
Email:question@hh-healthcare.com
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints; it is solely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is intended exclusively for healthcare professionals to stay informed and should not replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and the authors assume no related responsibility.Contact Email for Cooperation:vascular@edoctor.work。
