FcRH5-Targeted Therapy Cevostamab Advances to Phase 3 for Relapsed/Refractory Multiple Myeloma

Roche
Oncology Drug Research, Development, and Manufacturing
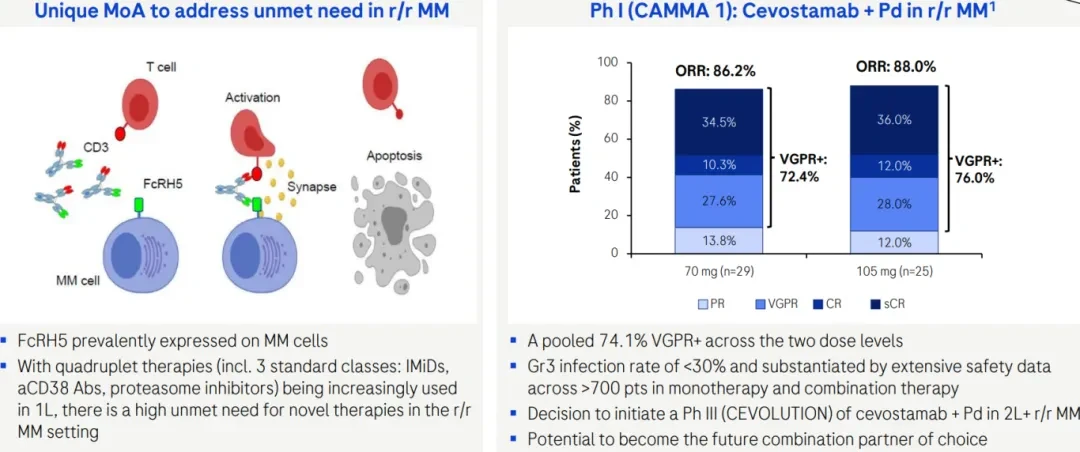
On September 22, 2025, Roche announced at the 2025 Pharma Day event that the FcRH5×CD3 bispecific antibody Cevostamab has entered Phase 3 clinical trials (CEVOLUTION). The trial is expected to commence in 2026, aiming to evaluate the efficacy of Cevostamab in combination with Pd (pomalidomide and dexamethasone) for treating patients with second-line or higher relapsed/refractory multiple myeloma (2L+r/r MM). During the event, Roche also highlighted Phase 1 CAMMA1 data, showing that Cevostamab achieved ORRs of 86.2% and 88% at two dose levels (70mg and 105mg), respectively. Additionally, both as monotherapy and in combination therapy, the Grade 3 infection rates were below 30%, demonstrating favorable safety. Roche believes Cevostamab has the potential to become the preferred combination therapy partner in this treatment area in the future.
Multiple Myeloma (MM) is a hematological malignancy originating from plasma cells in the bone marrow. Its pathogenesis involves the malignant transformation and abnormal proliferation of bone marrow plasma cells, leading to excessive production of monoclonal immunoglobulins, which causes clinical complications such as bone lesions, renal failure, anemia, and hypercalcemia.[1]In the past few decades, novel drugs such as proteasome inhibitors, immunomodulatory agents, and monoclonal antibodies have significantly improved remission rates and overall survival in patients with multiple myeloma (MM). Currently, the median overall survival for MM patients is 5 years. Among low-risk stage I patients, 82% can survive up to 5 years; however, most stage I patients will eventually develop drug resistance, become refractory to treatment, and progress to high-risk status. In contrast, only 40% of high-risk stage III patients survive 5 years, as these patients often show no response to initial treatment or experience early relapse.[2][3]. This shows that the recurrence of MM is an inevitable outcome, indicating that the current primary strategy for treating MM is to explore new targets to extend the survival period of patients with multiple myeloma.[4]。
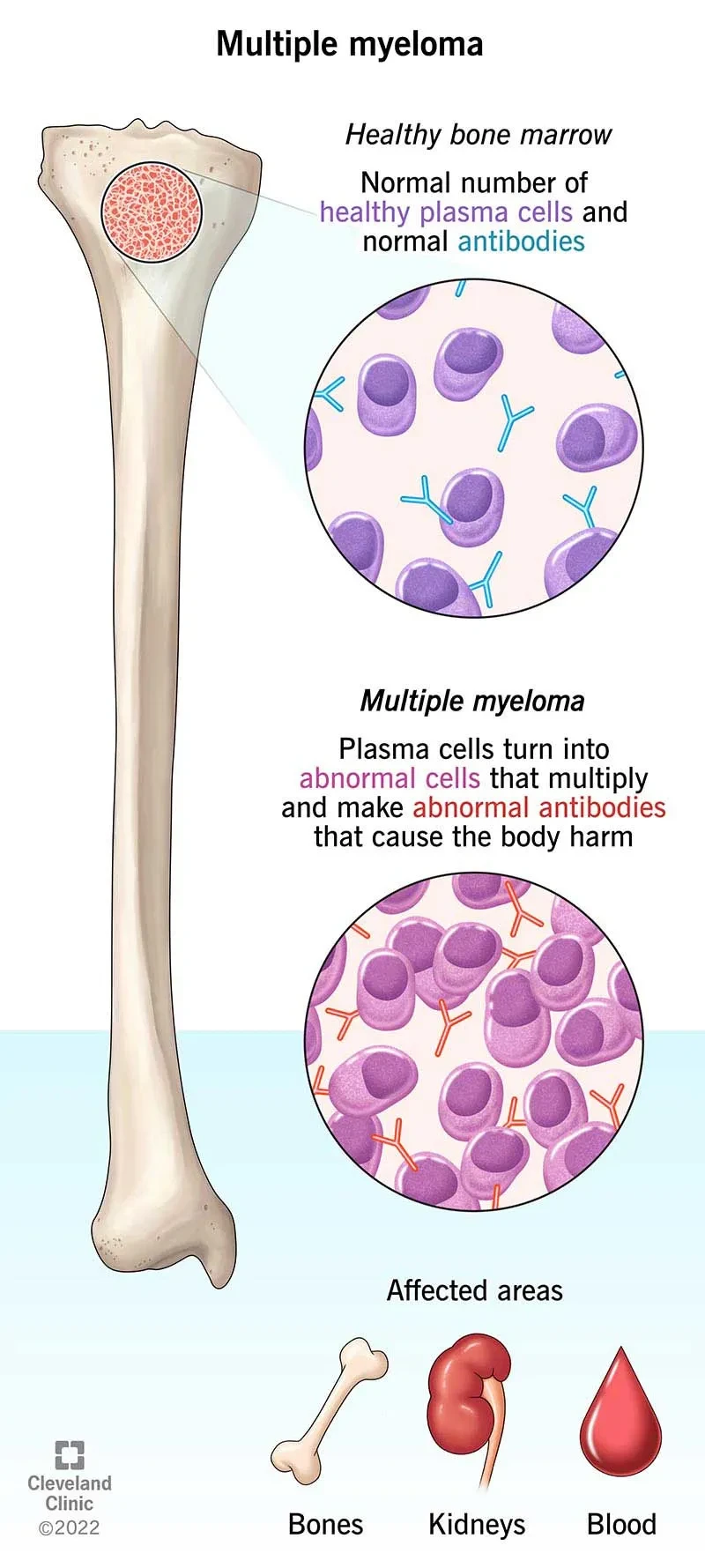
Illustration of Multiple Myeloma[5]
FcRH5, also known as FcRL5, IRTA2, or CD307, is located at the chromosomal breakpoint of 1q21. FcRH5 is exclusively expressed in the B-cell lineage, appearing from the pre-B cell stage of B-cell development, and its expression level gradually increases as B cells mature step by step. This process continues until B cells develop into naïve B cells and further differentiate into plasma cells.[6]。
FcRH5 is a type I transmembrane glycoprotein belonging to the immunoglobulin superfamily (IgSF), encoding 977 amino acids, with its extracellular segment containing 9 Ig-like domains, and its intracellular portion containing 1 immunoreceptor tyrosine-based activation motif (ITAM) and 2 inhibitory motifs (ITIM).[7]FcRH5 plays a dual role in regulating B-cell activity, capable of both activating and suppressing immune responses. When FcRH5 is cross-linked with the B-cell antigen receptor (BCR), it can recruit SHP-1 (protein tyrosine phosphatase) via its ITIM, reducing the level of tyrosine phosphorylation to prevent excessive immune activation; conversely, FcRH5 can also promote B-cell activation and differentiation. After co-stimulation with BCR, FcRH5 can enhance the proliferation and differentiation of naïve B cells, and this activating function is associated with the recruitment of Lyn (a Src family kinase) to the ITAM of FcRH5. The balance between activating and inhibitory signals, mediated by molecules such as SHP-1 and Lyn, determines the outcome of B-cell activation and contributes to maintaining immune homeostasis. However, when FcRH5 expression becomes dysregulated, it may contribute to the development of B-cell malignancies.[8]. The study found that the expression level of FcRH5 in plasma cells of MM patients was significantly higher than that in normal B cells.[4]Flow cytometry analysis showed that FcRH5 was more universally expressed than GPRC5D and BCMA in bone marrow plasma cell samples from MM patients.[9], FcRH5 has thus been identified as another potential target for the treatment of MM.
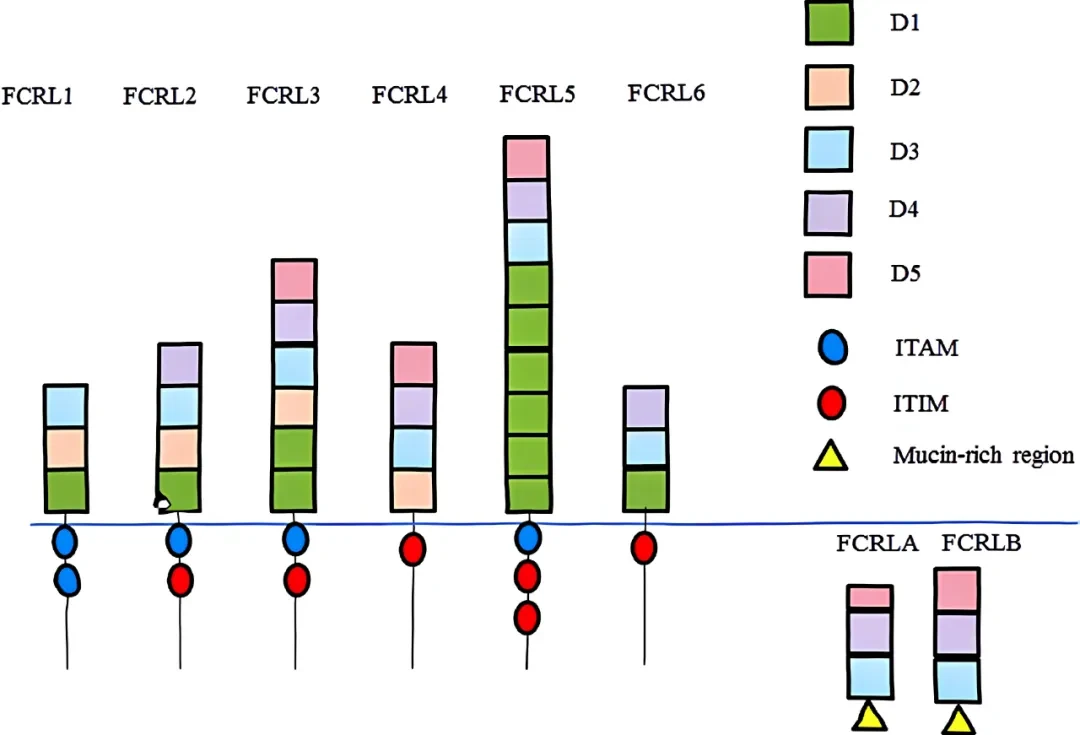
FcRH Protein Structure[7]
The FcRH5 gene has three different mRNA subtypes (FcRH5a, FcRH5b, and FcRH5c), where FcRH5c is the transmembrane protein mentioned earlier; FcRH5a is a secreted protein containing 8 Ig-like domains and 13 unique polar amino acids at the C-terminus; FcRH5b is a glycosylphosphatidylinositol (GPI)-anchored membrane protein with a peptide segment containing a GPI attachment signal (32 amino acids) following its first 6 Ig-like domains. Based on the structural characteristics of the three different subtypes, the Ig-like domain 9 becomes the unique extracellular domain of FcRH5.[10]In addition, studies have shown that malignant plasma cells in MM patients secrete large amounts of soluble FcRH5a, further suggesting that therapeutic antibodies should specifically target the lg-like domain 9 of the transmembrane form FcRH5c.
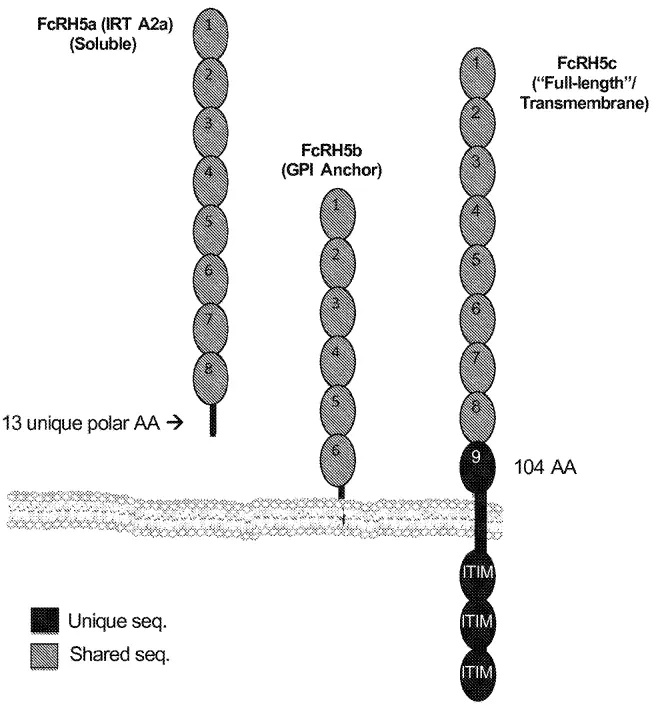
Three Different Subtypes of FcRH5[10]
The clinical termination of RG-7598 (DFRF4539A) also confirms the importance of targeting the lg-like domain 9. This ADC drug, developed by Genentech, targets FcRH5 and had entered Phase I clinical trials, demonstrating significant efficacy in xenograft models. However, clinical results showed a generally low response rate among patients. One reason for the failure of DFRF4539A is the elevated levels of soluble FcRH5a in the blood of multiple myeloma patients, which may reduce the binding of DFRF4539A to transmembrane FcRH5c, thereby affecting the drug's efficacy.[11]. The clinical failure of this drug provided important insights for the epitope design of subsequent FcRH5 drugs.
Currently, the drug types targeting FcRH5 mainly focus on T cell-dependent bispecific antibodies (TDB), ADCs, and CAR-T. The most advanced in progress is Cevostamab (BFCR4350A) mentioned earlier, which is a TDB drug targeting the membrane-proximal domain of FcRH5 on myeloma cells and CD3 on T cells. During the antibody development process, researchers designed three TDBs targeting different regions of FcRH5 (membrane-proximal region, central region, and distal region) (as shown in the figure below). The research results showed that the epitope of the membrane-proximal domain is essential for the formation of an effective immunological synapse and the exertion of cytotoxic effects by the anti-FcRH5×CD3 TDB.[1]A preliminary clinical activity and safety trial showed that Cevostamab monotherapy demonstrated potential efficacy in heavily pretreated patients with relapsed/refractory multiple myeloma (R/R MM).[4]。
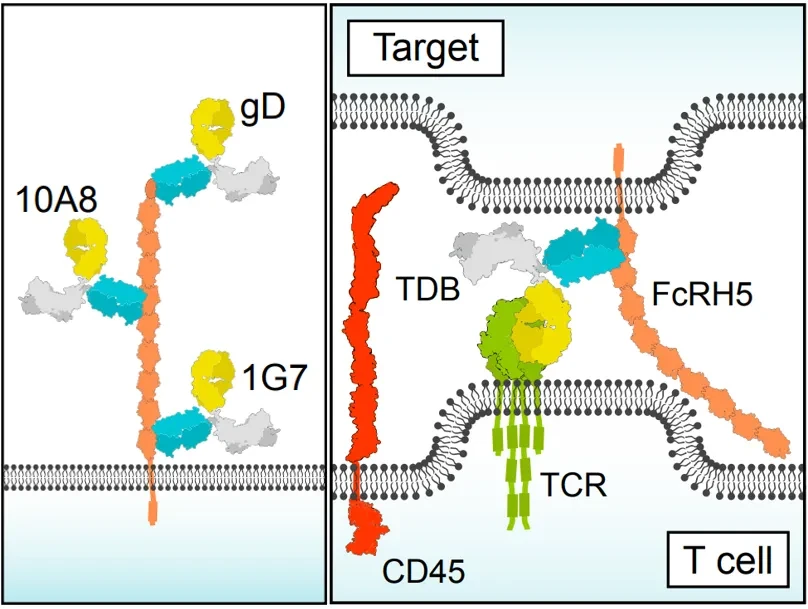
Cevostamab Recognizes the Membrane-Proximal Domain of FcRH5[1]
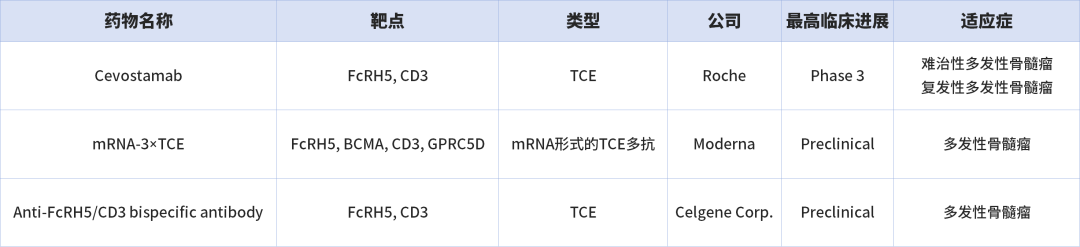
Some FcRH5-Targeted Drugs
FcRH5, as a highly promising therapeutic target for MM, offers more selectivity and possibilities for the treatment of MM.Kactus Biosystems supplies high-quality FcRH5 and FcRH5 transmembrane domain proteins, covering multiple species and various tag designs. During the antibody development process, in addition to using the full-length extracellular region of FcRH5, the transmembrane domain protein can also be used for immunization and screening to obtain more potent antibodies.
Data Example:
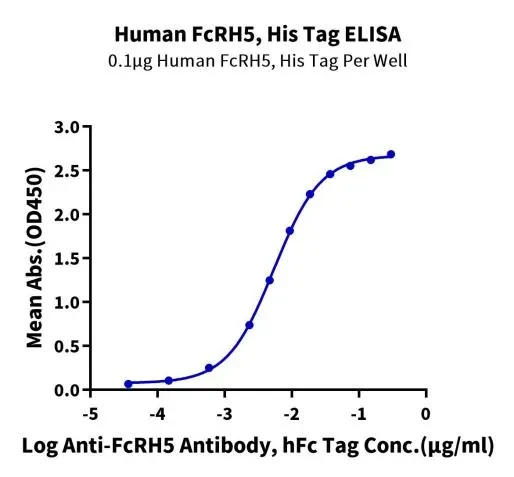
Immobilized Human FcRH5, His Tag at 1 μg/ml (100 μl/well) on the plate. Dose response curve for Anti-FcRH5 Antibody, hFc Tag with the EC50 of 5.4 ng/ml determined by ELISA (QC Test).
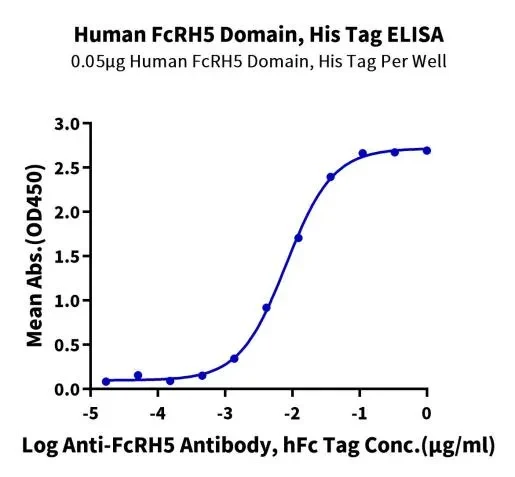
Immobilized Human FcRH5 Domain, His Tag at 0.5 μg/ml (100 μl/well) on the plate. Dose response curve for Anti-FcRH5 Antibody, hFc Tag with the EC50 of 8.1 ng/ml determined by ELISA (QC Test).
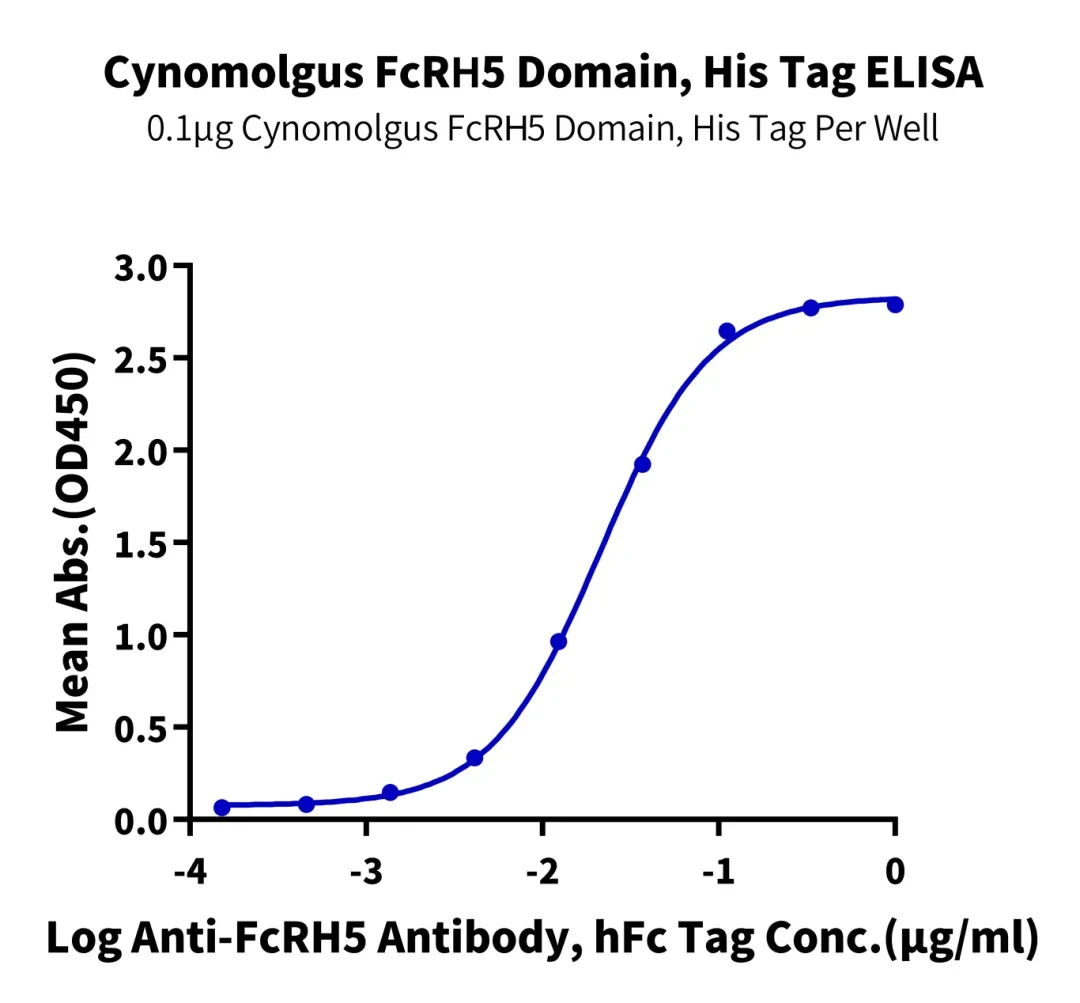
Immobilized Cynomolgus FcRH5 Domain, His Tag at 1 μg/ml (100 μl/well) on the plate. Dose response curve for Anti-FcRH5 Antibody, hFc Tag with the EC50 of 21.3 ng/ml determined by ELISA (QC Test).
Product List:
FCR-HM10D | Human FcRH5 Domain Protein | ||
FCR-HM20D | Human FcRH5 Domain Protein | ||
References:
[1] Li, Ji et al. “Membrane-Proximal Epitope Facilitates Efficient T Cell Synapse Formation by Anti-FcRH5/CD3 and Is a Requirement for Myeloma Cell Killing.” Cancer cell vol. 31,3 (2017): 383-395. doi:10.1016/j.ccell.2017.02.001
[2] Palumbo A, Avet-Loiseau H, Oliva S, Lokhorst HM, Goldschmidt H, Rosinol L, et al. Revised international staging system for multiple myeloma: a report from international myeloma working group. J Clin Oncol. (2015) 33:2863-9. doi: 10.1200/JCO.2015.61.2267
[3] Avet-Loiseau H. Ultra high-risk myeloma. Hematol Am Soc Hematol Educ Program. (2010) 2010:489–93. doi: 10.1182/asheducation-2010.1.489
[4] Cheng, Linyan et al. “Efficacy and safety of bispecific antibodies vs. immune checkpoint blockade combination therapy in cancer: a real-world comparison.” Molecular cancer vol. 23,1 77. 16 Apr. 2024, doi:10.1186/s12943-024-01956-6
[5] Multiple Myeloma: Signs and symptoms, Causes, Stages, Types, Diagnosis and Treatment options - Page 4 of 6 - TheLifeToday
[6] Polson AG, Zheng B, Elkins K, Chang W, Du C, Dowd P, et al. Expression pattern of the human FcRH/IRTA receptors in normal tissue and in B-chronic lympho cytic leukemia. Int Immunol. 2006;18:1363–73.
[7] Capone, Mollie et al. “Fc Receptor-Like Proteins in Pathophysiology of B-cell Disorder.” Journal of clinical & cellular immunology vol. 7,3 (2016): 427. doi:10.4172/2155-9899.1000427
[8] What Is FcRH5? Role in Immunity, Disease, and Treatment - Biology Insights
[9] Devasia, A.J., Chari, A. & Lancman, G. Bispecific antibodies in the treatment of multiple myeloma. Blood Cancer J. 14, 158 (2024). https://doi.org/10.1038/s41408-024-01139-y
[10] US 10,435,471 B2
[11] Stewart, A.K., Krishnan, A.Y., Singhal, S. et al. Phase I study of the anti-FcRH5 antibody-drug conjugate DFRF4539A in relapsed or refractory multiple myeloma. Blood Cancer Journal 9, 17 (2019). https://doi.org/10.1038/s41408-019-0178-8

400-614-0008
www.kactusbio.cn
support@kactusbio.com