Dissolve™ AV Scoring Drug-Coated Balloon for Recurrent, High-Resistance AVF Stenosis: A Case Series from Sir Run Run Shaw Hospital Access Team

DK Medtech
Vascular Interventional Balloon Product Developer

Stenosis and occlusion of arteriovenous fistulas (AVFs) in hemodialysis patients severely affect the function and usability of vascular access. Dense fibrosis or hyperplastic tissue makes it difficult to fully dilate some lesions with standard-pressure balloons, especially for refractory and long-segment stenosis, which are the main causes of surgical failure and low patency rates. The reasons may be related to the irregular tearing of the intima and partial neotissue of the media by balloon angioplasty (PTA), leading to endothelial damage and intense proliferation of vascular smooth muscle cells and macrophages. In recent years, there has been growing exploration and clinical research worldwide on the use of high-pressure balloons, scoring balloons, and drug-coated balloons for PTA treatment of dialysis access. DK Medtech, specializing in the research, development, and production of vascular interventional medical devices, focuses on balloon innovation and has developed the Dissolve™ AV Scoring Drug-Coated Balloon, integrating "high pressure," "scoring," and "drug coating" to address multiple key challenges associated with hemodialysis access stenosis.
DK MedtechSpecial Launch【Access Team of Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University: Treatment of Recurrent AVF High-Resistance Stenosis with Scoring Drug-Coated Balloons】, demonstrating the precise operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, intraoperative standardized procedures and technical applications, complication prevention, perioperative management, and other aspects, the aim is to promote the standardization of diagnosis and treatment for hemodialysis access stenosis, strengthen technical exchange and experience sharing among doctors, with the hope of providing new ideas and methods for the future diagnosis and treatment of hemodialysis access, benefiting more clinical patients.

Breaking Through Hardships, Extending Effects: Combining Near and Far
Scoring Drug-Coated Balloon for the Treatment of Recurrent High-Resistance Stenosis in AVF
Lu Mingxi, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine

Basic Information NO.1
Patient:Male, 66 years old.
Chief Complaint:Maintenance hemodialysis for 3 years, difficulty in fistula hemostasis for 2 weeks.
History of Present Illness:Stenosis of arteriovenous fistula, chronic kidney disease stage 5, on hemodialysis, hypertension.
Past Medical History:More than four years ago, the patient was found to have a creatinine level of 850umol/L during a routine examination for diabetic complications. He was then admitted to the Endocrinology Department of another hospital for treatment (specific medications unknown). Later, as his creatinine level remained high, the local hospital recommended dialysis. The patient underwent peritoneal dialysis for over a year. At the end of 2020, he underwent an autologous arteriovenous fistula formation in the left upper arm (high elbow fistula). Over three years ago, he started regular hemodialysis (on Mondays, Wednesdays, and Fridays). Due to poor fistula flow, he underwent balloon angioplasty after arteriovenous fistula surgery in June 2021 and June 2022 respectively. Two weeks ago, it became difficult to stop bleeding at the hemodialysis puncture site of the aneurysm. An outpatient ultrasound review showed stenosis of the fistula, and PTA is planned. The patient has had type 2 diabetes for 19 years, with blood sugar controlled by Aspart insulin, which has been fairly effective; hypertension was diagnosed 6 years ago, currently treated with oral antihypertensive drugs, and blood pressure is under control.
Physical Examination:Increased pulsation and weakened thrill at the autologous arteriovenous anastomosis of the left upper arm. Obvious thrill can be palpated 10 cm from the anastomosis at the outflow tract of the basilic vein fistula, with the stenotic area transitioning from pulsation to thrill. Positive arm-raising test: after raising the arm, the blood vessels near the fistula anastomosis remain highly engorged and cannot collapse.
Admission Diagnosis:Preoperative Diagnosis: Stenosis of arteriovenous fistula, Chronic Kidney Disease Stage 5, Hemodialysis status, Hypertension.
History of Vascular Access NO.2
Time | Main Treatment Process |
2023.12.5 | Balloon Expansion After Arteriovenous Fistula Creation in the Left Upper Arm |
2023.6.27 | Balloon Expansion After Arteriovenous Fistula Creation in the Left Upper Arm |
2022.6 | Balloon Expansion After Arteriovenous Fistula Creation in the Left Upper Arm |
2020.12 | Left upper arm autologous arteriovenous fistula formation, access via brachial artery to median cubital vein fistula, with the basilic vein of the upper arm as the drainage vein. |
Early 2020 | Start hemodialysis, initially peritoneal dialysis |
Preoperative Analysis NO.3
Preoperative Analysis:The patient was hospitalized for balloon angioplasty of an arteriovenous fistula six months ago due to excessive pressure in the fistula and difficulty in hemostasis. Restenosis occurred six months after the surgery. The previous use of high-pressure balloon dilation had been ineffective for this patient. For this hospitalization, it is planned to treat the lesion using either a high-pressure balloon or a high-pressure scoring drug-coated balloon.
Surgical Objective
Short-term Goals:Solve the problem of patients' difficulty in hemostasis and restore their hemostasis time to normal.
Long-term Goals:Extend the primary patency time of patients' fistulas and reduce the number of interventions.
Surgical Strategy/Plan
Balloon dilation treatment using high-pressure balloons;
Evaluate the effect of high-pressure balloon dilation during the operation. If the effect is not as expected, use a high-pressure scoring balloon for treatment.

Preoperative evaluation, brachial artery-median cubital vein fistula, with the drainage vein being the basilic vein of the upper arm. The arrow indicates the site of stenosis.
Surgical Procedure NO.4
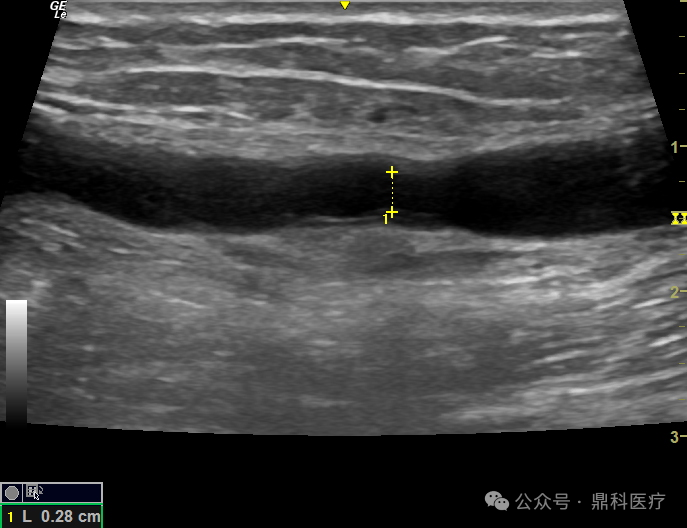
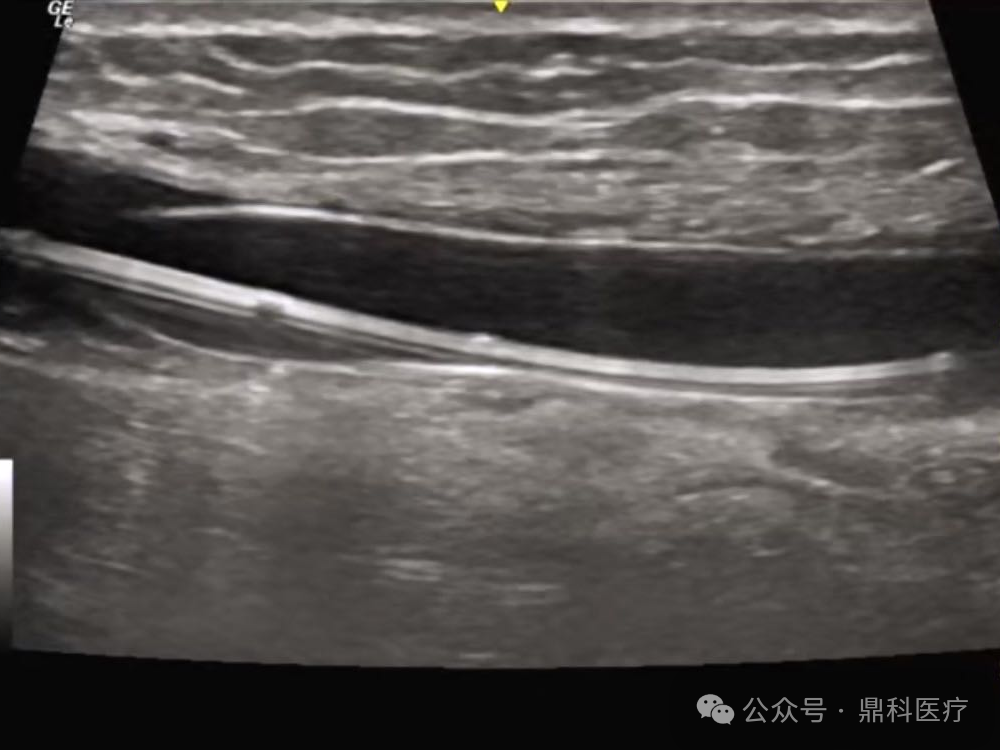
Imaging Description:Preoperative assessment: Color Doppler ultrasound showed a stenosis 10 cm from the anastomosis in the left upper limb, with the narrowest inner diameter approximately 1.9 mm and intimal thickness 2.2 mm.

Imaging Description:Preoperative assessment: Color Doppler ultrasound showed a stenosis 10 cm from the anastomosis in the left upper limb, with the narrowest inner diameter approximately 1.9 mm and intimal thickness 2.2 mm.
Imaging Description:The patient lies in the supine position, with the left forearm in external rotation. After routine disinfection and draping, 2% lidocaine is used for infiltration anesthesia on the venous outflow tract side of the left upper arm. The puncture needle is inserted, and upon observing the rush of arteriovenous fistula blood flow, the guidewire is advanced. The needle is withdrawn, the skin is punctured, and a 6F sheath is inserted. Heparin (20mg) is administered intravenously. The guidewire passes through the lesion.
Imaging Description:First, a 7.0mm * 40mm DK Medtech high-pressure balloon was used for dilation. After reaching the burst pressure, the balloon still had a notch, and the stenosis was not fully expanded.
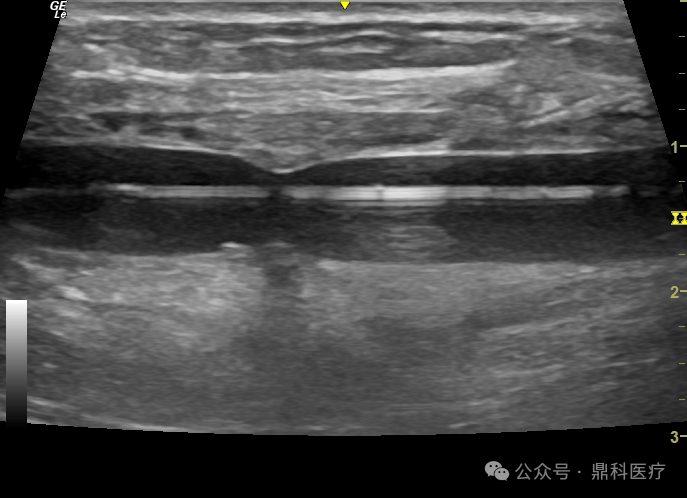
Imaging Description:Switched to a 7.0mm * 60mm DK Medtech high-pressure scored drug-coated balloon, which reached the lesion site.
Imaging Description:7.0mm*60mm DK Medtech high-pressure scored drug-coated balloon was slowly inflated to 20atm. Initial notch remained, and the pressure was continuously maintained until 120 seconds.
Imaging Description:7.0mm*60mm DK Medtech high-pressure scored drug-coated balloon continuously expands, with late-stage stenosis gradually improving until fully dilated, and pressure is released after 120 seconds.
Imaging Description:Evaluate after the first dilation.
Imaging Description:7.0mm*60mm DK Medtech High-Pressure Scoring Drug-Coated Balloon Rotates 60 Degrees and Reaches the Lesion Site Again.
Imaging Description:The 7.0mm*60mm high-pressure scored drug-coated balloon was dilated again at 20atm and maintained for 60 seconds.
Imaging Description:After the dilation was completed, the narrow inner diameter was re-measured at 5.5mm, and the brachial artery flow was measured at 1417ml/min.

The scored drug-coated balloon used during the surgery.
Follow-up NO.5
Discharge Status:The patient was discharged smoothly, with improved pressure during local dialysis and a hemostasis time of less than 10 minutes.
Case Summary NO.6
Preoperative Assessment Key Points:Preoperative ultrasound evaluation: the inflow diameter of the proximal artery is 8.1mm, anastomosis diameter is 3.8mm, normal outflow tract diameter is 8.0mm, and fistula flow is 612ml/min. Color Doppler ultrasound shows a stenosis in the left upper limb located 10cm from the anastomosis, with the narrowest inner diameter approximately 1.9mm and intima thickness 2.2mm.
Surgical Strategy/Technical Key Points:
In June 2023, this patient underwent balloon angioplasty for arteriovenous fistula stenosis. The use of a high-pressure balloon dilation yielded unsatisfactory results, with short-term recurrence of restenosis postoperatively.
The AV Peripheral Scoring Balloon Dilation Catheter, in addition to having high-pressure characteristics, features scoring elements on its surface that provide focused pressure scoring. This enables effective and precise incision of the intima and fibrous ring, enhancing dilation efficiency and increasing lumen gain. The balloon surface is coated with paclitaxel, which effectively inhibits intimal hyperplasia at the lesion site, improving long-term patency rates.
In this case, it can be seen that the lesion was fully opened when pressurized to 20 atm.
Characteristics/Usage Tips of the Device:
Dissolve AV Peripheral Scoring Balloon Dilation Catheter is equipped with three nickel-titanium alloy triangular scoring elements on its surface. The balloon surface is coated with a paclitaxel drug layer, which is used to inhibit the proliferation of the intima after adequate expansion of the lesion. In this case, after using the balloon once, rotate the balloon approximately 60 degrees and expand the lesion again to achieve more thorough dilation treatment for the stenotic lesion.
During the use of the AV Peripheral Scoring Balloon Dilation Catheter, pay attention to the following: When pressurizing up to 8 atm, increase by 2 atm every 3 seconds. Do not increase pressure too quickly to minimize the occurrence of complications such as vascular rupture and dissection.
For lesions that are resistant to initial dilation, maintaining the burst pressure for a period of time can fully leverage the role of the scoring wire, and there is still an opportunity to completely dilate the stenosis.

Introduction of Experts


Professor Li Hua
Surgical Guidance
Director of the Department of Nephrology, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University; Director of the Vascular Access Center; Member of the Zhejiang Province Nephrology Committee of the Chinese Medical Association; Member of the Nephrology Committee of the Chinese Research Hospital Association; Standing Committee Member of the Clinical Nephrology Professional Committee of the China Medical Education Association; Member of the Vascular Access Group under the Blood Purification Center Management Branch of the Chinese Hospital Association; Chairman of the Nephrology Committee of the Zhejiang Society of Mathematical Medicine; Deputy Director of the Zhejiang Dialysis Quality Control Center; Vice Chairman of the Zhejiang Kidney Rehabilitation Society.

Professor Lu Mingxi
Surgeon of This Case
Chief Physician, Attending Doctor, Assistant Director of the Nephrology Department at邵逸夫医院
Graduated from the Medical College of Zhejiang University, and went to Shizuoka Prefectural General Hospital in Japan for further study in 2014.
Committee Member of the Society Of Dialysis Access Specialists (SoDAS)
Member of the Vascular Access Working Group of the Blood Purification Branch of the China Hospital Management Association
Member of the Chinese Hemodialysis Access Expert Committee of the International Vascular Alliance
Member of the Geriatric Nephrology Branch of the Chinese Geriatrics Society
Member of the Nephrology Branch of the Zhejiang Medical Association, Deputy Leader of the Dialysis Access Group
Standing Committee Member of the Blood Purification Group, Artificial Organs Branch, Chinese Society of Biomedical Engineering
Youth Committee Member of the Vascular Access Specialty Committee of the Peripheral Vascular Disease Branch of the Chinese Society of Integrated Traditional and Western Medicine
Standing Committee Member of the Dialysis Access Group, Integrated Traditional Chinese and Western Medicine Intervention Committee, China Association of Traditional Chinese Medicine Information
Standing Committee Member of the Vascular Access Group, Interventional Physicians Branch, Chinese Medical Doctor Association
Member of the Asia-Pacific Vascular Academic Alliance Hemodialysis Access Youth League
Standing Committee Member and Secretary of the Nephrology Committee, Zhejiang Society of Mathematical Medicine
Standing Committee Member of the Health Appropriate Technology Branch of the China Health Industry Enterprise Association
