Professor Xu Liyun's Team: Breaking Through Resistance and Extending Patency – Integrated Management of Refractory AVF Stenosis

DK Medtech
Vascular Interventional Balloon Product Developer

Stenosis of autologous/artificial arteriovenous fistula (AVF/AVG) is the most common complication in hemodialysis patients. Percutaneous transluminal angioplasty (PTA) has become the primary method for maintaining dialysis access. However, the blunt and irregular tearing of the intima and part of the media by traditional balloons during PTA can cause excessive damage to the endothelial vessels, leading to intense proliferation of vascular smooth muscle cells and macrophages, which rapidly results in restenosis.
In recent years, there has been continuous international exploration and clinical research on drug-coated balloons for PTA treatment of dialysis access. DK Medtech has developed the Dissolve™ AV Scoring Drug-Coated Balloon, which integrates three features—"scoring," "high-pressure," and "drug-coating"—into one device, making it the world's first third-generation drug-coated balloon:
Directional Scoring: Uniform and regular tearing of the intima to reduce damage from blunt splitting.
High Burst Pressure: For high-resistance lesions, improving technical success rate.
Paclitaxel Coating: Effectively Inhibits Excessive Proliferation of Smooth Muscle Cells.
DK Medtech Special ReleaseProfessor Xu Liyun's Team: Breaking Through and Extending Efficacy —— A Case Study of Refractory Stenosis in Arteriovenous Fistula, demonstrating the precise operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized procedures during surgery, technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.

Breaking through hardness and prolonging effects, combining near and far.
Refractory Stenosis of Arteriovenous Fistula
Xu Liyun, Zhou Lingling, Taizhou Hospital of Zhejiang Province

Patient Information
Basic Information:Patient, female, 75 years old.
Chief Complaint:Maintenance hemodialysis for over 5 years, found weakened bruit of arteriovenous fistula 3 days ago.
History of Present Illness:Five years ago, the patient was diagnosed with stage 5 chronic kidney disease (CKD) at our hospital. Initially, a temporary catheter was placed in the right femoral vein for hemodialysis treatment, followed by the creation of an "arteriovenous fistula in the left forearm + placement of a cuffed long-term catheter in the right internal jugular vein." A dual-lumen cuffed catheter was used as the vascular access. In December 2018, the patient began hemodialysis using the native arteriovenous fistula. However, the patient repeatedly experienced low blood flow during hemodialysis. Further examination revealed significant stenosis of the arteriovenous fistula. During this period, the patient was hospitalized in our department and underwent multiple fistula repair surgeries, which improved blood flow postoperatively. The most recent fistula repair surgery was performed on September 11, 2023. On November 20, 2023, the patient noticed the disappearance of the bruit in the left upper limb arteriovenous fistula, indicative of acute thrombosis. Subsequently, the patient underwent surgical thrombectomy and balloon angioplasty, resulting in stable hemodialysis post-surgery. Three days prior to admission, the patient noticed weakened bruit and prominent pulsation in the arteriovenous fistula. Ultrasound examination revealed stenosis in the outflow tract of the basilic vein. The patient was admitted with diagnoses of "left upper limb arteriovenous fistula stenosis and stage 5 chronic kidney disease."
Past Medical History:History of gout, hypertension, hypertensive heart disease, peripheral arterial atherosclerosis, and pulmonary hypertension.
Physical Examination:Blood pressure 130/93 mmHg, pulse 79/min, ear temperature 36.5°C, regular heart rhythm, no pathological murmurs heard. Clear breath sounds in both lungs, no dry or wet rales heard. Soft abdomen, no tenderness or rebound pain, liver and spleen not palpable below the ribs. No edema in both lower limbs. Reduced bruit and enhanced pulsation of the arteriovenous fistula in the left forearm.
Admission Diagnosis:
Stenosis of Left Upper Limb Arteriovenous Fistula
Chronic Kidney Disease Stage 5
Hypertensive Nephropathy
Hemodialysis Status
Secondary Hyperparathyroidism
Previous interventional treatment
Time | Main Treatment Process |
2018.8.23-8.30 | Temporary hemodialysis catheter in the right femoral vein, AVF in the left upper limb + TCC in the right internal jugular vein (removed on 2018.3.18) |
2018.8.29-2020.12.7 | Anastomotic stenosis, with five episodes of stenosis during this period |
2021.3.29-2022.8.10 | Stenosis in the outflow tract to the middle segment of the cephalic vein in the upper limb, with five occurrences of stenosis during this period. |
2022.10.26-2023.3.15 | Thrombosis in the cephalic vein outflow tract, anastomosis of the distal cephalic vein and basilic vein, with five instances of stenosis during the process. |
2023.3.15-Present | Stenosis at the Junction of the Cephalic Vein and Basilic Vein |
Preoperative Analysis
Preoperative Analysis:Distal radial artery occlusion, with stenosis approximately 50 mm long at the elbow crease (vascular transposition site) in the outflow tract of the arteriovenous fistula.mm, A length of approximately 30 was observed in the cephalic vein at the mid-forearm.mmThe stenotic segment.
Surgical Objective:
Main Objectives:Dilate stenotic vessels, blood flow reaches 250ml/min;
Secondary Objectives:The narrow inner diameter can be expanded to 3.5mm.
Surgical Strategy/Plan:First, use an ultra-high-pressure balloon to dilate the narrowed area; if the effect is not good, switch toDissolve™ AV Scoring Drug-Coated Balloon。
Surgical Procedure
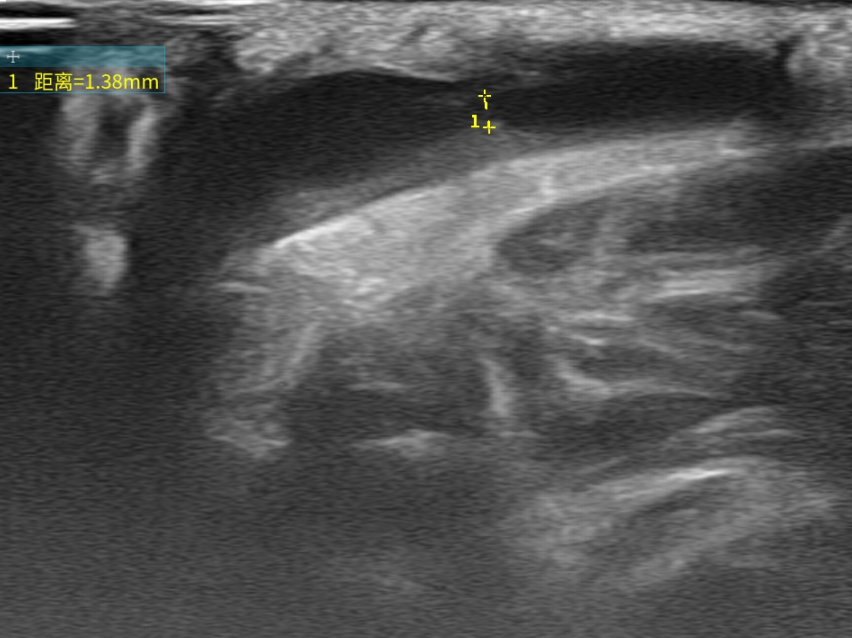
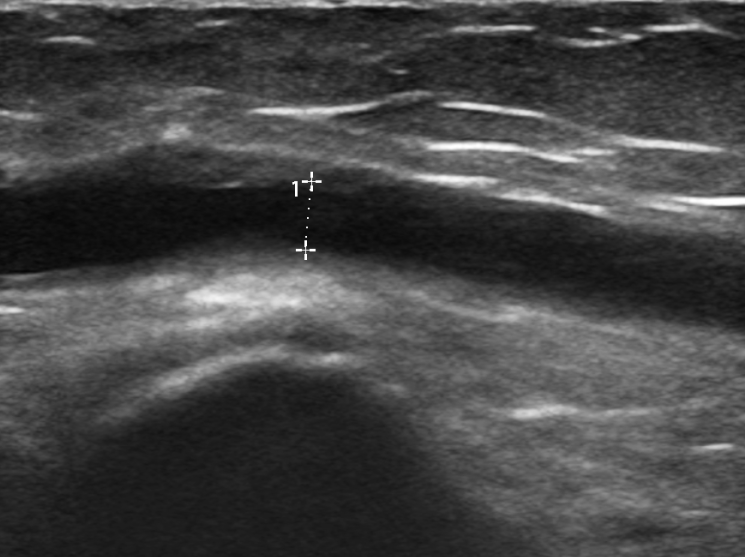
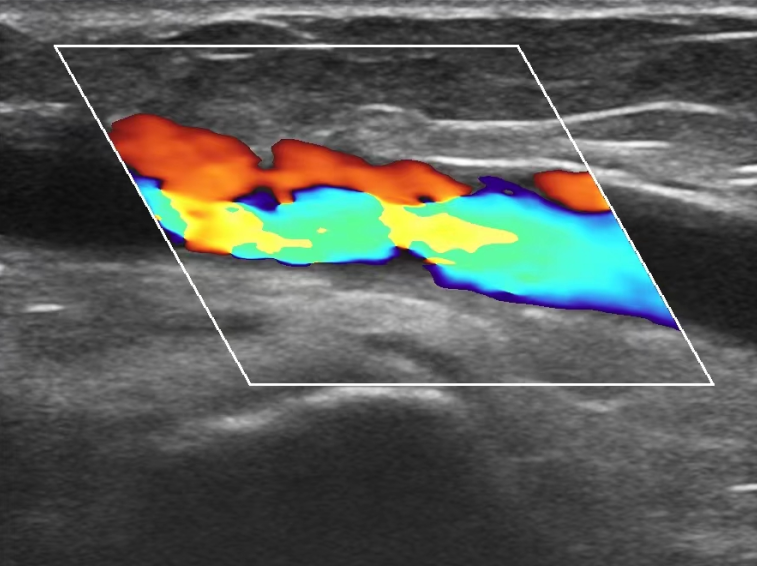
Target Lesion Stenosis Location
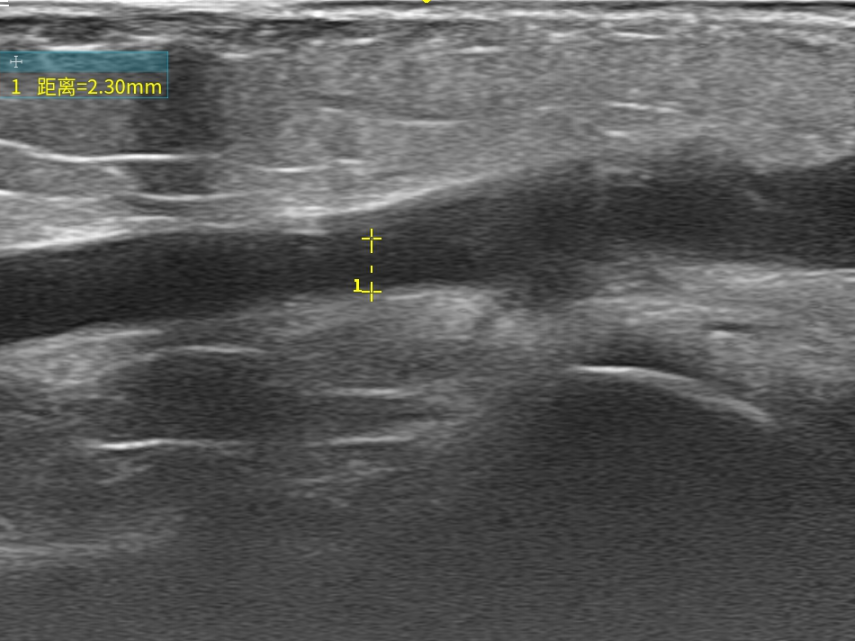
Use Bard 6mm×40mmThe vascular diameter after the use of the ultra-high pressure balloon was 2.30mm.
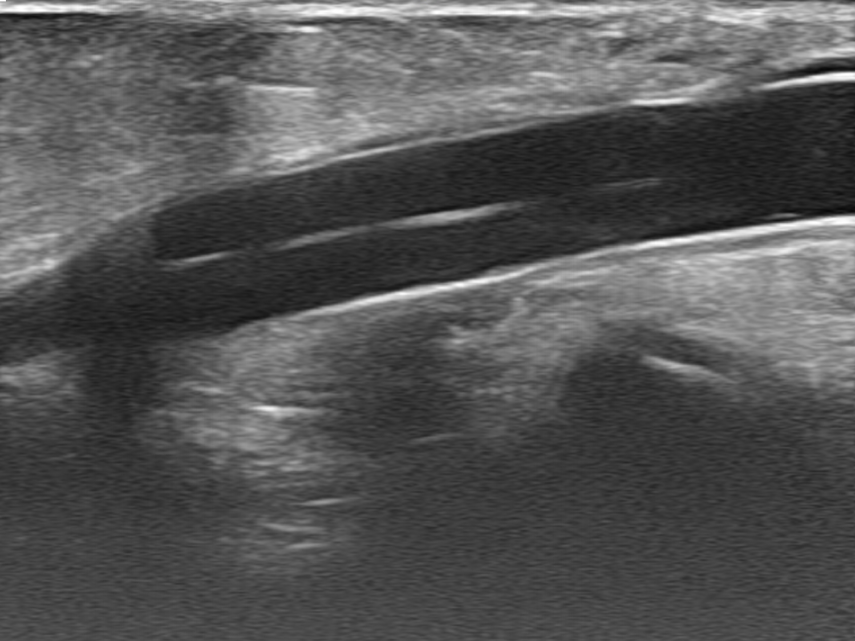
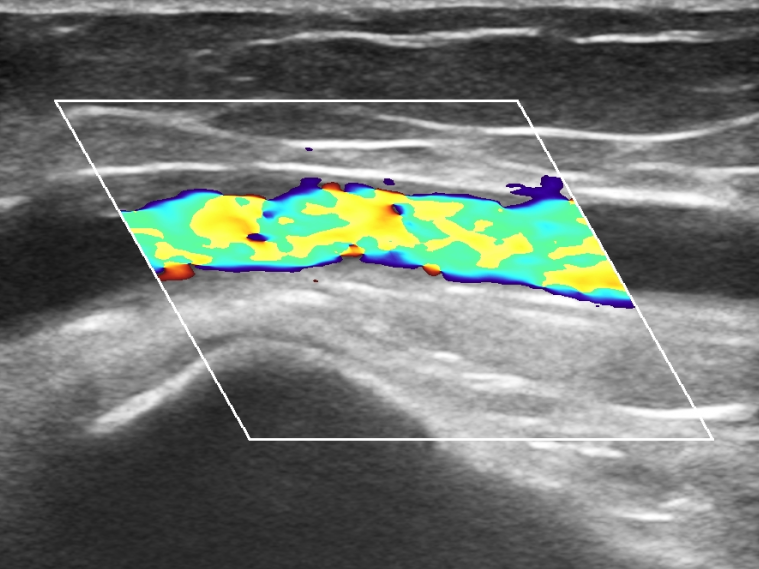
Using DK Medtech 6mm×60mmDissolve™ AV Scoring Drug-Coated Balloon Imaging
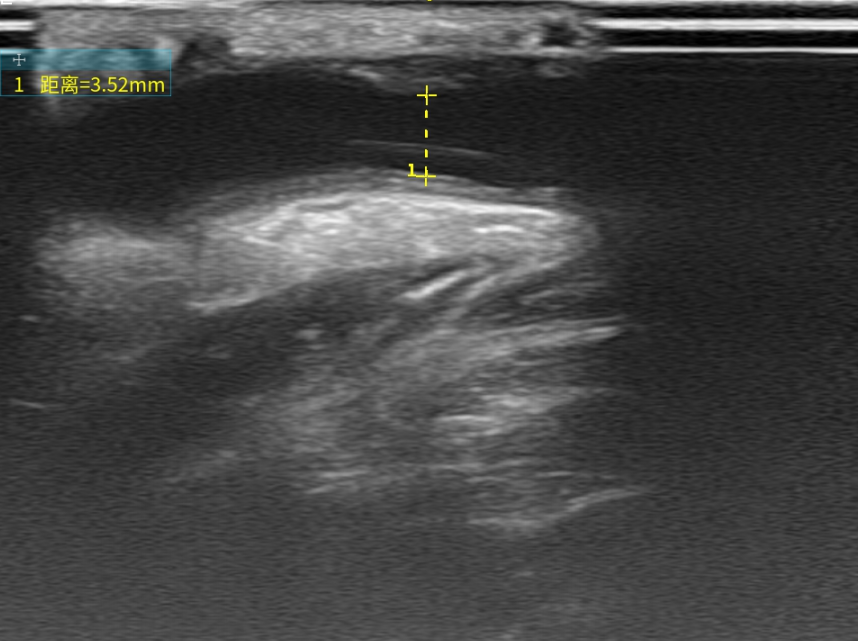
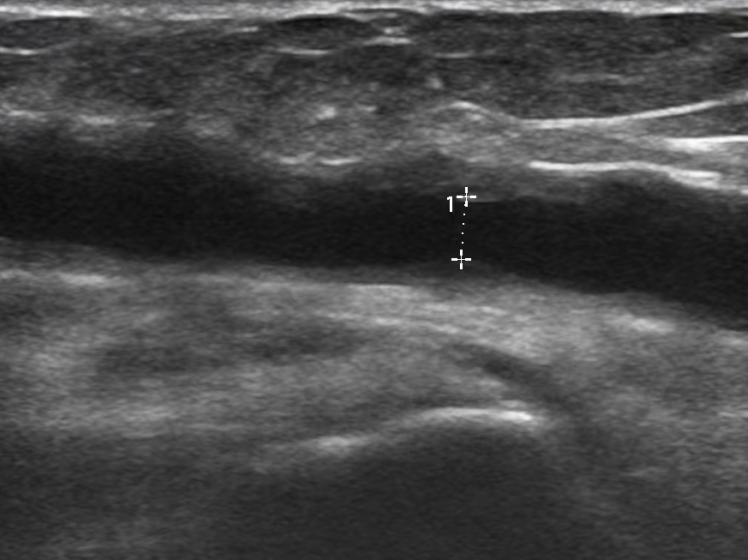
Use DK MedtechDissolve™ AV Scoring Drug-Coated BalloonThe diameter of vascular dilation after was 3.52mm.
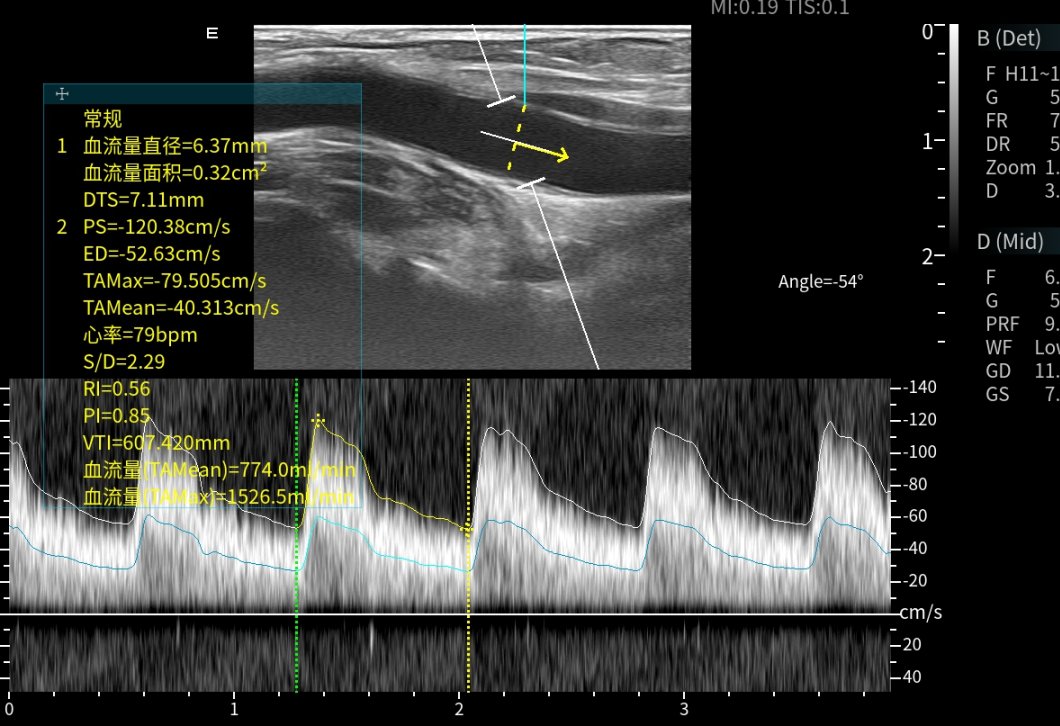
Postoperative Brachial Artery Blood Flow
Follow-up
Discharge Status:The arteriovenous fistula in the left forearm had a loud murmur and palpable thrill, with no local exudate and dry, clean dressing. The blood flow rate during the first hemodialysis after the surgery was 250ml/min.
Two-month postoperative follow-up:
Diameter of Lesion Site Three Months Post-Operation
Postoperative Lesion Location Flow
The diameter of the lesion site was 2.5 cm two months after the surgery.mm
Postoperative Lesion Location Flow
Case Summary
Case Characteristics:The patient has been on hemodialysis for 5 years, with more than 10 balloon dilation procedures performed due to stenosis and thrombosis of the arteriovenous fistula in the left forearm, and the vascular condition is poor.
Preoperative Assessment Key Points:Distal radial artery occlusion, with stenosis approximately 50 mm long at the elbow crease (vascular transposition site) in the outflow tract of the arteriovenous fistula.mm, A length of approximately 30 was observed in the cephalic vein at the mid-forearm.mmThe stenotic segment.
Surgical Strategy/Technical Key Points:CONQUEST 6mm×40mm balloon, under ultrasound guidance, entered the venous outflow tract stenosis segment, and was dilated multiple times at pressures of 30atm and 30atm respectively. The vascular stenosis was dilated to 2.3mm, with suboptimal dilation.
Features/Usage Tips of the Device:Change to DK MedtechDissolve™ AV Scoring Drug-Coated Balloon6mm×60mm, the blood vessels dilated well. Repeat B-ultrasound showed brachial artery blood flow of 774ml/min, resistance index of 0.56, and the narrowest point expanded to 3.5mm.

Expert Introduction


Dr. Xu Liyun, Chief Physician
Surgical Guidance
Chief Physician of the Department of Nephrology, Taizhou Hospital of Zhejiang Province,Head of the Hemodialysis Vascular Access Center;Member of the Vascular Access Group, Nephrology Branch, Zhejiang Provincial Medical Association;Member of the Hemodialysis Access Expert Committee, China Branch of the International Vascular Access Alliance;Member of the Vascular Access Professional Committee of the China Ambulatory Surgery Alliance for Dialysis;Member of the Nephrology Branch of the Zhejiang Mathematical Medicine Association;Member of the Taizhou Medical Association's Nephrology Branch.

Zhou Lingling, Master
Surgeon of This Case
Attending Doctor of Nephrology Department, Taizhou Hospital;Master of Nephrology, Wenzhou Medical University;Attending Doctor of the Vascular Access Team, Department of Nephrology, Taizhou Hospital of Zhejiang Province.With over 10 years of experience in vascular access, specializing in the establishment and maintenance of vascular access, as well as the management of severe complications such as central venous stenosis.Youth Committee Member of Taizhou Medical Association.

Department Introduction

The Blood Purification Center of Taizhou Hospital in Zhejiang Province was established in 1988. It currently has three dialysis treatment centers, with 186 hemodialysis machines and is equipped with an internationally advanced purified water treatment system. The center provides an annual hemodialysis service capacity of approximately 100,000 cases and performs over 1,500 vascular access surgeries. Specialized techniques include plasma exchange, immunoadsorption, hemoperfusion, CRRT, parathyroidectomy and transplantation, parathyroid radiofrequency ablation, arteriovenous fistula protection techniques (such as red light therapy, ladder puncture technique, fixed-point puncture), as well as the establishment, maintenance, and repair of various complex vascular accesses.
Hemodialysis Access CenterFounded in 2016, starting from the insertion of the first tunneled dialysis catheter with a polyester cuff in 2003, the center now routinely performs autologous arteriovenous fistula surgery, autologous fistula repair surgery, great saphenous vein transplantation, artificial vessel transplantation, endovascular treatment for arteriovenous fistula stenosis under DSA, ultrasound-guided arteriovenous fistula balloon dilation and thrombectomy, among others. Since 2017, the Vascular Access Center of Taizhou Hospital has voluntarily carried out the "Vascular Access Screening for Uremic Hemodialysis Patients in Taizhou City" project, providing support and promoting vascular access-related medical techniques to grassroots hospitals. In 2023, the center completed over 1,500 surgeries, ranking 2nd in the DRG evaluation of tertiary hospitals in Zhejiang Province for the "Uremia + Percutaneous Transluminal Vascular Access Formation" procedure over the past two years.
