Managing Complex Cephalic Arch Stenosis with Recurrent Thrombosis in Hemodialysis Access: A Case Report by Prof. Cao Hanhua’s Team Using Dissolve™ AV Scoring Drug-Coated Balloon

DK Medtech
Vascular Interventional Balloon Product Developer

Stenosis and obstruction of arteriovenous fistulas (AVFs) in hemodialysis patients severely affect the function and usability of vascular access. Dense fibrosis or hyperplastic tissue makes it difficult to fully dilate some lesions with ordinary-pressure balloons, especially for refractory and long-segment stenosis, which are the main causes of surgical failure and low patency rates. The reasons may be related to irregular tearing of the intima and partial neotissue of the media by balloon angioplasty (PTA), leading to endothelial damage and intense proliferation of vascular smooth muscle cells and macrophages. In recent years, there has been continuous international exploration and clinical research on the use of high-pressure balloons, scoring balloons, and drug-coated balloons for PTA treatment of dialysis access. DK Medtech specializes in the research, development, and production of interventional vascular medical products, focusing on balloon innovation. It has developed the Dissolve™ AV Scoring Drug-Coated Balloon, which integrates "high pressure," "scoring," and "drug coating" to address multiple key challenges associated with hemodialysis access stenosis.
DK MedtechSpecial Launch[Professor Cao Hanhua from Kecheng District People's Hospital: Management of Repeated Thrombosis in Complex Arteriovenous Fistula with Stenosis at the Venous Arch] Case Presentation, demonstrating the delicate operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for hemodialysis access stenosis, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future hemodialysis access diagnosis and treatment, benefiting more clinical patients.

Recurrent Thrombosis
Management of Stenosis in the Arched Cephalic Vein of Complex Arteriovenous Fistula
Cao Hanhua, Kecheng District People's Hospital

Basic Information NO.1
Patient:Female, 60 years old.
Chief Complaint:Hemodialysis for 12 years, increased venous pressure for 4 days.
History of Present Illness:More than 12 years ago, the patient was switched from peritoneal dialysis to hemodialysis due to a diagnosis of "polycystic kidney disease, chronic kidney disease stage 5, peritoneal dialysis-associated peritonitis." The vascular access was an autologous arteriovenous fistula in the left upper arm. The dialysis frequency was three times per week (Tuesday, Thursday, Saturday), lasting four hours each session, with generally smooth hemodialysis processes under normal circumstances. From June 2023 to August 2023, the patient was hospitalized multiple times at our facility for surgical treatment due to fistula thrombosis. The most recent surgery took place on August 21, 2023, which included upper limb venous catheter thrombolysis, catheter embolectomy, balloon dilation, and venography. The procedure went smoothly, and post-surgery, the fistula flow rate and venous pressure were adequate, with smooth hemodialysis processes. Four days ago, during hemodialysis, the patient’s venous pressure rose to a maximum of 280 mmHg, but blood flow remained acceptable. The patient reported that the fistula wall felt significantly stiffer upon palpation compared to before, with no swelling in the left forearm, no pain, no numbness or discomfort in the extremities, and no chills or fever. For further diagnosis and treatment, the patient visited our hospital, and the outpatient department admitted the patient with a diagnosis of "chronic kidney disease stage 5, arteriovenous fistula stenosis."
Past Medical History:The patient was diagnosed with "polycystic kidney disease and polycystic liver disease" over 14 years ago, at which time the serum creatinine level was 260 umol/L. Due to progressively increasing serum creatinine levels, the patient subsequently underwent dialysis treatment; Renal hypertension was also identified over 14 years ago, and in the past two months, the patient has been on midodrine tablets for low blood pressure management. The patient denies any history of trauma, blood transfusion, or allergies to medications or food.
Physical Examination:Physical Examination: A longitudinal surgical scar approximately 2.5 cm in length is visible 2 cm above the transverse elbow crease of the right upper limb. The cephalic vein shows significant tortuosity with evident saccular dilation, and there is no skin lesion. Palpation: The skin temperature of both upper limbs is normal. A distinct pulse can be palpated at the anastomosis site of the arteriovenous fistula and 2 cm above it, with a faint thrill. Auscultation: A unidirectional blowing murmur can be heard at the anastomosis site of the arteriovenous fistula.
Admission Diagnosis:Preoperative Diagnosis:
Stenosis of Arteriovenous Fistula;
Polycystic Kidney Disease, Chronic Kidney Disease Stage 5, Renal Anemia, Renal Hypertension, Hemodialysis Status;
Polycystic liver.
History of Vascular Access NO.2
Time | Main Treatment Process |
2023-06-15 | Recanalization of Left Upper Arm Cephalic Vein Arch Stenosis Occlusion + Catheter-directed Thrombolysis of Upper Limb Veins + 5mm High-pressure Balloon Dilation + Reconstruction of Cephalic Vein Arch |
2023-06-16 | Upper Limb Venous Catheter Thrombolysis + Surgical Thrombectomy + Cephalic Vein Arch Reconstruction + 6mm High-Pressure Balloon Dilation |
2023-08-21 | Upper Limb Venography + Superior Vena Cava Venography + Upper Limb Venous Catheter Thrombolysis + Catheter Embolectomy + 5mm High-Pressure Balloon Dilation |
Preoperative Analysis NO.3
Preoperative Analysis:The patient has a lesion in the cephalic vein arch and has undergone two previous reconstructions of the cephalic vein arch with PTA treatment. The last surgery only lasted for two months, and further expansion requires a change in treatment method to improve therapeutic outcomes. This time, the use of a scoring drug-coated balloon is being considered.
Surgical Objective
Main Objectives:Increase vascular diameter through PTA treatment with a scored drug-coated balloon;
Secondary Objectives:Inhibit intimal hyperplasia and improve fistula patency rate.
Surgical Strategy/Plan:Upper extremity venography, central venography + balloon angioplasty for left cephalic vein and left subclavian vein stenosis under DSA (Dissolve™ AV).

Surgical Procedure NO.4
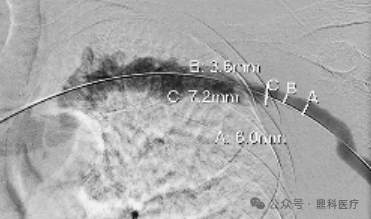
After puncturing the basilic vein in the upper arm, a 7F vascular sheath was inserted. The guidewire passed through the tortuous segment of the basilic vein, and was then advanced into the superior vena cava via the basilic vein. A 5mm high-pressure balloon was used for dilation at 18 ATM, maintained for 2 minutes. Post-procedure angiography showed rebound of the stenotic lesion.

Post-procedure angiography showed improvement in the stenotic lesion, no contrast extravasation, and a minimum lumen diameter of 3.6 mm at the most narrowed site.
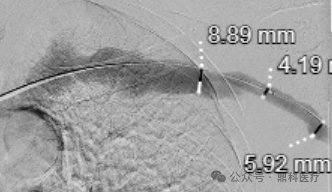
A 7mm high-pressure balloon was inserted through a guidewire exchange and repeatedly dilated at the stenotic lesion site where the left jugular vein meets the subclavian vein. The balloon was difficult to fully expand, so it was repeatedly dilated twice at 16ATM, with each dilation maintained for 2 minutes.
Post-procedure angiography showed improvement in the stenotic lesion, no contrast extravasation, and a minimum lumen diameter of 4.19 mm at the most severe stenosis site.
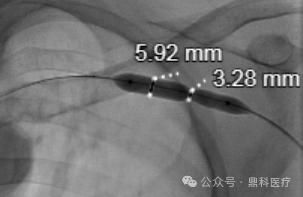
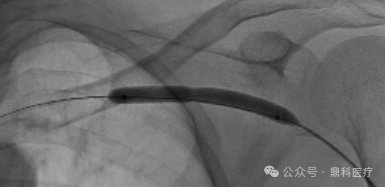
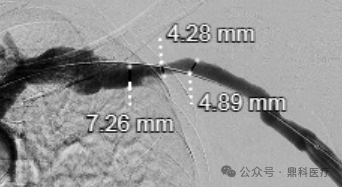
Heparin saline pre-flush preparation ready 6mm×6cm scored drug-coated balloon (DK Medtech Dissolve™ AV) exchanged over guidewire and positioned scored drug-coated balloon (DK Medtech Dissolve™ AV), expanded at 22-26ATM, maintained for 2 minutes 30 seconds.

Post-procedure angiography showed significant resolution of the stenotic lesion, with a diameter of 4.28mm at the narrowest point.
Follow-up NO.5
Discharge Status:Good postoperative fistula thrill, no abnormal pulsation detected. Postoperative dialysis proceeded smoothly with a dialysis flow rate of 260ml/min and venous pressure of 98mmHg. No pain was reported at the fistula site during dialysis.
Case Summary NO.6
Case Characteristics:The patient experienced repeated thrombosis of the internal fistula and had undergone PTA treatment twice before, with the last dilation lasting less than 2 months.
Preoperative Assessment Key Points:Preoperative comprehensive assessment of the intimal hyperplasia and vascular calcification degree of the patient's fistula vessels to formulate a reasonable surgical plan.
Surgical Strategy/Technical Key Points:To fully dilate the hyperplastic intima, inhibit postoperative intimal hyperplasia, and address calcified stenotic lesions, the Dissolve™ AV scoring drug-coated balloon is the optimal choice, offering the advantages of high pressure, scoring, and drug coating.
Device Features/Usage Tips:
Preoperative balloon only needs to be flushed with saline in the balloon catheter lumen; soaking the balloon end is not recommended to avoid drug loss.
Do not remove the coating protective sleeve; advance the balloon along the guidewire to the sheath opening until it is locked at the sheath opening.
If the lesion has been fully dilated before the filling pressure is less than RBP, please maintain the pressure for 2 minutes to ensure adequate drug adherence. If the lesion has not been fully dilated when the filling pressure reaches RBP, still maintain the pressure for 2 minutes, then release the pressure and rotate the balloon approximately 60° before re-dilating to RBP, and maintain the pressure for 1 minute. If there is significant residual stenosis or elastic recoil in the lesion, post-dilation can be performed using an ultra-high-pressure balloon or a high-pressure balloon with a diameter 1mm larger than Dissolve AV.
Surgical Record NO.7
1. 2023-06-15 Recanalization of Left Upper Arm Cephalic Vein Arch Stenosis Occlusion + Catheter-directed Thrombolysis of Upper Limb Veins + 5mm High-pressure Balloon Dilation + Cephalic Vein Arch Reconstruction
The patient lies in a supine position. Preoperative color Doppler ultrasound showed that the entire length of the arteriovenous fistula from the anastomosis to the cephalic vein arch in the upper arm was tortuous, dilated, and thrombosed. After routine disinfection and draping, a 6F vascular sheath was inserted towards the anastomosis at the site of fistula dilation in the middle of the upper arm. Under vascular ultrasound guidance, a 0.35 super-smooth guidewire was advanced to the brachial artery. A Boston Scientific MUSTANG 5*40mm dilation balloon (Boston Scientific) was then inserted over the guidewire. After removing the guidewire, 100,000 units of urokinase were injected into the balloon. A 6F vascular sheath was placed 5 cm proximal to the anastomosis and directed towards the heart. Under vascular ultrasound guidance, a 0.35 super-smooth guidewire was advanced but could not pass through the tortuous segment in the upper-middle part of the upper arm. A Boston Scientific MUSTANG 5*40mm dilation balloon (Boston Scientific) was inserted over the guidewire. After removing the guidewire, 100,000 units of urokinase were injected into the balloon, followed by balloon compression, which dissolved most of the thrombus and restored blood flow. The 6F vascular sheath in the middle of the upper arm was removed, and the puncture site was sutured with 5.0 vascular sutures. Subsequently, a 6F vascular sheath was reinserted towards the heart at the tortuous segment of the upper arm. Under vascular ultrasound guidance, a 0.35 super-smooth guidewire was advanced but could not pass through the cephalic vein arch. A Boston Scientific MUSTANG 5*40mm dilation balloon (Boston Scientific) was inserted over the guidewire. After removing the guidewire, 100,000 units of urokinase were injected into the balloon, followed by balloon compression, which dissolved most of the thrombus and restored blood flow. However, the occluded segment of the cephalic vein arch still could not be passed through. Attempts were made again with the balloon combined with the guidewire to pass through the stenotic segment of the cephalic vein arch. A 0.14 guidewire was used but still could not pass through. During the attempt with the 0.35 guidewire, the guidewire became embedded and fractured, leaving a residual fragment at the cephalic vein arch, where a thrombus formed again in the cephalic vein arch. After informing the patient's family, open surgery was performed.
The patient underwent brachial plexus anesthesia, followed by re-disinfection and draping. A 3 cm surgical incision was made in the middle of the upper arm, and the cephalic vein was dissected for about 2 cm with a rubber strip used to control blood flow. A 7 cm incision was then made 1 cm below the mid-clavicle. Blunt dissection exposed the cephalic vein arch, which appeared tortuous and dilated. The segment where it joined the subclavian vein showed a narrowing of about 3 cm. The narrowed section was transected, and a complete 5 cm segment of 0.35 guidewire tip was removed. Upon releasing the blood flow, a thrombus measuring approximately 10 x 0.8 cm was expelled. Color Doppler ultrasound confirmed no residual thrombus within the arteriovenous fistula. A Boston Scientific 5*40mm dilation balloon (MUSTANG) was used to dilate the cephalic vein arch near the subclavian vein. After dilation, a 2 cm oblique incision was made to trim the stenotic area and valve. The tortuous cephalic vein was repaired using 7.0 vascular sutures as a patch. After restoring blood flow, the inner diameter measured approximately 0.4 cm. Color Doppler ultrasound showed smooth blood flow. After thorough hemostasis, the vascular sheath was removed, and the incisions were sutured layer by layer. The procedure was completed.
2. Upper limb venous catheter thrombolysis + surgical thrombectomy + cephalic vein arch reconstruction + 6mm high-pressure balloon dilation on 2023-06-16
The patient lies flat, exposing the left upper limb. Preoperative color Doppler ultrasound showed thrombosis throughout the fistula anastomosis to the cephalic vein arch. After routine disinfection and draping, the original mid-upper arm skin incision was separated to expose the cephalic vein. A 0.5cm longitudinal venotomy was performed, and a vascular clamp was used to remove the thrombus. Blood flow was restored, ejecting multiple small thrombi. The vessel was sutured with 7-0 vascular sutures. Simultaneously, the original mid-clavicle skin incision was separated to expose the cephalic vein arch. The vessel was transected at the original suture site, and a long segment of thrombus was removed with a vascular clamp. Heparin saline was used for flushing. Proximal vessel patency was confirmed. The tortuous part of the cephalic vein was trimmed and anastomosed with 7-0 vascular sutures. After restoring blood flow, re-thrombosis of the distal fistula was observed, along with stenosis visible in the cephalic vein near the shoulder. The original vascular suture in the mid-upper arm was reopened, and the thrombus was again removed with a vascular clamp. A 6F vascular sheath was inserted into the mid-upper arm, and 100,000 units of urokinase were injected before inserting a 0.35 super-slip guidewire. A Boston Scientific MUSTANG 6*40mm dilation balloon (Bard) was advanced along the guidewire to compress the thrombus while adjusting the direction of the vascular sheath. A guidewire was advanced proximally, and a Boston Scientific MUSTANG 6*40mm dilation balloon (Bard) was advanced along the guidewire to the stenotic area of the cephalic vein near the shoulder. Three dilations were performed at 16-20 ATM, expanding the stenotic area from 2mm to 4mm. The balloon was then removed, and blood flow signals increased. Bleeding recurred at the cephalic vein near the mid-clavicle, likely due to vessel wall thinning associated with vascular sclerosis. The area was again sutured with 7-0 vascular sutures. Color Doppler ultrasound confirmed continuous fistula blood flow without significant thrombus, and thrill was palpable. The vascular sheath was removed, and the subcutaneous tissue and skin of the mid-upper arm and mid-clavicle were sutured in layers. Sterile dressing was applied.
3. Upper extremity venography + SVC venography + catheter-directed thrombolysis of upper extremity vein + catheter aspiration thrombectomy + 5mm high-pressure balloon dilation on 2023-08-21
The patient was placed in a supine position. After routine disinfection and draping, the puncture site was selected near the shoulder on the cephalic vein of the left upper arm. Successful puncture was achieved toward the distal end. Heparin was administered intravenously for prophylactic anticoagulation, and an 8Fr vascular sheath was inserted. Under ultrasound guidance, the guidewire was adjusted, and with the assistance of a balloon catheter, it successfully passed through the thrombus in the cephalic vein of the upper arm and through the anastomosis. The guidewire was then withdrawn, and urokinase was injected locally into the thrombus via the balloon for thrombolysis. After local massage and partial dissolution and softening of the thrombus, the guidewire was exchanged to insert and connect the thrombectomy catheter (AcoStream by Aortec) system. Under ultrasound guidance, repeated aspiration of the thrombus began within the thrombus, removing most of the thrombus distal to the puncture site. Increased pressure in the proximal lumen led to the insertion of an 8Fr vascular sheath directed toward the proximal end in the lower segment of the upper arm. Attempts were made to pass the guidewire through the tortuous lumen in the middle segment of the upper arm to reach the proximal thrombus site but failed repeatedly. Subsequently, the proximal sheath was rotated towards the proximal end, and a guidewire was inserted through the sheath. With the assistance of the guidewire, the thrombectomy catheter was inserted at the occluded cephalic vein arch, aspirating the thrombus from the proximal to the distal end. A guidewire and a 5*60mm balloon were then inserted through the sheath and successfully passed through the occluded lesion of the cephalic vein arch into the left subclavian vein. Gradual dilation was performed at 8-22 ATM, restoring patency of the local occlusion and the confluence of the subclavian vein. Post-dilation, the lumen was recanalized, and blood flow partially restored. Follow-up ultrasound indicated residual thrombus near the anastomosis in the middle and lower segments of the upper arm. An 8Fr vascular sheath was reinserted into the middle segment of the cephalic vein toward the distal end, and the thrombectomy system was inserted through the sheath for aspiration. Most of the thrombus was removed, and embolization occurred, drifting to the cephalic vein arch. Thrombectomy was again performed through the proximal sheath using the thrombectomy system, combined with biopsy forceps for mechanical thrombectomy. Afterward, the 5*60mm balloon was used to dilate the cephalic vein arch, with the longest inflation maintained for one minute. Upon completion, the local lumen was recanalized, with ultrasound showing a minimum internal diameter of 3mm. Angiography through the sheath showed recanalization of the cephalic vein in the upper arm, the cephalic vein arch, the left subclavian vein, the left innominate vein, and the superior vena cava, with significant thrill noted in the cephalic vein of the upper arm. The balloon, guidewire, and vascular sheath were sequentially removed, and the puncture site was sutured with 5-0 PROLENE thread. Hemostasis was achieved, followed by dressing application, concluding the procedure.

Introduction of Experts


Professor Cao Hanhua
Surgeon of This Case
Vice President of Kecheng District People's Hospital, Director of Nephrology Department, Chief Physician.
Leading Discipline Leader of County-Level Hospitals in Zhejiang Province, Rising Star in Zhejiang Medical Field, 115 Talent in Quzhou City, Committee Member of Nephrology Branch of Zhejiang Medical Association, Committee Member of Nephrology Branch of Quzhou Medical Association, Youth Committee Member of Rheumatology Branch of Zhejiang Medical Association.
Expertise: Diagnosis and treatment of kidney diseases and rheumatic diseases. Has accumulated rich experience in the treatment of refractory nephropathy and maintenance of complex vascular access. Was the first to carry out the puncture method of peritoneal dialysis catheter insertion in Zhejiang Province. The techniques for establishing and maintaining complex fistulas are at an advanced level in Zhejiang.

Department Introduction


The Nephrology Department of Kecheng District People's Hospital is a leading medical discipline at the county level in Zhejiang Province.Key Clinical Specialty Construction Project of Zhejiang Province,Key Discipline of Quzhou City, Key Collaborative Department of the Kidney Disease Center at the First Affiliated Hospital of Zhejiang University (Zhejiang University), Application and Promotion Unit for Hemodialysis Access Establishment and Maintenance Technology under the National Health Industry Enterprise Management Association, Member Unit of the Yangtze River Delta Vascular Access Alliance. The department has established several provincial expert workstations. It includes 2 chief physicians, 4 deputy chief physicians, 4 attending physicians, and 3 resident physicians. Professor Weiqin Lin and Professor Jianyong Wu from the Kidney Disease Center of the First Affiliated Hospital of Zhejiang University, as well as Professor Hua Li from the Kidney Disease Center of Sir Run Run Shaw Hospital affiliated with Zhejiang University, regularly visit the hospital for consultations, surgeries, and professional guidance. Currently, the department has 45 open beds and 83 hemodialysis machine positions, serving over 200 patients on long-term maintenance dialysis. The number of vascular access surgeries and dialysis sessions conducted annually rank among the top in the Quzhou region. The department was the first in western Zhejiang to perform laparoscopic peritoneal dialysis catheter implantation, parathyroidectomy with transplantation, balloon angioplasty and stent placement for fistula stenosis, and interventional procedures for central venous stenosis.
Main diseases diagnosed and treated:Chronic nephritis, nephrotic syndrome, IgA nephropathy, diabetic nephropathy, hypertensive nephropathy, multiple myeloma-associated nephropathy, chronic renal failure, urinary tract infection, systemic lupus erythematosus, rheumatoid arthritis, Sjögren's syndrome, scleroderma, dermatomyositis, etc.
Main Surgeries Performed:Renal biopsy, temporary hemodialysis catheter insertion, semi-permanent hemodialysis catheter with polyester cuff insertion, autologous arteriovenous fistula formation, artificial vessel arteriovenous fistula formation, thrombectomy of autologous/artificial vessel arteriovenous fistula, balloon dilation and stent placement for autologous/artificial vessel arteriovenous fistula, instant-access artificial vessel arteriovenous fistula formation, interventional treatment for central venous lesions under DSA, peritoneal dialysis catheter insertion, parathyroidectomy with autotransplantation, etc. Annual surgical volume exceeds 600 cases, ranking among the top in nephrology specialties across Zhejiang Province.
Main Medical Technology:Diagnosis and treatment of early-stage kidney disease, immunosuppressive therapy for chronic kidney disease, hemodialysis, hemofiltration, diagnosis and treatment of complications related to end-stage kidney disease, peritoneal dialysis, etc.
