Bispecific Antibodies, ADCs, and Combination Therapies Converge on SCLC: Innovations Highlighted Ahead of WCLC 2025

BioNTech
Developer of Novel Biologics

Amgen
Developer of Treatment Drugs for Serious Diseases

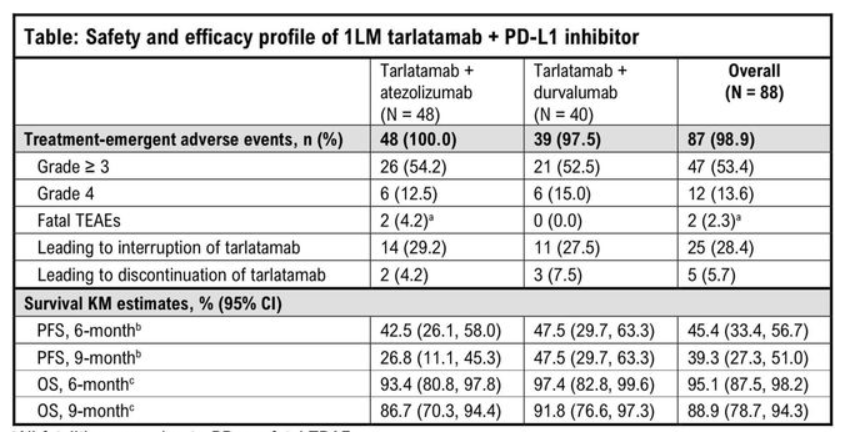
At last year's relevant conference, Amgen had already announced the preliminary efficacy of this therapy. As of May 31, 2024, a total of 88 patients had received treatment, with male patients accounting for 62.5% and a median age of 64.0 years. The median time from the start of first-line chemotherapy-immunotherapy to the start of first-line maintenance therapy was 3.6 months. The median PFS after the start of first-line maintenance therapy was 5.6 months. Due to insufficient follow-up time, the median OS has not yet matured, with an estimated 9-month OS rate of 88.9%. The DCR was 62.5%, and the median DoR was 9.3 months.
In the safety analysis, with a median follow-up of 10.0 months, no DLT occurred. The most common TEAEs of any grade were CRS (53.4%), dyspepsia (47.7%), and fatigue (34.1%). The most common TEAEs of grade ≥3 were hyponatremia (10.2%), neutropenia (6.8%), and anemia (6.8%). CRS primarily occurred during the first cycle, mostly grades 1-2, with one patient experiencing grade 3 CRS. Any-grade, grade 3, and grade 4 immune effector cell-associated neurotoxicity syndrome and related neurological events occurred in 11.4%, 2.3%, and 0% of patients, respectively.

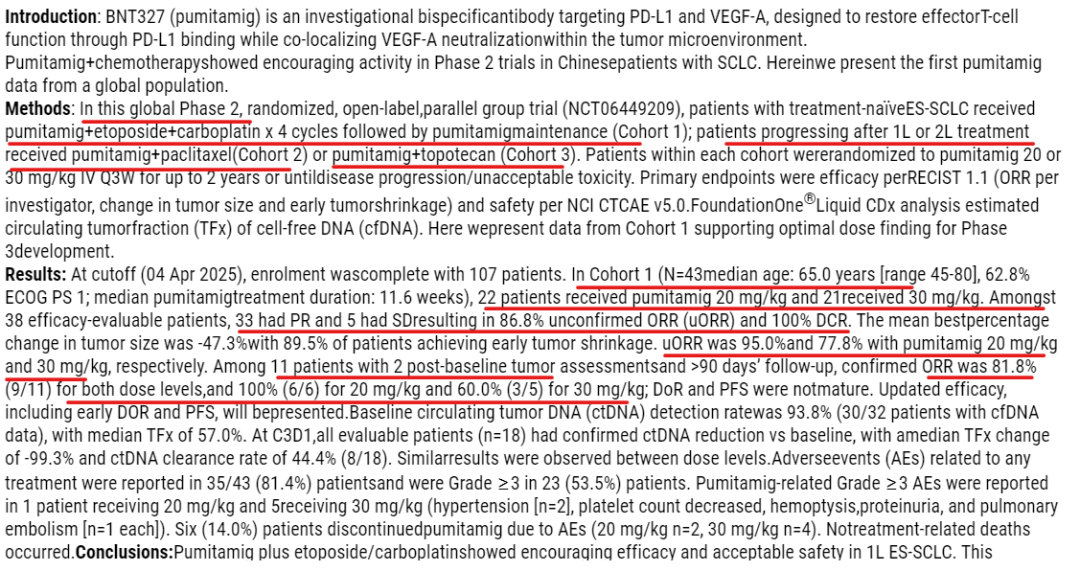
As of the cutoff date (April 4, 2025), 107 patients have been enrolled.In the first cohort(N=43, median age 65.0 years [range 45-80], 62.8% of patients with ECOG PS score of 1; median treatment duration of Pumitani 11.6 weeks)Twenty-two patients received 20 mg/kg of pimitanib, and 21 patients received 30 mg/kg. Among the 38 evaluable patients, 33 achieved partial response (PR), and 5 had stable disease (SD). The unconfirmed objective response rate (uORR) was 86.8%, and the disease control rate (DCR) was 100%.The average of the optimal percentage change in tumor size was -47.3%, with 89.5% of patients achieving early tumor shrinkage.The uORR for the 20 mg/kg and 30 mg/kg dose groups were 95.0% and 77.8%, respectively.InAmong 11 patients who completed two baseline tumor assessments and were followed up for >90 days, the confirmed objective response rate (cORR) was 81.8% (9/11) in both dose groups, with the 20 mg/kg group reaching 100% (6/6) and the 30 mg/kg group at 60.0% (3/5).; Duration of Response (DoR) and Progression-Free Survival (PFS) data are not yet mature. Updated efficacy data, including early DoR and PFS, will be disclosed subsequently.
The baseline circulating tumor DNA (ctDNA) detection rate was 93.8% (30 positive cases among 32 patients with cfDNA data), with a median tumor fraction (TFx) of 57.0%. On the first day of Cycle 3 (C3D1), all evaluable patients (n=18) showed a reduction in ctDNA from baseline, with a median TFx change of -99.3% and a ctDNA clearance rate of 44.4% (8/18). Results were similar across different dose groups.
Among 43 patients, 35 (81.4%) reported treatment-related adverse events (AEs) of any grade, including 23 (53.5%) with ≥Grade 3. Pumitanib-related ≥Grade 3 AEs were reported in 1 patient in the 20 mg/kg group and 5 patients in the 30 mg/kg group (hypertension [2 cases], decreased platelet count, hemoptysis, proteinuria, and pulmonary embolism [1 case each]). Six (14.0%) patients discontinued pumitanib due to AEs (2 in the 20 mg/kg group and 4 in the 30 mg/kg group). No treatment-related deaths occurred.
3)SHR-4849Is a DLL3 ADC independently developed by Hengrui with intellectual property rights. Its payload is a topoisomerase inhibitor (TOPOi). In December last year, HengruiLicensed to US-based IDEAYA Biosciences for over $1 billion in total,Hengrui Medicine-led Phase I Clinical Trial in China (NCT06443489) Demonstrates Significant Antitumor Activity in Small Cell Lung Cancer (SCLC) Treatment

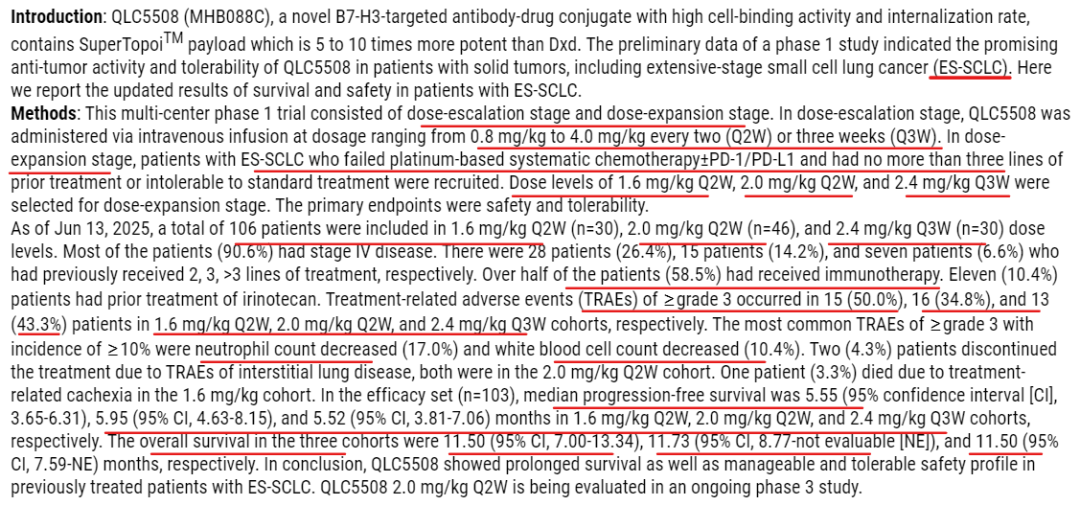
As of June 13, 2025, a total of 106 patients were enrolled at dose levels of 1.6 mg/kg Q2W (n=30), 2.0 mg/kg Q2W (n=46), and 2.4 mg/kg Q3W (n=30). The majority of patients (90.6%) were Stage IV. There were 28 patients (26.4%) who had received second-line treatment, 15 patients (14.2%) who had received third-line treatment, and 7 patients (6.6%) who had received more than third-line treatment. More than half of the patients (58.5%) had received immunotherapy. Eleven patients (10.4%) had previously been treated with irinotecan.
In terms of efficacy,The median progression-free survival for the 1.6 mg/kg Q2W, 2.0 mg/kg Q2W, and 2.4 mg/kg Q3W groups were respectively5.55 months, 5.95 months, and 5.52 months. The overall survival periods for the three cohorts were 11.50 months, 11.73 months, and 11.50 months, respectively.
In terms of safety, ≥3-grade treatment-related adverse events (TRAEs) occurred in 15 patients (50.0%), 16 patients (34.8%), and 13 patients (43.3%) in the 1.6 mg/kg Q2W, 2.0 mg/kg Q2W, and 2.4 mg/kg Q3W groups, respectively. The most common ≥3-grade TRAEs were decreased neutrophil count (17.0%) and decreased white blood cell count (10.4%). Two patients (4.3%) discontinued treatment due to interstitial lung disease, both from the 2.0 mg/kg Q2W group. One patient (3.3%) in the 1.6 mg/kg group died due to treatment-related cachexia.

On September 7, 2024, Merck announced the treatment of extensive-stage small cell lung cancer (ES-SCLC) patients with Ifinatamab deruxtecan (I-DXd).Phase II IDeate-Lung01 TrialThe positive results of the mid-term.
The research results showed that, in ES-SCLC patients treated with Ifinatamab deruxtecan, the objective response rates (ORR) for the 12mg/kg (n=42) and 8mg/kg (n=46) dose groups were54.8% and 26.1%; The median duration of response (DOR) was4.2 months and 7.9 months; Disease Control Rate (DCR) was90.5% and 80.4%; The median progression-free survival (PFS) was5.5 months and 4.2 months;The median overall survival (OS) was11.8 months and 9.4 monthsNotably, 12mg/kg was selected as the optimal dose for the expansion phase of the IDeate-Lung01 Phase 2 trial and the recently initiated IDeate-Lung02 Phase 3 study.
In the subgroup of patients with brain target lesions at baseline, assessed by central nervous system (CNS) BICR, in the 12mg/kg (n=10) and 8mg/kg (n=6) cohorts,The intracranial ORR was 50.0% and 66.7%, respectively.。
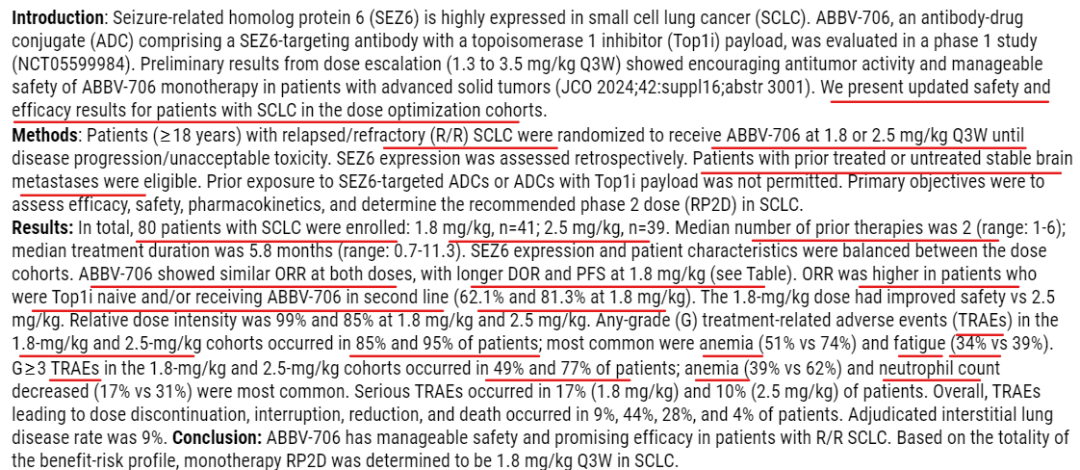
6)Phase I Study Results of ABBV-706 in Patients with Relapsed/Refractory (R/R) Small Cell Lung Cancer (SCLC)

Study Design:Patients with R/R SCLC aged ≥18 years were randomly assigned to receive ABBV-706 at doses of 1.8 mg/kg or 2.5 mg/kg (administered intravenously once every 3 weeks) until disease progression or intolerable toxicity. SEZ6 expression levels were assessed retrospectively. Patients with stable brain metastases, previously treated or untreated, were allowed to enroll, while those who had received prior treatment with SEZ6-targeted antibody-drug conjugates (ADC) or ADCs containing a topoisomerase I inhibitor (Top1i) payload were excluded. The primary study objectives included evaluating efficacy, safety, pharmacokinetics, and determining the recommended Phase II dose (RP2D) for the SCLC indication.
Research Results: A total of 80 SCLC patients were enrolled (41 in the 1.8 mg/kg group and 39 in the 2.5 mg/kg group). The median number of prior treatment lines was 2 (range: 1-6), and the median treatment duration was 5.8 months (range: 0.7-11.3). SEZ6 expression levels and baseline characteristics were balanced between the two groups.
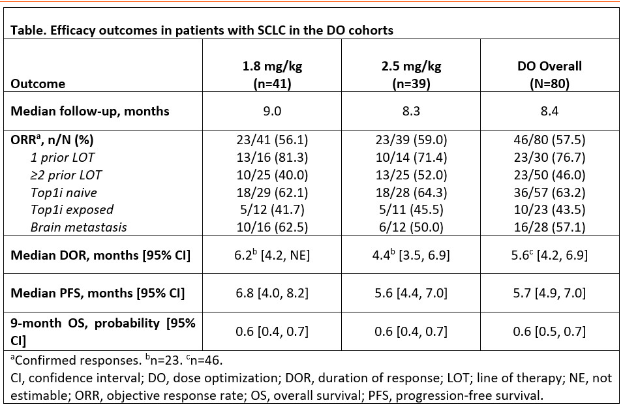
Objective Response Rate (ORR) Similar in Both Dose Groups, but the 1.8 mg/kg group had longer durations of response (DOR) and progression-free survival (PFS) (see attached table for details).InPatients who have not received Top1i treatment and/or used ABBV-706 as a second-line therapy showed a higher ORR (62.1% and 81.3% in the 1.8 mg/kg group, respectively).)
Safety Data: The 1.8 mg/kg group demonstrated superior safety.,All-grade treatment-related adverse events (TRAEs): 85% in the 1.8 mg/kg group and 95% in the 2.5 mg/kg group occurred, most commonly anemia (51% vs 74%) and fatigue (34% vs 39%). ≥Grade 3 TRAEs: 49% in the 1.8 mg/kg group and 77% in the 2.5 mg/kg group occurred, mainly anemia (39% vs 62%) and decreased neutrophil count (17% vs 31%). Severe TRAEs: 17% in the 1.8 mg/kg group, 10% in the 2.5 mg/kg group.Overall TRAEs Impact: The rates of discontinuation, interruption, dose reduction, and death were 9%, 44%, 28%, and 4%, respectively.Incidence of Interstitial Lung Disease:9%。

2023Year7Month12Date12Month6Day, Total Enrollment44Example patients, with a median age of63Years, Male Proportion84.1%(37/44). The median follow-up time was15.28Months.43In patients whose efficacy can be evaluated, observed37Partial Response Example (PR) and6Example: Disease stabilization (SD),ORRAndDCRRespectively86%And100%MedianPFSFor5.7Months(95%CI: 4.8-7.0)。MedianOSNot yet reached,15MonthsOSRate is63.5%。
Manageable Safety,40Example (90.9%) Patients experience ≥3LevelDuring treatmentCurrent adverse events (TEAEs), most common (≥20%)≥3LevelTEAEsIncluding decreased neutrophil count(65.9%), decreased white blood cell count (25.0%) and decreased platelet count (25.0%)。20Example (45.5%) The patient experienced immune-related adverse events (irAEs), where ≥3LevelirAEsIncidence rate is15.9%. No treatment-related deaths occurred.
References
WCLC Abstract and Related Company Disclosures


All articles reproduced in this official account are intended to convey more information, with the source and author clearly indicated. Media or individuals who do not wish to be reprinted may contact us (cbplib@163.com), and we will promptly delete the content. All articles represent the views of the author and do not reflect the position of this website.