Case Series: Management of Recurrent AVG Outflow Stenosis by Professor Xu Yong’s Team

DK Medtech
Vascular Interventional Balloon Product Developer

Intimal Hyperplasia at the AVG Venous Anastomosis is the primary cause of AVG stenosis. In addition, intimal hyperplasia in the outflow tract is also one of the reasons for AVG stenosis and dysfunction. Currently, multiple guidelines recommend PTA as the first-line treatment for AVG stenosis. Dense fibrosis in the stenotic venous segment or scar tissue proliferation at the puncture site makes it difficult to fully dilate some lesions with a standard-pressure balloon, especially for refractory and long-segment stenosis, which are the main causes of surgical failure and low patency rates. The reason may be related to the irregular tearing of the intima and partial neotissue of the media by the balloon during PTA, causing damage to endothelial vessels and intense proliferation of vascular smooth muscle cells and macrophages. In recent years, there has been continuous international exploration and clinical research on the use of high-pressure balloons, scoring balloons, and drug-coated balloons for PTA treatment of dialysis access. DK Medtech specializes in the research and development and production of vascular interventional medical products, focusing on balloon innovation, and has developed the Dissolve™ AV Scoring Drug Balloon, which integrates "high pressure," "scoring," and "drug coating" to address multiple hotspots and challenges in hemodialysis access stenosis.
DK MedtechSpecial Launch[Changsha Jieao Hospital - Professor Xu Yong, Professor Liu Xinxin, Professor Ling Jie: Management of Recurrent Stenosis in AVG Outflow Tract] Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, perioperative management, etc., it aims to promote the standardization of diagnosis and treatment for hemodialysis access stenosis, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future hemodialysis access diagnosis and treatment, benefiting more clinical patients.

Repeated Stenosis Management of AVG Outflow Tract
Xiang Yi Jia Nephrology Doctors Group - Changsha Jie Ao Hospital: Xu Yong, Liu Xin Xin, Ling Jie

Basic Information NO.1
Patient:Male, 48 years old.
Chief Complaint:Regular hemodialysis for 18 years, high venous pressure during dialysis for half a month.
History of Present Illness:18 years ago, he was diagnosed with chronic kidney disease at the uremic stage due to fatigue and poor appetite in another hospital, and then started regular hemodialysis. During this period, he visited our hospital multiple times due to access issues. Half a month ago, he experienced high venous pressure during dialysis, reaching over 300mmHg at its highest, and required more than 2 hours of needle compression post-dialysis, prompting him to seek medical attention.
Past Medical History:Previous history includes "reduction, bone grafting, and internal fixation with a plate for a right intercondylar supracondylar femoral fracture due to trauma," a history of temporary neck tube placement surgery, a history of arteriovenous fistula formation surgery in both forearms, and a history of parathyroidectomy.
Physical Examination:Body Temperature: 36.3°C, Pulse: 98 beats/min, Respiration: 20 breaths/min, Blood Pressure: 128/88 mmHg. A palpable thrill and induration at the anastomosis of the arteriovenous fistula were noted, with faint vascular murmur audible.
Admission Diagnosis:Preoperative Diagnosis: 1. Stenosis of arteriovenous fistula 2. Chronic renal insufficiency, uremic stage, uremic cardiomyopathy, renal anemia, renal hypertension.
History of Vascular Access NO.2
Time | Main Treatment Process |
2005 | Initiate Arterial Direct Penetration Dialysis |
2008 | Left forearm AVF |
2010 | Left AVF failure, establish right forearm AVF |
2019 | Dysfunction of the forearm AVF, reconstructed at another hospital |
2020 | Right-sided outflow stenosis of the internal fistula, underwent patch surgery |
July 2021 | The right AVF was completely occluded from the anastomosis to the elbow, and PTA + thrombectomy surgery was performed in our hospital. |
November 2021 | The right AVF was completely occluded again, so the second PTA + thrombectomy surgery was performed. |
July 2022 | High Tension in Internal Fistula Leads to Difficult Hemostasis and Third PTA Surgery |
September 2022 | Repeat occlusion led to thrombectomy + artificial vessel grafting (outflow tract) |
November 2022 | Due to the high tension of the internal fistula, it was difficult to stop the bleeding, and the patient visited our hospital for the fifth time. |
January 2023 | The 6th Time: Restenosis of the Outflow Tract, Treated with Drug-Coated Balloon + Thrombectomy |
November 2023 | The 7th Time: Restenosis of the Outflow Tract, Treated with High-Pressure Scoring Drug-Coated Balloon + Thrombectomy |
Preoperative Analysis NO.3
Surgical Goal
Main Objectives:Clinical Manifestations of High Venous Pressure During Dialysis Resolution for More Effective Dialysis
Secondary Objective:Extend the Service Life of Dialysis Access, Reduce Intervention Frequency
Surgical Strategy/Plan
Balloon dilation (using high-pressure scored drug-coated balloon) + thrombectomy
Abandon the internal fistula and switch to artificial blood vessels.
Long-term Care
Surgical Procedure NO.4

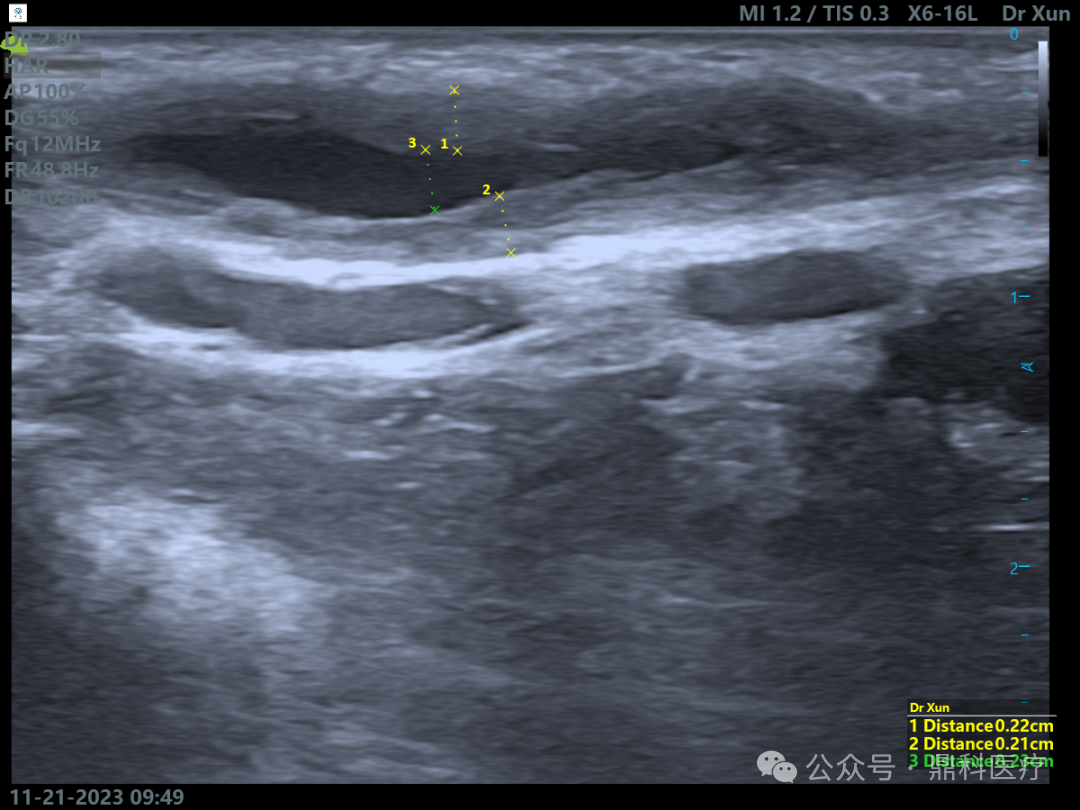
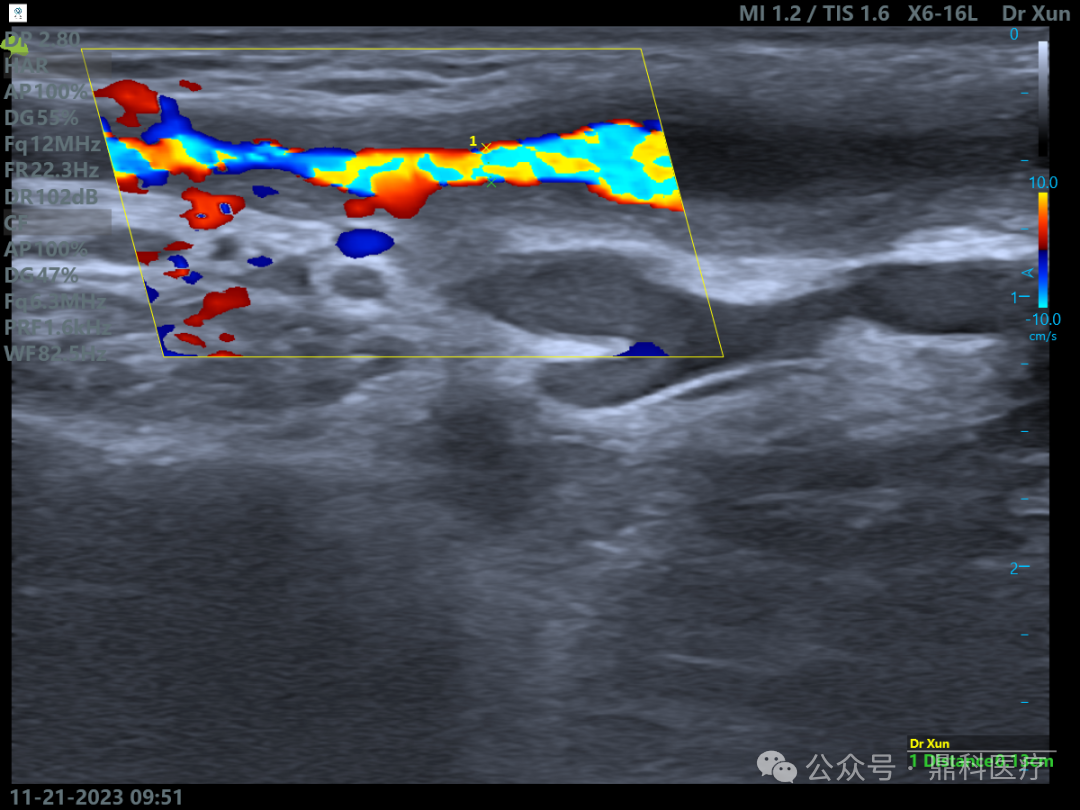
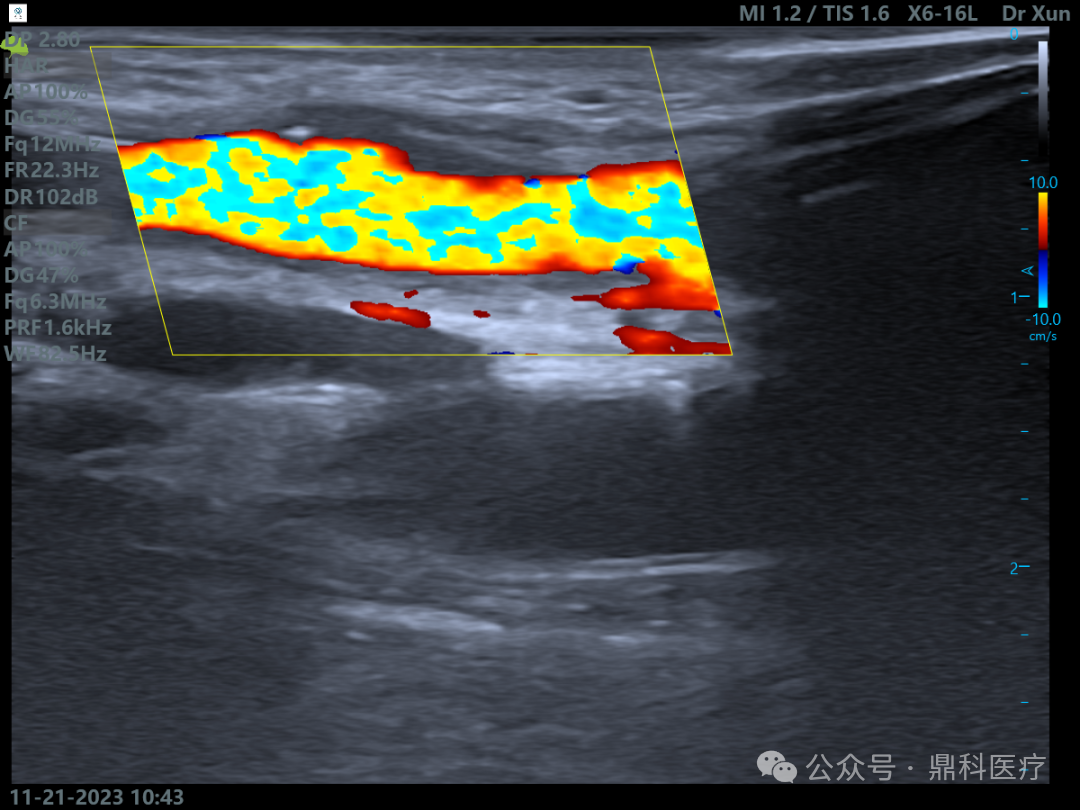
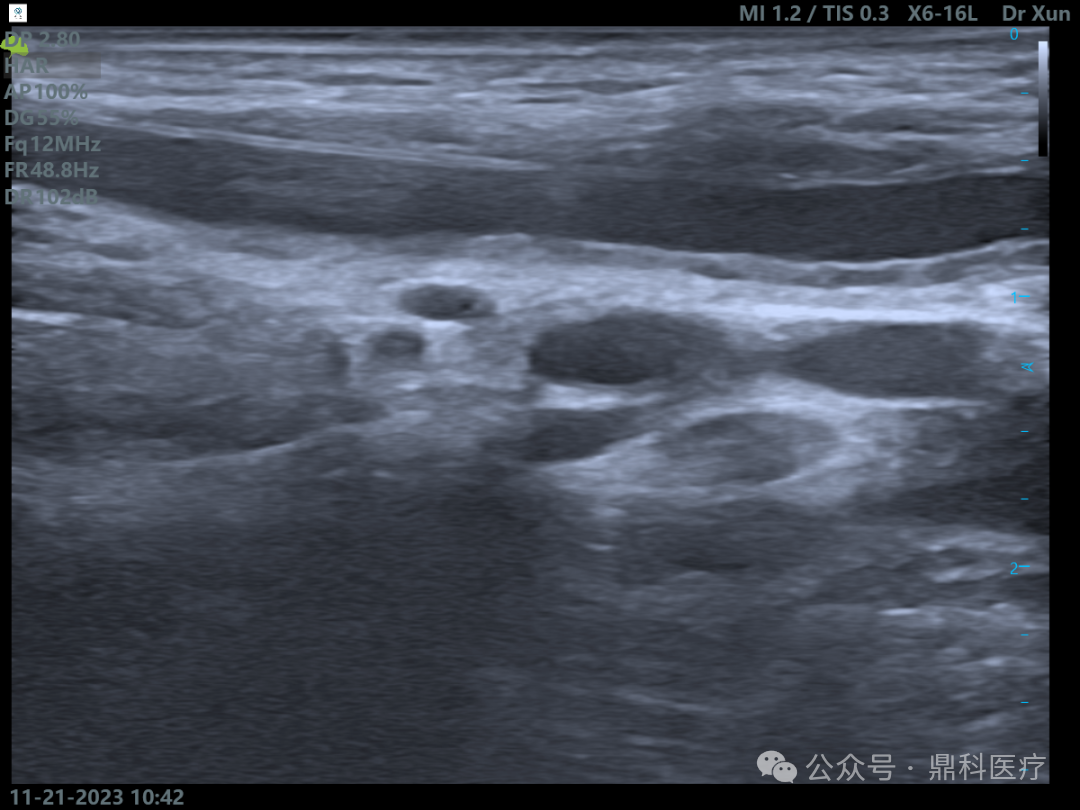
Preoperative assessment showed aneurysmal dilation and intimal thickening, with multiple PTA surgeries performed.

An 8F short sheath was placed into the aneurysm-like dilation, and a .35 guidewire was inserted, smoothly passing through the stenotic segment.
The balloon was placed into the stenotic segment and began to expand, maintained for 90 seconds, repeated two to three times.
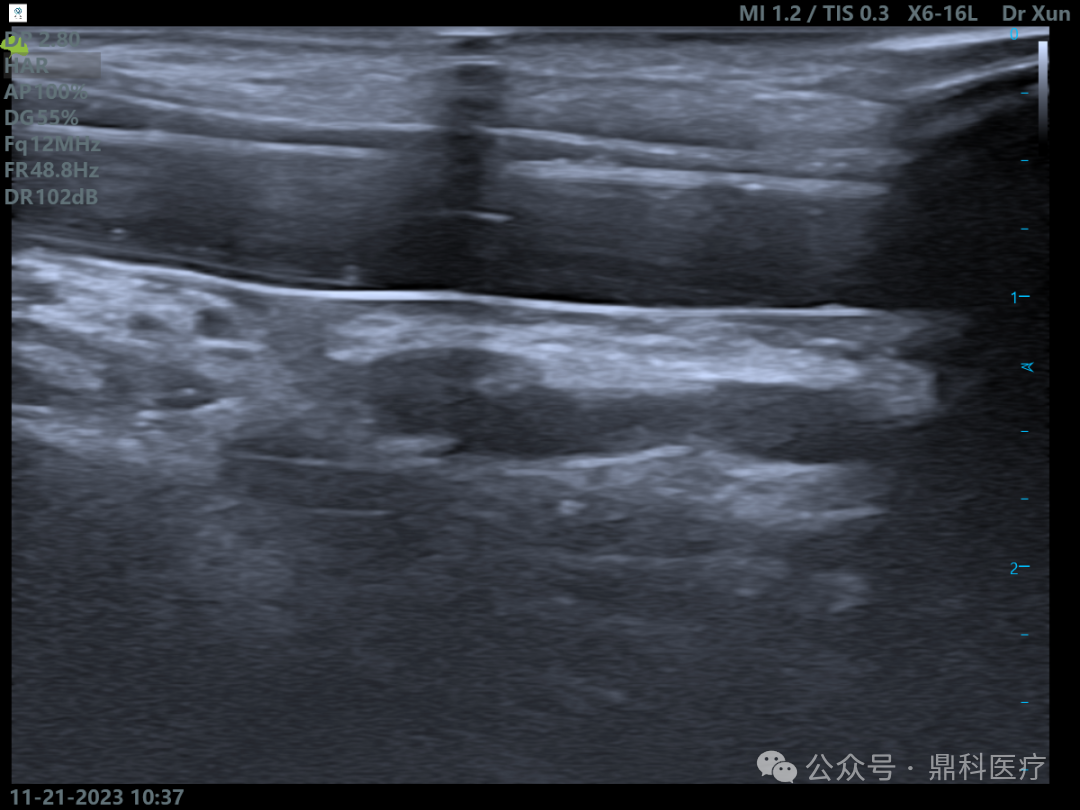
After dilation, the narrowed segment of the blood vessel is visible, with a significantly increased effective lumen.
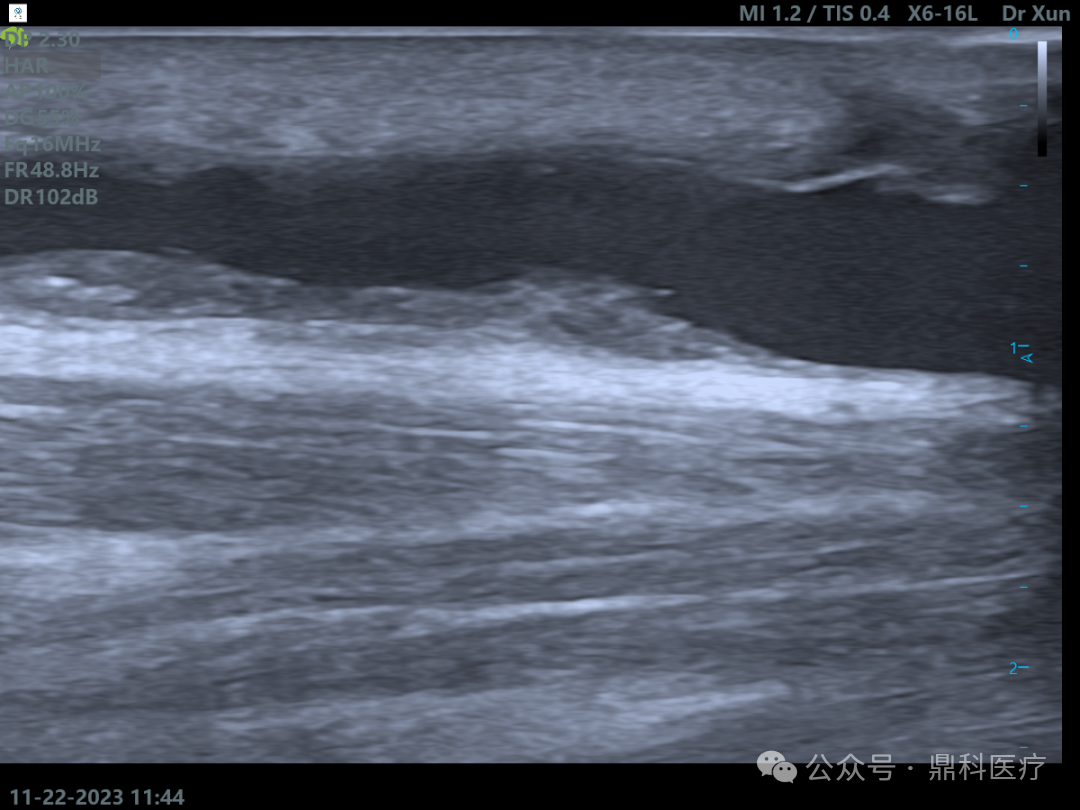
On the second day after the operation, the复查 showed that the vascular cavity's intima had significantly improved compared to immediately post-operation.
Follow-up NO.5
Discharge Status:The patient's condition is stable. Re-examination of the right upper limb arteriovenous fistula ultrasound shows: RI 0.5, blood flow 1122 ml/min (preoperative 275 ml/min). The venous pressure during dialysis is around 100 mmHg, and bleeding can be stopped with 20 minutes of compression after needle removal post-dialysis.
Case Summary NO.6
Case Characteristics:Long-term dialysis patient with multiple access surgeries.
Preoperative Assessment Key Points:Based on the patient's own vascular conditions, a suitable surgical plan is generally formulated.
Surgical Strategy/Technical Key Points:It is planned to insert the sheath from the arterial puncture site, pass through with a .35 guidewire towards the heart, and after reaching the lesion site, place the balloon for dilation.
Device Features / Usage Tips:Reduce the contact between the balloon body and the external environment (choose an 8F short sheath; do not remove the protective sleeve from the balloon body, advance the balloon along the guidewire to the sheath opening until it is snugly fitted), minimizing drug loss; before starting dilation, ensure the balloon is positioned at the lesion site; maintain balloon inflation for 90-120 seconds after expansion; after releasing pressure, rotate the balloon 60° and expand again; during expansion, minimize coverage of the normal vessel wall.

Introduction of Experts


Professor Xu Yong
Surgical Guidance
Attending Physician, Department of Nephrology, Third Xiangya Hospital, Central South University, Medical Doctor.
Research Direction: Surgical Treatment of Secondary Hyperparathyroidism in Uremic Patients and Establishment and Maintenance of Vascular Access.
Standing Committee Member of the Ultrasound Interventional Vascular Access Group, Interventional Physicians Branch, Chinese Medical Doctor Association;Member of the Vascular Access Group, Blood Purification Branch, Chinese Hospital Association;Member of the Hunan Traditional Chinese Medicine Association's Professional Committee on Nephrology;Director of the Kidney Health Branch of the Hunan Kidney Health Service Association.

Professor Liu Xinxin
Surgeon of This Case
Graduated from Nanhua University, currently serving as the Director of the Nephrology Department at Changsha Jieao Kidney Disease Hospital, and concurrently holding the position of Chief of the Medical Affairs Department at Changsha Jieao Hospital.
With over a decade of experience in nephrology and hemodialysis, participated in more than 2,000 cases of surgical treatment for hyperparathyroidism, ranking among the leading in China. Possesses extensive management experience for patients undergoing hyperparathyroidism surgery. Specializes in primary and secondary kidney diseases, diagnosis and treatment of chronic kidney disease, management of hemodialysis patients, temporary and long-term hemodialysis catheterization, arteriovenous fistula surgery, handling complex vascular access, artificial blood vessels, and vascular access interventional procedures. Familiar with common internal medicine conditions, treatment of critically ill patients, management of acute complications during hemodialysis, and systematic management of hemodialysis patients. Proficient in evaluating, long-term planning, and establishing vascular access.
Published multiple papers in core journals and domestic journals, and won the Excellent Paper Award at the Japan Dialysis Conference in 2018.
Member of the Chinese Non-public Kidney Disease Committee, Youth Member of the Changsha Medical Association Kidney Disease Society. Council Member of the Hunan Health Association Kidney Health Branch. Member of the Hunan Traditional Chinese Medicine and Integrated Chinese-Western Medicine Kidney Disease Professional Committee. Council Member of the Hunan Health Service Association Organ Transplantation Branch.

Professor Lingjie
The Surgeon of This Case
Graduated from Nanhua University,Chief Resident of Nephrology Department, Changsha Jieao Hospital;Lecturer of Xiang Yijia Doctor Group Training Team.
Skilled in various vascular access procedures, parathyroidectomy operations, and postoperative maintenance.Care and management, well-versed in the complications of various kidney diseases and dialysis patientsDiagnosis and Treatment.

Department Introduction


Xiangyixia Nephrology Doctors Group, established in September 2015, is composed of medical staff and technicians from the nephrology and hemodialysis department of Xiangya Third Hospital and the Kidney Disease Center of the Second Affiliated Hospital of Nanjing Medical University. It is one of the few nephrology doctor groups in China.
Xiang Yijia Kidney Doctors Group currently has more than 20 core nephrology experts and kidney specialists. It also has 42 staff members, including blood purification specialists, nephrology follow-up professionals, educational nursing staff, and equipment engineers. The group operates six nephrology specialty hospitals and one hemodialysis center, located in Changsha (Hunan), Chaling (Hunan), Kaili (Guizhou), Shaoyang (Hunan), Nan County (Hunan), Longhui (Hunan), and Shaoguan (Guangdong). The seven hospitals under Xiang Yijia Doctors Group are designed as regional dialysis clinical support centers, providing medical, nursing, and technical support to independent hemodialysis centers. They address long-term dialysis complications in uremic patients, establish vascular access centers, and set up parathyroid surgery centers.
Xiang Yi Jia Nephrology Medical Group adheres to the service philosophy of "Providing Healthcare with Warmth" and is committed to creating high-quality dialysis services. The group specializes in various complex uremic vascular access surgeries, with extensive experience in managing vascular access complications, artificial catheter insertion, and maintenance. The number of lower limb instant-access artificial vascular graft implantations ranks internationally leading. Since 2015, the total number of parathyroidectomy with autotransplantation surgeries for uremic patients, which leads in Hunan Province, has reached nearly 2,000 cases, ranking among the top ten in China. Other features of the group’s dialysis technology include dialysis center construction, high-quality dialysis, nutrition related to dialysis, exercise therapy, and health education.
