Professor Yang Jun's Team Showcases Dissolve™ AV Scoring Drug-Coated Balloon for Recurrent AVF Neointimal Hyperplasia

DK Medtech
Vascular Interventional Balloon Product Developer

Stenosis of autologous/artificial arteriovenous fistula (AVF/AVG) is the most common complication in hemodialysis patients. Percutaneous transluminal angioplasty (PTA) has become the primary method for maintaining dialysis access. However, the blunt and irregular tearing of the intima and part of the media by traditional balloons during PTA excessively damages the endothelial vessels, causing intense proliferation of vascular smooth muscle cells and macrophages, which rapidly leads to restenosis.
In recent years, there has been continuous international exploration and clinical research on drug-coated balloons and other devices for PTA treatment of dialysis access. DK Medtech has developed the Dissolve™ AV Scoring Drug Balloon, which integrates three features: "scoring," "high pressure," and "drug coating." This is the world's first third-generation drug balloon:
Directional Scoring: Uniform and regular tearing of the intima to reduce damage from blunt splitting.
High Burst Pressure: For high-resistance lesions, improving technical success rate.
Paclitaxel Coating: Effectively Inhibits Excessive Proliferation of Smooth Muscle Cells.
DK Medtech Special Release【Professor Yang Jun's Team: Scored Drug-Coated Balloon for the Treatment of Recurrent AVF Intimal Hyperplastic Stenosis】Case Presentation, demonstrating the precise operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized procedures and technical applications during surgery, complication prevention, perioperative management, and other aspects, the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.

Scored Drug-Coated Balloon Therapy
Recurrent AVF Intimal Hyperplastic Stenosis

Yang Jun, First Affiliated Hospital of Xinxiang Medical University
Patient Information
Basic Information:Female, 34 years old.
Chief Complaint:Elevated blood creatinine for 12 years, arteriovenous fistula stenosis detected in half a day.
History of Present Illness:Elevated serum creatinine was found during a physical examination 12 years ago, with the highest level reaching 390 umol/L. There were no symptoms of nausea, vomiting, hematuria, or foamy urine. The patient intermittently took medication and did not undergo regular follow-up examinations during this period. Over four years ago, the patient visited the local county hospital due to nausea and vomiting. Renal function tests showed a creatinine level of 900 umol/L. After ruling out surgical contraindications, the patient underwent "autologous arteriovenous fistula formation + long-term internal jugular vein catheter placement" in September 2019. After discharge, the patient received regular hemodialysis three times per week. Due to multiple instances of fistula stenosis, the patient underwent "arteriovenous fistula balloon angioplasty" on 2019-12-26, 2020-04-15, 2020-09-11, 2021-03-17, 2021-09-15, 2022-04-12, 2022-09-15, 2023-10-30, and 2024-03-20. A half-day ago, an outpatient ultrasound review revealed arteriovenous fistula stenosis, and the patient was admitted to our department. On 2024.7.3, the patient is scheduled to undergo treatment with a scoring drug-coated balloon.
Past Medical History:Hypertension for 5 years, currently treated with oral antihypertensive medication, blood pressure is under control.
Physical Examination:Increased pulsation and weakened thrill at the autologous arteriovenous anastomosis site in the left upper arm.
Admission Diagnosis:Stenosis of autologous arteriovenous fistula, chronic kidney disease stage 5, obstructive nephropathy, on hemodialysis, hypertension.
Previous interventional treatment
Time | Main Treatment Process | |
2019-12-26 | 7mm High-Pressure Balloon Catheter | |
2020-04-15 | 6mm Ultra-high Pressure Balloon Catheter | |
2020-09-11 | 6mm High-Pressure Balloon Catheter | |
2021-03-17 | 6mm Ultra-high Pressure Balloon Catheter | |
2021-09-15 | 6mm Ultra-high Pressure Balloon Catheter | |
2022-04-12 | 6mm Ultra-high Pressure Balloon Catheter | |
2022-09-15 | 6mm Peripheral Cutting Balloon Catheter | |
2023-05-15 | Drug-Coated Balloon (External Hospital) | |
2023-10-30 | 7mm Notched Balloon Catheter | |
2024-03-20 | 6mm Notched Balloon Catheter |
Preoperative Analysis
Preoperative Analysis:More than four years ago, the patient was hospitalized for arteriovenous fistula stenosis and low blood flow, and underwent balloon angioplasty of the artificial arteriovenous fistula. After the surgery, restenosis occurred intermittently at an average frequency of once every six months. The previous use of high-pressure balloon dilation had not been satisfactory for this patient. This hospitalization plans to treat the lesion with a high-pressure scoring drug-coated balloon.
Preoperative Assessment:Radial artery-cephalic vein arteriovenous fistula, with intimal hyperplastic stenosis at the outlet tract origin.

Surgical Objective:
Short-term Goals:Solve the problem of stenosis in patients' internal fistulas to meet the blood flow requirements for dialysis.
Secondary Objective:Prolong the restenosis time of patients' internal fistulas and reduce the number of interventions for patients.
Surgical Strategy/Plan:Use 6.0mm * 60mm DK Medtech Dissolve™ AV Scoring Drug-Coated Balloon and 5.0mm * 40mm Peripheral High-Pressure Balloon to dilate arteriovenous fistula stenosis.
Surgical Procedure
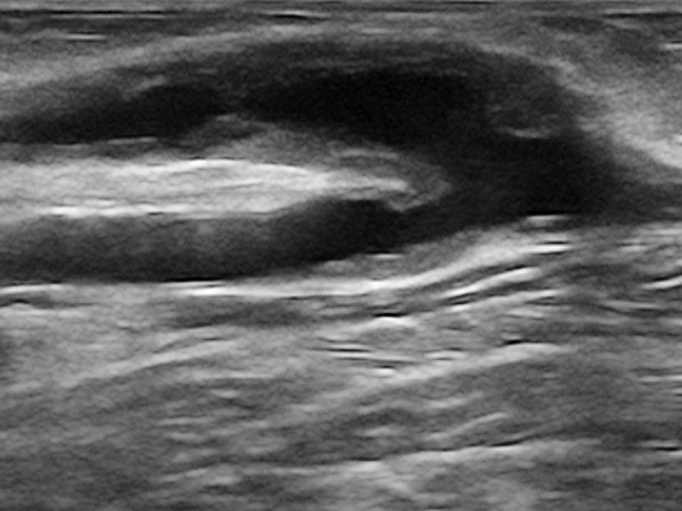
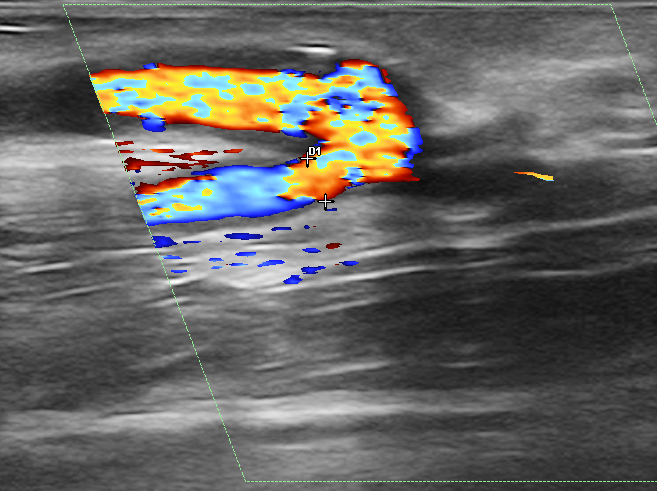
Preoperative assessment: Color Doppler ultrasound showed stenosis at the origin of the outflow tract in the left upper limb, with a minimum inner diameter of approximately 1.5mm, length of 37mm, and intimal thickness of 1.4mm.
The patient lies in the supine position, with the left forearm in external rotation. After routine disinfection and draping, 2% lidocaine is used for infiltration anesthesia on the venous outflow side near the elbow of the left arm. The puncture needle is inserted, and once the blood flow from the arteriovenous fistula is observed, the guidewire is advanced. The needle is withdrawn, the skin is dilated, and a 7F sheath is inserted. Heparin (20mg) is administered intravenously. The guidewire passes through the lesion.
Use 6.0mm * 60mmDK Medtech Dissolve™ AV Scoring Drug-Coated Balloon, the balloon reaches the lesion site, slowly inflating to 14atm, and continues to maintain pressure until 120s.
Stenosis improved in the late dilation phase, and pressure was released after 120 seconds.
After the balloon rotates 60°, it reaches the lesion site again and is expanded again at 14atm for 60 seconds.
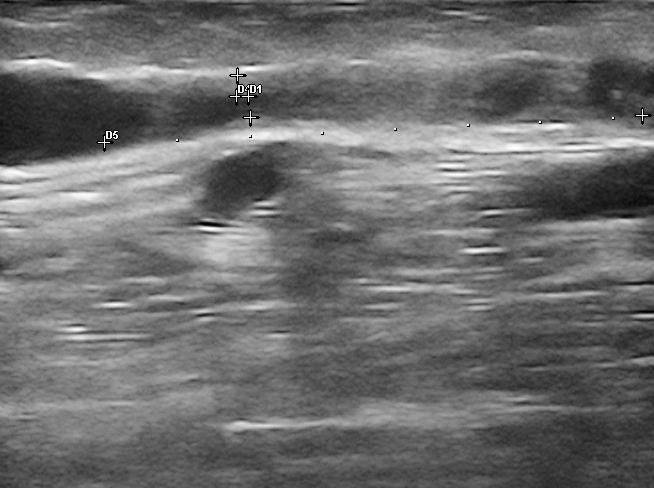
Assessment after dilation, postoperative inner diameter 4.1mm.
The puncture site was selected at the distal radial artery. After infiltration anesthesia with 2% lidocaine, the puncture needle was inserted. Upon observing the outflow of arteriovenous fistula blood, a guidewire was advanced, the needle was withdrawn, the skin was incised, a 5F sheath was inserted, and 20mg of heparin was administered intravenously.The guidewire passed through the lesion into the proximal radial artery.。
Use 5.0mm * 40mm peripheral high-pressure balloon, the balloon reaches the proximal end of the radial artery and is slowly pressurized to 8 atm for dilation, continuing to maintain pressure until 30 seconds.
The evaluation was performed after dilation, with the inner diameter increasing from 2.1mm preoperatively to 3.2mm postoperatively.
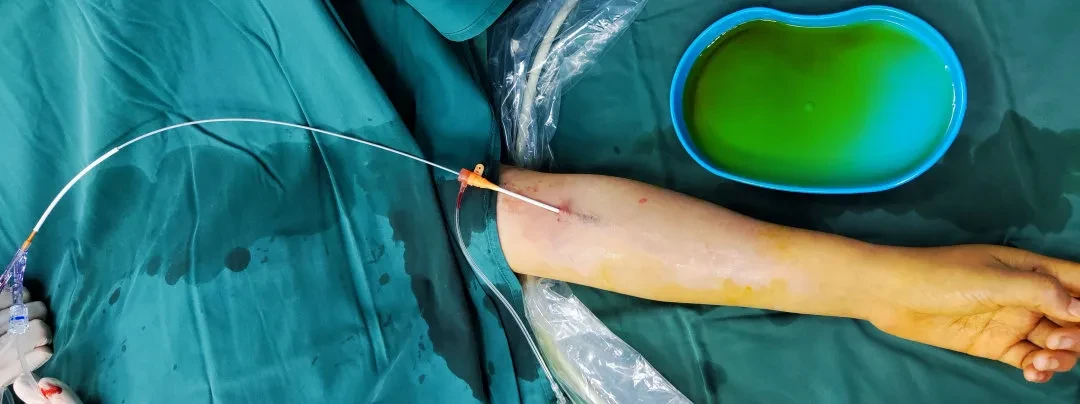

The scored drug-coated balloon and sheath used during the surgery showed a blood flow rate of 1688 ml/min measured by ultrasound on the first day after the operation.
Follow-up
Discharge Status:The patient was discharged smoothly, and the blood flow of the arteriovenous fistula met the requirements for dialysis in the local area. In August, a follow-up examination showed intimal thickening, with the distal cephalic vein measuring 3.7mm and a flow rate of 1574ml/min.
Case Summary
Preoperative Assessment Key Points:Preoperative ultrasound evaluation showed that the color Doppler ultrasound revealed stenosis at the starting segment of the outflow tract in the left upper limb, with the narrowest inner diameter of approximately 1.5mm, intima thickness of 1.4mm, and fistula flow rate of 320ml/min.
Surgical Strategy/Technical Key Points:
In December 2019, this patient underwent balloon angioplasty for arteriovenous fistula stenosis. The effect was not ideal after using a high-pressure balloon for dilation, and the stenosis recurred during this period.
DK Medtech Dissolve™ AV Scoring Drug-Coated BalloonIn addition to having high-pressure characteristics, the dilatation catheter is equipped with a scoring element on its surface that focuses pressure through scoring, effectively and regularly incising the intima and fibrous annulus, enhancing dilatation efficiency, and increasing lumen gain. Its balloon surface is coated with paclitaxel, which can effectively inhibit intimal hyperplasia at the lesion site and improve long-term patency rates.
In this case, it can be seen that the lesion was fully opened when pressurized to 14atm.
Device Features / Usage Tips:
DK Medtech Dissolve™ AV Scoring Drug-Coated BalloonThe dilatation catheter is equipped with three nickel-titanium alloy triangular scribed components on its surface, and the balloon surface is coated with a paclitaxel drug layer. After adequately dilating the lesion, paclitaxel is used to inhibit the hyperplastic intima. In this case, after using the balloon once, the balloon was rotated approximately 60 degrees and then used again to dilate the lesion, allowing for more thorough treatment of the stenotic lesion.
DK Medtech Dissolve™ AV Scoring Drug-Coated BalloonDuring the use of the dilation catheter, attention should be paid to the process: when pressurizing up to 8 atm, increase by 2 atm every 3 seconds. Do not increase pressure too quickly to prevent complications such as vascular rupture and dissection to the greatest extent.
For lesions that are resistant to initial dilation, maintaining the burst pressure for a period of time can fully utilize the role of the scoring wire, and there is still an opportunity to completely dilate the stenosis.

Expert Introduction


Professor Yang Jun
The Surgeon of This Case
Chief Physician, Director of the Blood Purification Unit at the Kidney Disease Hospital of the First Affiliated Hospital of Xinxiang Medical University. Concurrently serves as a committee member of the Nephrology and Blood Purification Branch of the Chinese Research Hospital Association, committee member of the Blood Purification Branch of the Henan Medical Association, committee member of the Blood Purification Quality Control Committee of the Henan Physician Association, committee member of the Renal Pathology Branch of the Henan Medical Association, Chairman of the Blood Purification Branch of the Xinxiang Medical Association, and Vice Chairman of the Blood Purification Quality Control Committee of the Xinxiang Medical Association. Has led and participated in 2 provincial and ministerial level research projects, 2 joint construction projects, and 1 artificial liver project. Published 4 SCI articles, over 10 core journal articles, and authored 1 monograph.

Department Introduction

Hemodialysis Unit I of the Nephrology Hospital was established in 1982 as the earliest department specializing in hemodialysis in Henan Province. It has now grown to include 31 hemodialysis machines, 5 hemofiltration machines, 2 ARTTs, 1 hemoperfusion machine, 12 CRRT machines, and 1 dual reverse osmosis water treatment system. In 2013, it was designated as a national hemodialysis training base for county-level hospitals by the Medical Service Supervision Department of the Ministry of Health and the Nephrology Physicians Branch of the Chinese Medical Doctor Association. In August 2017, it became a member unit of the Henan Hemodialysis Alliance, and in December 2017, a member unit of the Henan CRRT Alliance. On June 26, 2021, it was approved as a national demonstration center for artificial liver and blood purification technology under the "One City, One Center" initiative. The department specializes in the establishment and maintenance of vascular access and performs procedures such as balloon angioplasty for arteriovenous fistulas guided by DSA or ultrasound, and long-term dialysis catheter replacement guided by DSA or ultrasound. The department currently has 8 physicians and 32 nursing staff, including 2 senior title holders, 15 intermediate title holders, and 18 junior title holders, with 6 master's degree holders. The team is composed of a professional and technically proficient blood purification workforce with personnel at various levels of high, middle, and primary technical ranks.
