Application Experience of Scoring Drug-Coated Balloon in AVG Stenosis: A Case Series by Professor Zhang Heping's Team

DK Medtech
Vascular Interventional Balloon Product Developer

AVGHyperplasia of the venous anastomosis is the main cause of AVG stenosis. Currently, multiple guidelines recommend PTA as the preferred method for treating AVG stenosis. Dense fibrosis in the stenotic venous segment or scar hyperplasia at the puncture site makes it difficult to fully dilate some lesions with ordinary-pressure balloons, especially for refractory and longer-segment stenoses, which are the primary causes of surgical failure and low patency rates. The reasons may be related to the irregular violent tearing of the intima and some newly formed medial tissue by the balloon during the PTA process, causing damage to the endothelial vessels and intense proliferation of vascular smooth muscle cells and macrophages. In recent years, there have been continuous international explorations and clinical studies on the use of high-pressure balloons, scoring balloons, and drug-coated balloons for PTA treatment of dialysis access. DK Medtech specializes in the research, development, and production of vascular interventional medical products, focusing on balloon innovation. It has developed the Dissolve™ AV Scoring Drug Balloon, which integrates "high pressure," "scoring," and "drug coating" to address multiple hotspots and challenges in hemodialysis access stenosis.
DK MedtechSpecial Launch[Application Experience of Scored Drug-Coated Balloons by Professor Zhang Heping's Team from the Affiliated Hospital of North Sichuan Medical College] Case Presentation, demonstrating the precise operations of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for hemodialysis access stenosis, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for the future diagnosis and treatment of hemodialysis access, benefiting more clinical patients.

Experience with the Application of Notched Drug-Coated Balloons
Zhang Heping, Affiliated Hospital of North Sichuan Medical College

Patient Information
Basic Information:Female, 43 years old.
Chief Complaint:Hemodialysis for 3+ years, poor fistula flow for 1 day.
History of Present Illness:More than 3 years ago, the patient was diagnosed with "chronic kidney disease stage 5" at another hospital. After undergoing an arteriovenous fistula formation procedure, regular dialysis treatment was initiated, 3 times per week, without difficulty in puncture, increased venous pressure, or hemostasis issues. One year ago, the patient began experiencing recurrent episodes of hypotension during dialysis, with the lowest readings being undetectable. Nine and four months prior, the patient experienced poor fistula flow on two occasions, both treated with balloon dilation at our hospital. One day ago, the patient again presented with poor fistula flow unable to sustain dialysis and visited our hospital on January 17, 2024.
Past Medical History:No special.
Physical Examination:No swelling or aneurysm-like dilation on the side of the limb with the internal fistula, but local puncture scars are visible. A weak thrill can be palpated at the anastomosis site of the internal fistula, and a murmur can be heard without enhanced pulsation.
Admission Diagnosis:
Stenosis of Arteriovenous Fistula;
Chronic Kidney Disease Stage 5;
Hemodialysis status.
Previous interventional treatment
Time | Main Treatment Process |
April 2020 | Arteriovenous Fistula Formation |
March 2023 | Stenosis of Internal Fistula, Ultrasound-guided PTA Treatment (5mm High-pressure Balloon) |
August 2023 | Stenosis of Internal Fistula, Ultrasound-Guided PTA Treatment (6mm High-Pressure Balloon) |
January 2024 | Poor Internal Fistula Flow |
Preoperative Assessment Examination
The diameter of the proximal radial artery is approximately 4.2mm, while the distal radial artery is occluded. Intimal hyperplasia occurs near the arterial anastomosis, leading to luminal stenosis of about 1.8mm, known as the S1 stenosis. Intimal hyperplastic stenosis S2 occurs in the cephalic vein near the anastomosis, with a minimum inner diameter of 1.5mm and an adjacent inner diameter of approximately 3.5mm, spanning a range of about 3cm.
Approximately 4 cm from the anastomosis, there is intimal hyperplastic stenosis S3, with a minimum inner diameter of about 1.7 mm, adjacent diameter of approximately 3.8 mm, and a range of about 2 cm.
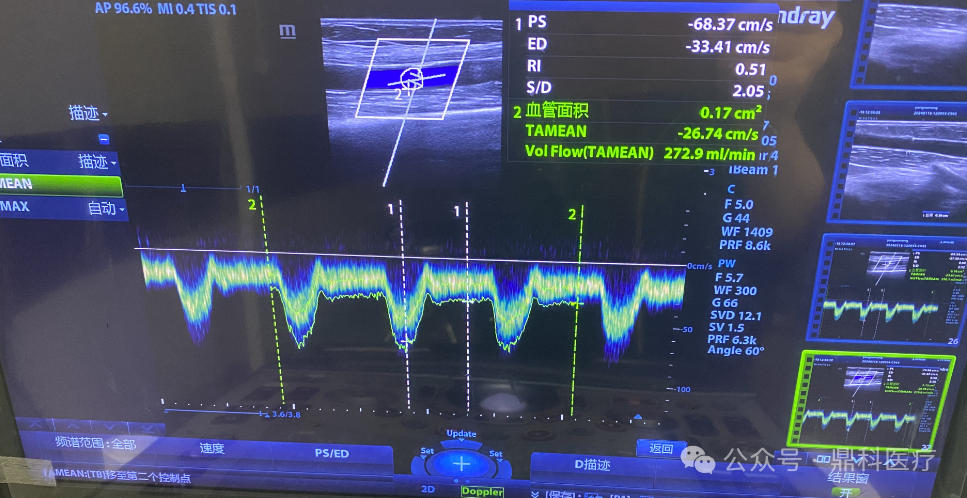
Preoperative brachial artery blood flow was 272.9 ml/min.
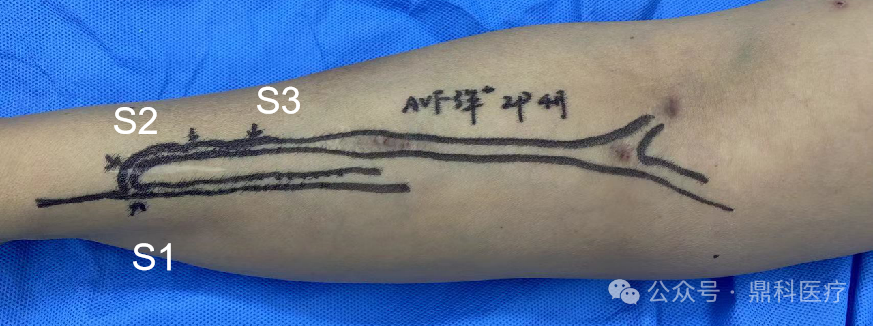
Preoperative Appearance Diagram.
Preoperative Analysis
Preoperative Analysis:Hyperplastic stenosis of arteriovenous fistula (Type I), planned to perform ultrasound-guided percutaneous transluminal angioplasty (PTA) of the right upper limb arteriovenous fistula.
Surgical Objective:
Main Objectives:Utilize high-pressure scoring to relieve S1, S2, and S3 stenosis.
Secondary Objective:Inhibit endometrial hyperplasia through drug action.
Surgical Strategy/Plan:
Plan to use a 5mm high-pressure balloon to dilate and relieve S1, and pre-dilate S2 and S3.
Significant intimal hyperplasia was observed in the arterial area near the anastomosis and in the fistula vein. It is planned to use a scoring drug-coated balloon (Dissolve™ AV) (6mmx60mm) for low-pressure drug application to S1 and S2, with full expansion of S2 and S3.
Surgical Procedure
Through the fistula vein retrograde approach, the guidewire tip enters the proximal end of the brachial artery. After pre-dilation of S3 with a 5mm high-pressure balloon at 20atm, advance to the anastomosis for full dilation of S1 and S2 at 20atm, maintaining for 30s-1min, and perform dilation twice.
After dilation, S1 and S2 were relieved.


Placement of a scored drug-coated balloon (6mmx60mm).
Placement of a scored drug-coated balloon (6mmx60mm) to cover S1 and S2.
6atm dilation, apply medication to S1 and S2, maintain for 2 minutes.
Retract the balloon, continue to fully expand S2 and S3 at 16atm, and maintain for 2 minutes.
S1 and S2 ExpansionThe diameter after expansion is approximately 3.3-4.5mm, with no vascular rupture.
The diameter of S3 is approximately 4.5mm after dilation.
The anastomotic site shows abundant blood flow signals.
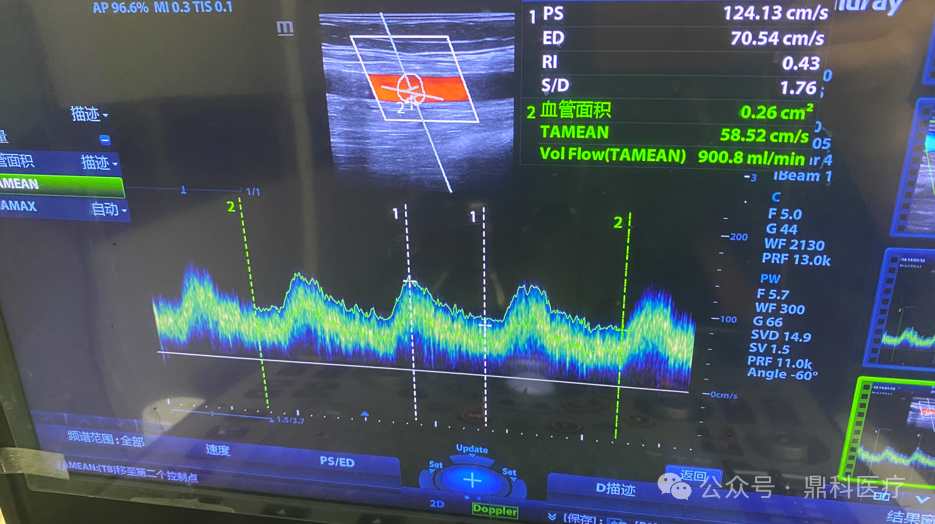
Postoperative brachial artery blood flow 900ml/min
Follow-up
Discharge Status:
Good postoperative thrill of the arteriovenous fistula, no enhanced pulsation. The next day, the patient's dialysis pump blood flow was 250ml/min.
Pre-discharge access care and follow-up education, with instructions to follow up at the dialysis access outpatient clinic two months post-surgery.
Case Summary
Case Characteristics:Long segmental, significant intimal hyperplastic stenosis.
Preoperative Assessment Key Points:
Evaluate the stenosis and the adjacent vessel diameter, and select the balloon size;
Preoperative evaluation and positioning requiredDissolve™ AV Balloon Drug Coating Position.
Surgical Strategy/Technical Key Points:
S1 anastomotic stenosis, arterial diameter approximately 4.2mm, 6mm balloon dilation may cause vascular rupture, planning to use 5mm high-pressure balloon to relieve S1.
Significant endometrial hyperplasia with irregular surface in S1 and S2, planned to be used after pre-dilation.Dissolve™ AV Balloon Coated with Drug and Navigated to S1 and S2, then Utilized its High-pressure Scoring Capability to Fully Dilate S3, Achieving Directional Tearing while Minimizing Intimal Injury.
Device Features/Usage Tips:
Preoperative balloon only needs to be flushed with saline in the balloon catheter lumen; soaking the balloon end is not recommended to avoid drug loss.
Do not remove the coating protective sleeve; advance the balloon along the guidewire to the sheath opening until it is locked at the sheath opening.
If the lesion has been fully dilated before the filling pressure is less than RBP, please maintain the pressure for 2 minutes to ensure adequate drug adhesion. If the lesion has not been fully dilated when the filling pressure reaches RBP, still maintain the pressure for 2 minutes, then release the pressure and rotate the balloon approximately 60° before re-dilating to RBP, and maintain the pressure for 1 minute.

Introduction of Experts


Zhang Heping, Associate Chief Physician
The Surgeon of This Case
Deputy Director of the Department of Nephrology and Secretary of the Party Branch at the Affiliated Hospital of North Sichuan Medical College;Member of the Nephrology Committee of the Chinese Research Hospital Association;Member of the Science Popularization Group of the Nephropathy Rehabilitation Professional Committee of the Chinese Rehabilitation Medical Association;Member of the Nephrology and Dialysis Professional Committee of the China Non-Public Medical Institutions Association;Member of the Nephropathy Prevention and Treatment Public Welfare Fund Professional Committee of the China Primary Health Care Foundation;Youth Committee Member of the Special Committee on the Development of Traditional Chinese Medicine for Kidney Diseases, China Association of Traditional Chinese Medicine;Vice Chairman of the Sichuan Provincial Association of Rehabilitation Medicine's Nephrology Committee;Standing Committee Member of the Sichuan Provincial Medical Health Promotion Association's Nephrology Committee;Member of the Metabolism Group of the Internal Medicine Professional Committee of the Sichuan Medical Association;Youth Committee Member of the Nephrology Specialized Committee, Sichuan Medical Association;Standing Committee Member of the Nephrology Special Committee of the High-Tech Zone Medical Association, Chengdu City;Member of the Nanchong City Medical Association's Nephrology Committee.

Department Introduction

The Department of Nephrology at the Affiliated Hospital of North Sichuan Medical College was established in 1985. It has now become the largest, most technically powerful, and most advanced kidney disease prevention and treatment center in Northeast Sichuan, integrating clinical care, teaching, and research. As one of the leading teams in Sichuan Province's nephrology field, it is a National Key Clinical Specialty (Provincial Project), a clinical teaching base for specialized nurses in hemodialysis under the Chinese Nursing Association, a training base for specialized nurses in hemodialysis in Sichuan Province, a network member unit of the National Clinical Research Center for Kidney Diseases, the lead unit of the Northeast Sichuan Nephrology Alliance, and the lead unit of the Northeast Sichuan Nephrology (Hemodialysis) Nursing Alliance.
Since the Department of Nephrology at the Affiliated Hospital of North Sichuan Medical College pioneered dialysis access technology in northeastern Sichuan in 2000, the department has continuously sent its members for further studies and research. With over 20 years of development and innovation, it has bravely taken on challenges and evolved into a specialized sub-group for dialysis access. Once again taking the lead in northeastern Sichuan, the hospital has established a day-care ward and an outpatient clinic for dialysis access, while comprehensively carrying out various dialysis access techniques. These include peritoneal dialysis catheter insertion and maintenance surgeries, as well as hemodialysis access surgeries such as autologous and artificial arteriovenous fistula formation, thrombolysis, open thrombectomy, reconstruction, reshaping, bridging, aneurysm resection, ultrasound-guided balloon angioplasty of arteriovenous fistulas, DSA-guided semi-permanent catheter insertion and replacement, and DSA-guided central venous balloon angioplasty. The surgical methods are diverse, and the surgical and postoperative management systems are standardized. Currently, the annual number of surgeries is close to 1,000 cases, ranking among the top in Sichuan Province, gradually establishing itself as the regional treatment center for dialysis access in northeastern Sichuan.
