GPRC5D/BCMA/CD3 Trispecific Antibodies Make Waves Again: Simcere Goes Global, and MBS314 by Betta Pharmaceuticals & ConYBio Achieves 100% ORR in High-Dose Cohort

Simcere
Innovative Drug Developer

Johnson & Johnson
Medical Device R&D and Manufacturer
▎Traceability
On January 13, 2024, Simcere and AbbVie jointly announced that they had reached a licensing option agreement regarding SIM0500, a drug candidate under development by Simcere Zaiming. Simcere Zaiming will receive an upfront payment from AbbVie, as well as optional rights payments and milestone payments totaling up to $1.055 billion. Additionally, Simcere Zaiming will receive tiered royalties based on the net sales of the product outside the Greater China region. AbbVie is entitled to collect tiered royalties based on the net sales in the Greater China region.
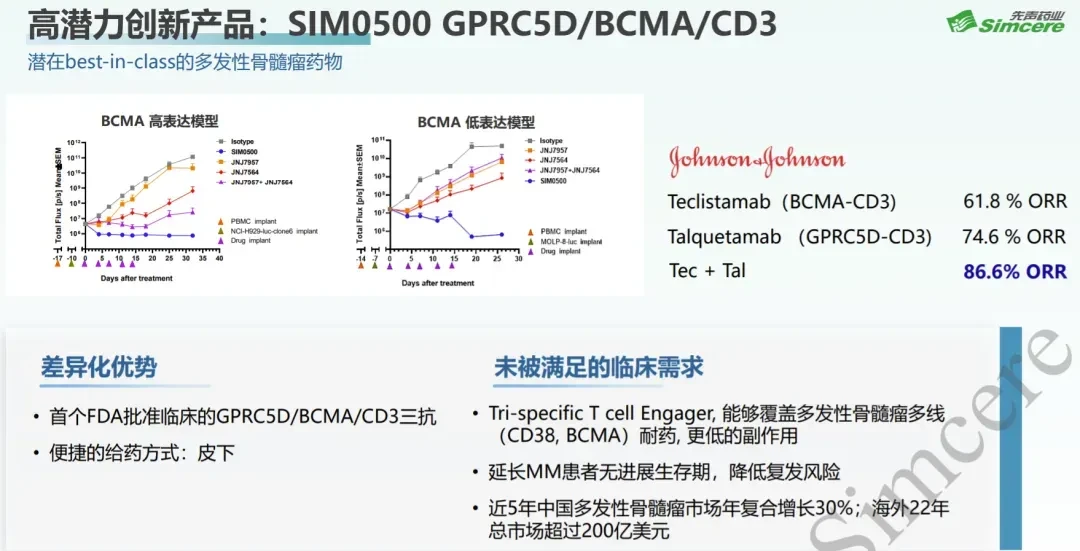
SIM0500 is a humanized GPRC5D-BCMA-CD3 trispecific antibody. This molecule combines a low-affinity yet highly targeted activating CD3 antibody, along with two tumor-associated antibodies: anti-G protein-coupled receptor class C group 5 member D (GPRC5D) and anti-B cell maturation antigen (BCMA). Preclinical data indicate that SIM0500 demonstrates significant advantages compared to JNJ-7957 (Teclistamab, BCMA/CD3) and JNJ-7564 (Talquetamab, GPRC5D/CD3), whether used as monotherapy or in combination.
Currently, SIM0500 has not been disclosed publicly, and AbbVie's introduction of the drug to some extent indicates its positive efficacy.
GPRC5D and BCMA exhibit non-complete correlation in their expression in tumors. Multi-specific antibodies targeting both GPRC5D and BCMA can cover patients with GPRC5D-positive tumors as well as those with BCMA-positive tumors, while avoiding recurrence caused by the loss of a single antigen, thereby increasing patient coverage and improving treatment efficacy. This is the rationale behind the current development of GPRC5DxBCMAxCD3 trispecific antibodies.
Johnson & Johnson has conducted clinical exploration on the combination of the two, and preclinical data show that JNJ-7957 and JNJ-7564 have strong combined advantages.
On January 9, 2025, Johnson & Johnson published the article "Talquetamab plus Teclistamab in Relapsed or Refractory Multiple Myeloma," presenting the clinical treatment outcomes of Talquetamab combined with Teclistamab. The data is positive.
'%20fill='%23FFFFFF'%3E%3Crect%20x='249'%20y='126'%20width='1'%20height='1'%3E%3C/rect%3E%3C/g%3E%3C/g%3E%3C/svg%3E)
116 patients were screened, and ultimately 94 patients were enrolled in the clinical trial to evaluate different dose levels of bispecific antibody combination therapy. Five dose levels were designed, with talquetamab, 0.8 mg/kg, plus teclistamab, 3.0 mg/kg, Q2W as the RP2D (recommended phase 2 dose).
Enrollment: The median age of patients across all dose groups was 64.5 years, with a median time of 6.1 years post-diagnosis, and they received a median of four treatment cycles. All patients had been treated with three classes of drugs, and the majority (65%) had received five classes of drugs. Seven patients had been treated with bispecific antibodies, and four patients had undergone CAR T-cell therapy. A total of 87 patients (93%) had disease refractory to their last treatment, and 81 patients (86%) had disease refractory to all three drug classes. Extramedullary disease was present in 34 patients (36%), and 21 of 51 patients (41%) exhibited high-risk cytogenetic features.
Safety:Three patients experienced dose-limiting toxicity (including one patient who developed grade 4 thrombocytopenia at the recommended phase 2 dose). The most common adverse events across all dose levels were cytokine release syndrome, neutropenia, dysgeusia, and non-rash skin reactions. Grade 3 or 4 adverse events occurred in 96% of patients, most of which were hematologic events.64% of patients developed grade 3 or 4 infections.When the recommended Phase 2 regimen was used, 80% of patients exhibited a treatment response (including 61% of patients with extramedullary disease).Cytokine release syndrome occurred in 74 patients (79%). Most events were grade 1 or 2, occurring during the step-up phase and early cycles of treatment; two patients (2%) experienced grade 3 cytokine release syndrome. Cytokine release syndrome led to cycle delays or dose adjustments in 14 patients (15%).
Efficacy:Under the recommended dose regimen in Phase 2, 35 of 44 patients (80%) exhibited a treatment response, with a median time to first response of 1.4 months (range: 0.3 to 5.1 months). A total of 34 patients (77%) achieved a very good partial response or better, and 23 patients (52%) achieved a complete response or better.Using the recommended Phase 2 regimen, high response rates were observed across multiple clinically relevant subgroups, including patients with International Staging System Stage III multiple myeloma (7 of 8 patients [88%]), patients who had received three or more prior lines of therapy (29 of 38 patients [76%]), patients with high-risk cytogenetic features (6 of 8 patients [75%]), and patients with extramedullary disease (11 of 18 patients [61%]).
Talquetamab and TeclistamabThe combination therapy achieved very excellent preliminary efficacy, but the incidence of treatment-related grade 3 or 4 infections was higher than that of using either treatment alone.
MBS314, co-developed by Tian Guang Shi and Kang Yuan Bo Chuang in China, is a novel trispecific antibody targeting CD3/BCMA/GPRC5D for the treatment of multiple myeloma. It is currently in Phase I clinical trials and has demonstrated excellent efficacy and safety both preclinically and clinically.
The molecular design is 1:1:1, with the CD3 antibody recognizing the CD3δ and CD3ε complex. The affinities of the BCMA and GPRC5D antibodies are -10 and -9, respectively. At the cellular level, both BCMA and GPRC5D antibodies exhibit better binding, especially the GPRC5D antibody.
Showed excellent efficacy in in vivo models, demonstrating better therapeutic effects compared to combination therapy. This is consistent with Simcere.SIM0500 shows similar in vivo efficacy, which means that this class of tri-specific antibodies has reproducible efficacy.
Roche presented their research at the 2023 ASH meeting, showing that in patients with relapsed/refractory multiple myeloma (RRMM), double and triple-negative (targeting GPRC5D, BCMA, and FcRH5) MM precursor cells (MMPCs) are relatively rare. The heterogeneity arises from the variability in expression of myeloma cells among individuals, which is also a key reason why multi-target antibodies achieve better efficacy. Importantly, the activation of CD3 has little correlation with antigen expression levels, which explains why low-expression antigens like DLL3 can still be druggable, and the same applies to GPRC5D. However, the presence of BCMA may compensate for the insufficient efficacy caused by low or absent GPRC5D expression, a critical factor behind the excellent efficacy of GPRC5D/BCMA/CD3. As shown in Figure 7A below, GPRC5D and BCMA together account for nearly 100% of the expression, with only differences in which one is more highly expressed.
Based on current clinical data, in the high-dose group, MBS314 achieved a 100% response rate in 3 patients, with two cases of confirmed CR (complete response), and the PR was VGPR (very good partial response), close to complete response. One of these patients had previously received CAR-T BCAM treatment. No dose-limiting toxicity has been observed so far.
And the safety profile shows very good advantages compared to刚才Talquetamab and TeclistamabCombination TherapyGrade 3 or Grade 4 infectionUp to 64%, andThe infection rate of grade 3 or higher for MBS314 is only 14.3%. GPRC5D has a certain degree of targeted skin toxicity, but most cases are grade 1-2 toxicity.MBS314No toxicity of grade 3 or higher,Compared with Johnson & Johnson and Roche, it also shows better safety advantages. BCMA shares some targeted killing, while GPRC5D as a whole takes the dominant role in cytotoxicity.
Tri-specific CD3/BCMA/GPRC5D antibody demonstrates significantly superior preliminary efficacy data compared to bispecific antibodies or combination therapies with bispecific antibodies, particularly showing better safety than the combination therapies.
Innovative drugs have deepened industry understanding through gradual exploration.CD3/BCMA/GPRC5D May Lead the Next BD Trend, We Wait and See.
Warm Tips
Simple operation can star ⭐️ PharmaExpress, receive our push notifications in the first time.