Janssen's KLK2/CD3 Bispecific Antibody Pasritamig (JNJ-78278343) Advances to Phase III Clinical Trial in Metastatic Castration-Resistant Prostate Cancer

Johnson & Johnson
Healthcare Product Manufacturers, Health Service Providers
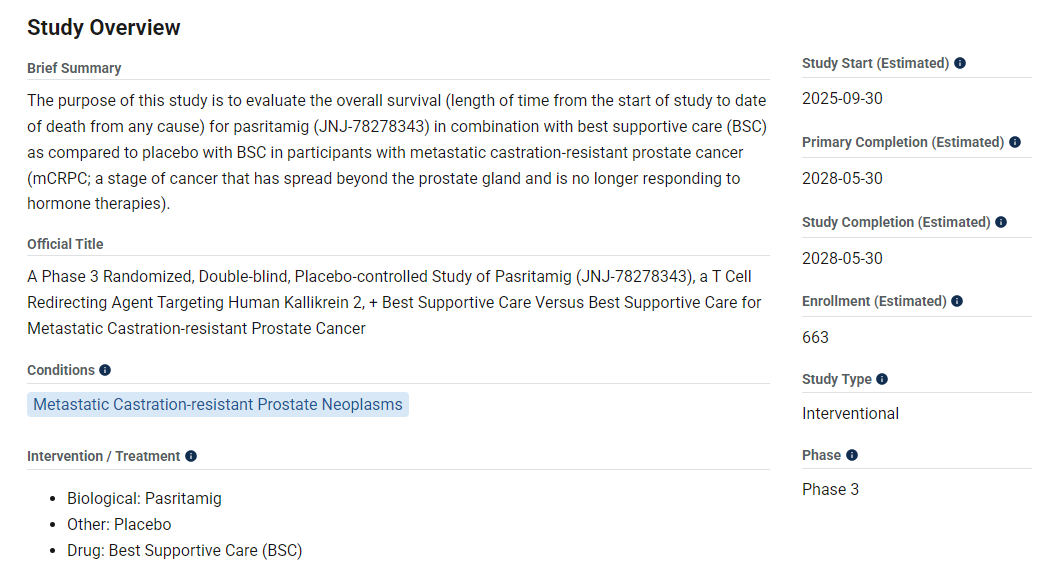
Recently,Under Johnson & JohnsonKLK2/CD3 Bispecific Antibody Pasritamig(JNJ-0815) registered a Phase III clinical trial (NCT07164443) on the website,Aimed to evaluateOverall Survival of the Drug Combined with Best Supportive Care (BSC) versus Placebo Combined with BSC in Patients with Metastatic Castration-Resistant Prostate Cancer (mCRPC)(OS)。This marks the official entry of Pasritamig into Phase III clinical development.
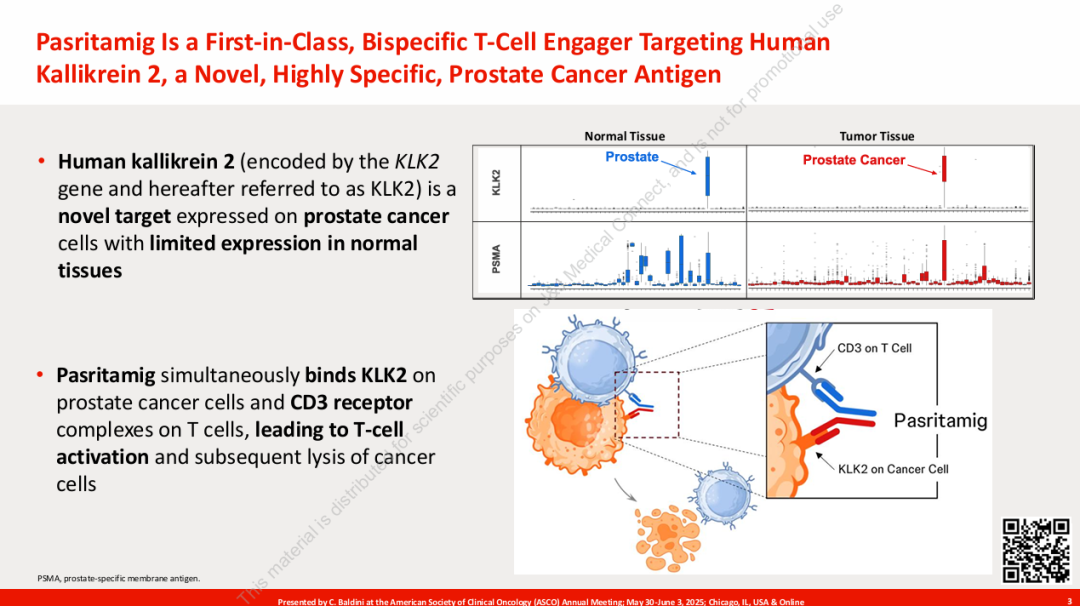
Human Kallikrein 2 (hK2), encoded by the KLK2 gene, is an androgen-regulated protease that is highly specifically expressed in prostate cancer tissues, particularly showing significant targeting potential in mCRPC.
Pasritamig adopts a symmetric 1+1 full-length antibody structure, which can simultaneously target KLK2 on the surface of tumor cells and CD3 on the surface of T cells, guiding T cells to kill tumors.
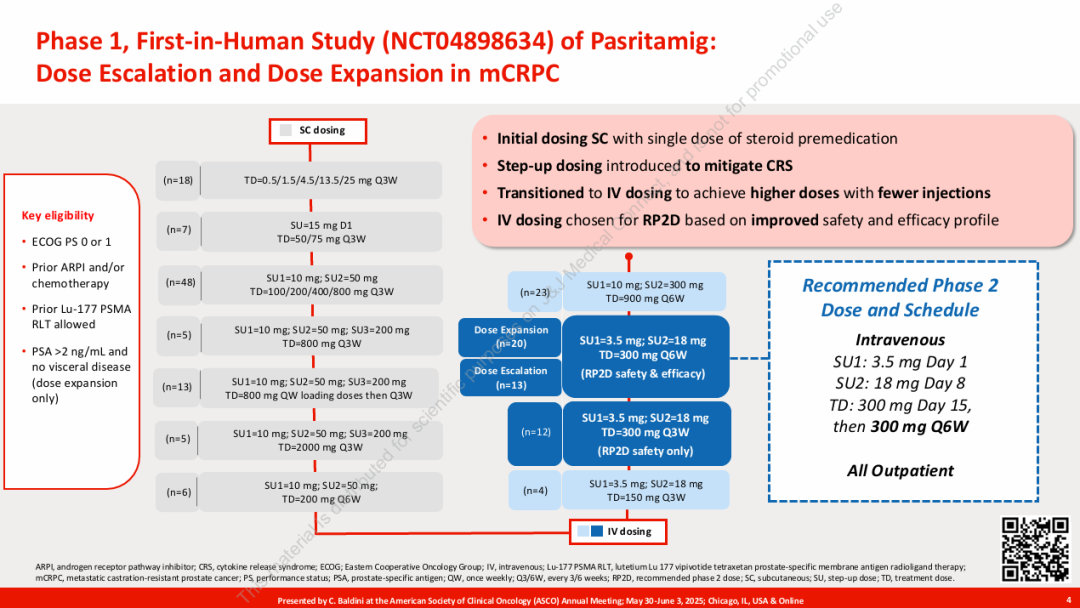
At the 2025 ASCO Annual Meeting, Johnson & Johnson presented the Phase I study results of Pasritamig (JNJ-78278343). As the first T-cell engager targeting human kallikrein 2 (KLK2), Pasritamig demonstrated excellent safety and efficacy in patients with metastatic castration-resistant prostate cancer (mCRPC).
Phase I First-in-Human Trial Evaluates 174 Patients Aged 36 to 89 Years, with an Average of 4 Prior Therapies. The Phase II Recommended Dose (RP2D) of Pasritamig is 3.5 mg on Day 1, 18 mg on Day 8, and 300 mg Intravenous Injection on Day 15, followed by once every six weeks. Due to a very similar toxicity profile, the RP2D safety group also included patients treated once every three weeks. The RP2D efficacy group only included patients receiving RP2D treatment once every six weeks.
In terms of efficacy, in the recommended Phase II dose (RP2D) group,42.4% of patients achieved a PSA50 response (prostate-specific antigen decrease ≥50%), with 36.4% being confirmed responses.; Median ImagingThe radiographic progression-free survival (rPFS) was 7.9 months, which is competitive compared to existing treatment data.As of the data cutoff, 21.2% of patients were still receiving treatment, suggesting the potential for long-lasting efficacy of the drug.
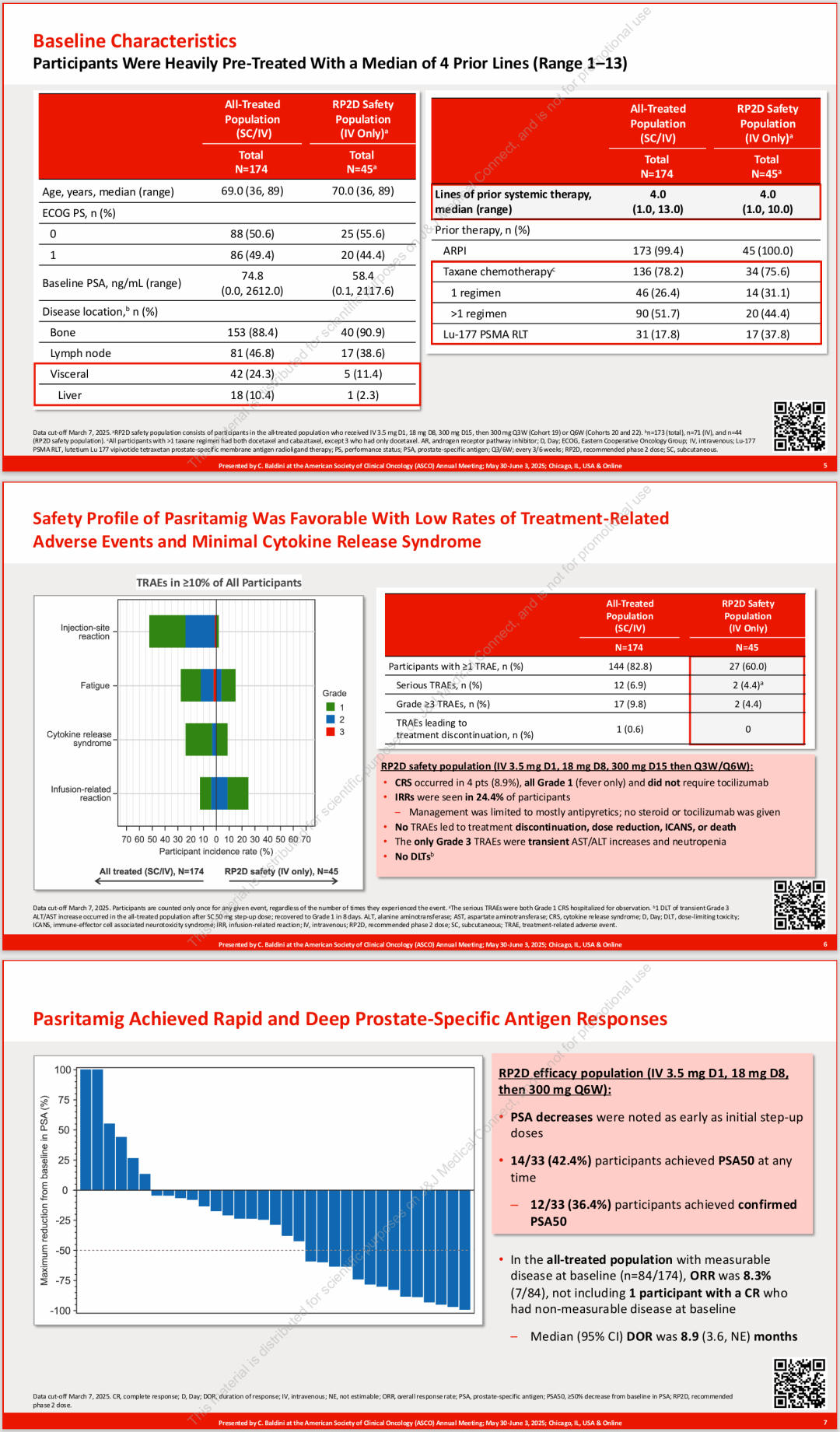
In terms of safety,Pasritamig has a lower incidence of adverse events, with no high-grade cytokine release syndrome (CRS) observed—only grade 1 CRS occurred, which did not require tocilizumab intervention. Overall, it demonstrated good tolerability.The study enrolled patients, most of whom had previously received ARPI and taxane chemotherapy. Of these, 99.4% had received an androgen receptor pathway inhibitor, and 78.2% had been treated with taxanes, indicating that Pasritamig remains active in refractory populations.
This study focused on the population of patients with metastatic castration-resistant prostate cancer (mCRPC) after multiple lines of treatment, among whom 99.4% had received androgen receptor pathway inhibitor (ARPI) therapy and 78.2% had undergone taxane-based chemotherapy. Regardless of whether the patients had previously received PSMA-targeted radioligand therapy (RLT), PSA50 responses and durable disease control were observed.
The recommended Phase II dose (RP2D) of Pasritamig is set to be administered once every six weeks in an outpatient setting, significantly enhancing the convenience of patient treatment.We look forward to the performance of this drug in future Phase III clinical trials, which provides new hope for patients with advanced prostate cancer.





Previous Review