Professor Wu Xin's Team Showcases DKutting® LL in the Treatment of Lower Extremity Atherosclerotic Occlusive Disease

DK Medtech
Vascular Interventional Balloon Product Developer

DKutting®LL continues to use DK Medtech's unique triangular nitinol coil spring patent technology, combined with the actual clinical needs of lower limb arteries. It significantly increases the length of the scoring element (up to 150mm) and develops a new fully coaxial balloon delivery system compatible with 0.014"/0.018" guidewires, enriching the selection of balloon diameters at 0.5mm intervals.
DK Medtech's unique directional scoring balloon boasts comprehensive performance with robust radial expansion and flexible axial bending. Its clinical performance has been widely recognized in both the coronary and hemodialysis access fields. The latest development is the DKutting.®LL Scoring Balloon is specifically designed for lower limb arterial intervention, demonstrating significant clinical advantages in directional dilation mechanisms and setting a new standard for peripheral vascular pre-dilation.
DK Medtech Special Release[Professor Wu Xin's Team: DKutting®Application of LL in Lower Extremity Arteriosclerosis Occlusion Disease: Case Presentation, demonstrating the fine operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized procedures and technical applications during surgery, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
DKutting® Application of LL in Lower Extremity Arteriosclerosis Obliterans
Wu Xin, Wangjing Hospital of China Academy of Chinese Medical Sciences
Patient Information
Basic Information:Male, 63 years old.
Chief Complaint:Intermittent claudication in both lower limbs for over a year.
History of Present Illness:More than a year ago, the patient developed intermittent claudication in both lower limbs without obvious cause. An ultrasound examination at the local community hospital suggested: lower limb arterial stenosis. After treatments such as acupuncture and massage, the intermittent claudication did not significantly improve. Subsequently, the patient's intermittent claudication worsened compared to before, with the claudication distance reduced to 20 meters. On October 25, 2024, an ultrasound examination at our hospital showed: atherosclerosis with plaque formation in the left lower limb artery: localized moderate stenosis of the left femoral artery; localized severe stenosis of the left popliteal artery: incomplete occlusion of the left anterior tibial artery. Atherosclerosis with plaque formation in the right lower limb artery: localized moderate stenosis of the right femoral artery and popliteal artery.); Incomplete occlusion of the right anterior tibial artery. The patient is now admitted to our department with "lower extremity atherosclerotic occlusive disease" for further treatment. Current symptoms: intermittent claudication in both lower limbs, more pronounced on the left side, with a claudication distance of 20 meters. No significant rest pain, no ulceration, no edema in both lower limbs, no dizziness or headache, no palpitations or chest tightness, no cough or sputum, no abdominal pain or diarrhea. Appetite and sleep are normal. Frequent and urgent urination, bowel movement once daily, slightly dry.
Past Medical History:Hypertension for 20 years, highest blood pressure 185/120mmHg, controlled by oral Metoprolol Succinate 47.5mg qn, with blood pressure maintained at 120/70mmHg. Diabetes for 20 years, managed by oral Saxagliptin 50mg qd, Dapagliflozin 10mg qd, and Acarbose 100mg tid; blood glucose not monitored. History of coronary heart disease for 10 years, underwent "coronary artery stent implantation" at Chaoyang Hospital 9 years ago, with a total of 3 stents implanted (details unknown), long-term oral administration of Aspirin 100mg qd and Clopidogrel Bisulfate 75mg qd for antiplatelet aggregation, and Rosuvastatin 5mg qn for lipid-lowering and plaque stabilization. History of chronic heart failure, managed by oral Furosemide 20mg bid (morning and before sleep), Spironolactone Tablets 40mg qd for diuresis, and Sacubitril Valsartan Tablets 200mg qd for cardiac function protection. Denies history of other chronic diseases such as cerebral infarction.
Physical Examination:The skin temperature of both lower limbs was relatively low, and the skin color was dark. No obvious edema was observed in both lower limbs. The femoral arteries on both sides were palpable, but the left femoral artery was weaker. The popliteal arteries, dorsalis pedis arteries, and posterior tibial arteries on both sides were not palpable.
Admission Diagnosis:
Lower Extremity Arteriosclerosis Obliterans: Occlusion of the Left Superficial Femoral Artery, Stenosis of the Right Superficial Femoral Artery, Occlusion of Both Peroneal Arteries, Occlusion of Both Anterior Tibial Arteries
Grade 3 Hypertension, Very High Risk Group
Type 2 Diabetes
Postoperative Coronary Artery Stent Implantation for Coronary Atherosclerotic Heart Disease
Chronic Heart Failure
Previous interventional treatment
Time | Main Treatment Process |
October 25, 2024 | Ultrasound examination in our hospital outpatient clinic showed: Atherosclerosis with plaque formation in the left lower limb arteries: Localized moderate stenosis of the left femoral artery; Localized severe stenosis of the left popliteal artery: Incomplete occlusion of the left anterior tibial artery. Atherosclerosis with plaque formation in the right lower limb arteries: Localized moderate stenosis of the right femoral and popliteal arteries; Incomplete occlusion of the right anterior tibial artery. It is recommended that surgical patients continue conservative treatment, with oral administration of Aspirin Tablets 100mg qd and Sarpogrelate Hydrochloride Tablets 100mg tid. |
October 27, 2024 | The patient's symptoms did not improve, and they agreed to undergo surgical treatment in the hospital. |
October 27, 2024 to November 1, 2024 | Complete preoperative examinations |
November 1, 2024 | Perform lower limb arterial angiography on the patient, balloon angioplasty of the left superficial femoral artery and calf arteries, and prepare for stent implantation in the left superficial femoral artery. |
November 6, 2024 | Angiography of Lower Limb Arteries and Balloon Angioplasty of Right Superficial Femoral Artery and Leg Arteries in the Interventional Treatment Center |
November 11, 2024 | Improved and discharged, continue antiplatelet, vasodilator, and lipid-lowering drug treatment after discharge. |
Preoperative Analysis
Preoperative Analysis:The patient has a 20-year history of hypertension and diabetes, with severe vascular disease and calcification. Ordinary balloons may not effectively dilate the blood vessels, failing to restore the effective lumen, and are prone to causing dissections. Rescue stent implantation may be required.
Surgical Objective:
Main Objectives:Opening blood vessels and restoring effective vascular lumen.
Secondary Objectives:Avoid the formation of flow-limiting layers and avoid stent implantation.
Surgical Strategy/Plan:Lower extremity arteriography, balloon angioplasty of the left superficial femoral artery and calf arteries, with preparation for stent implantation in the left superficial femoral artery.
Surgical Description:
A 6F femoral artery sheath was inserted through antegrade puncture of the left femoral artery.
5F Cordis VER135° catheter combined with Comand 18 guidewire for true lumen recanalization of the diseased vessel.
DK Medtech 5.0*150mm DKutting®LL Peripheral Scoring BalloonDilate the diseased vessel segment.
Drug-coated balloon applied to the vascular lesion segment.
Vascular suture closure device sutures the puncture site.
Surgical Procedure
Preoperative baseline angiography confirmed occlusion of the superficial femoral artery and anterior tibial artery.
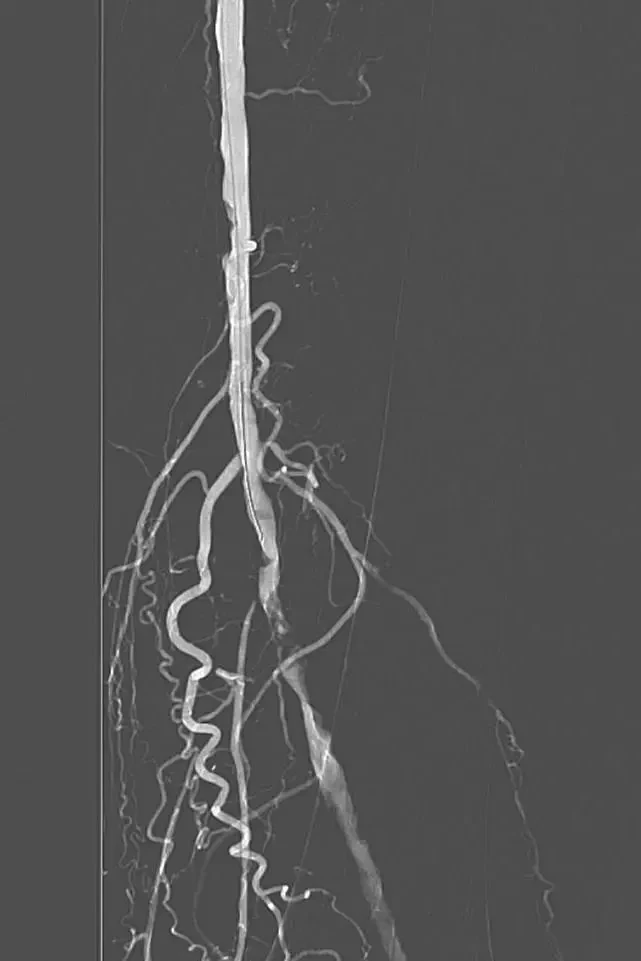
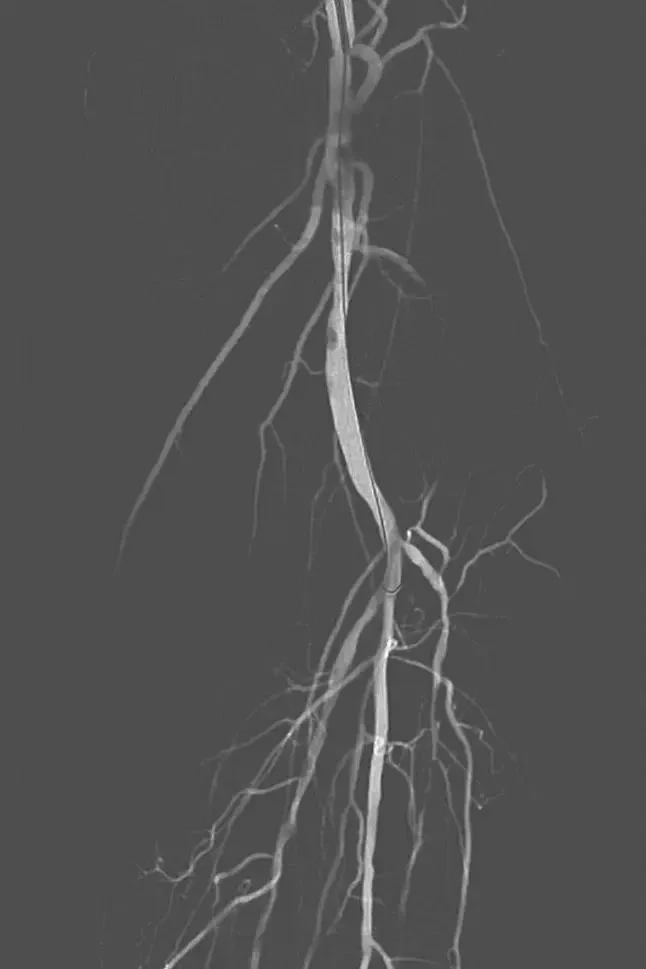
The road map guidewire opens the blood vessel to reach the popliteal artery.

DK Medtech 5.0*150mm DKutting®LL Peripheral Scoring BalloonDilate the superficial femoral artery, and blood flow was restored after dilation.


Post-dilation of the superficial femoral artery with a 5*150mm drug-coated balloon, followed by angiography after dilation of the peroneal artery with a 2.5*220mm drug-coated balloon.
Follow-up
Discharge Status:
The patient's symptoms of intermittent claudication in the left lower limb disappeared, and the skin temperature of the lower limb was good.
Continue oral administration of aspirin, sarpogrelate hydrochloride tablets, and atorvastatin calcium tablets after discharge.
Follow-up after 2 weeks: No intermittent claudication in both lower limbs, no numbness or cold discomfort in the limbs.
Case Summary
Case Characteristics:The patient has had hypertension and diabetes for over 20 years, with severe arterial sclerosis and calcification.
Preoperative Assessment Key Points:Lower Extremity Arterial Color Doppler Ultrasound, CTA Evaluation of Lesion Calcification Severity.
Surgical Strategy/Technical Key Points:Try to open the true lumen, slowly expand the balloon, and avoid the formation of flow-limiting dissections.
Characteristics/Usage Tips of the Device:The pressure increases slowly, pausing for 10 seconds with each increase of 1 atmosphere.

Introduction of Experts


Professor Wu Xin
The Surgeon of This Case
Director of the Department of Vascular Surgery, Wangjing Hospital, China Academy of Chinese Medical Sciences, Chief Physician, Ph.D., Professor, Master's Supervisor.
Young Member of the Vascular Surgery Branch of the Beijing Medical Association;Youth Committee Member of the Peripheral Vascular Disease Professional Committee of the Chinese Society for Microcirculation;Member of the Expert Committee on Geriatric Vascular Diseases of the Peripheral Vascular Disease Professional Committee of the Chinese Society of Integrated Traditional and Western Medicine;Member of the Vasculitis Expert Committee of the Peripheral Vascular Disease Professional Committee of the Chinese Association of Integrative Medicine;Member of the Vascular Surgery Professional Committee of the China Medical Education Association;Member of the Peripheral Vascular Disease Professional Committee of the Beijing Association of Integrated Traditional Chinese and Western Medicine;Member of the Peripheral Vascular Disease Professional Committee of the Chinese Association of Integrative Medicine;Committee Member of the Endovascular Treatment of Lower Extremity Veins Professional Committee, Peripheral Vascular Disease Committee, Chinese Society of Microcirculation;Member of the Diabetic Foot Professional Committee of the Beijing Association of Integrated Traditional Chinese and Western Medicine;Standing Committee Member and Deputy Secretary General of the Diabetic Foot Professional Committee of the Beijing Association of Integrated Traditional Chinese and Western Medicine;Member of the Venous, Hemodialysis Access, and Vascular Malformation Group of the Fourth Committee of the Vascular Surgery Branch of Beijing Medical Association;Council Member of the Vascular Surgery Specialty Physicians Branch of the Beijing Medical Association.

Department Introduction

The Department of Vascular Surgery at Wangjing Hospital of China Academy of Chinese Medical Sciences was established on December 16, 2014. Our department has introduced top domestic experts from the Vascular Surgery Department of Xuanwu Hospital, Capital Medical University, forming a highly skilled medical team with rich clinical experience. Adhering to the treatment concept that combines traditional Chinese and Western medicine, and utilizing advanced diagnostic technologies such as spiral CT angiography (CTA), magnetic resonance angiography (MRA), and digital subtraction angiography (DSA), we treat patients with peripheral vascular diseases through integrated methods including medication, minimally invasive interventional therapy, and surgical treatments, reaching an advanced level in China. We have currently introduced various state-of-the-art debulking technologies that can provide one-stop solutions for patients with arterial and venous thrombotic diseases. Combining VSD negative pressure wound therapy and the integrated treatment concept of traditional Chinese and Western medicine, we can promote the healing of ulcers and wounds. Venous thrombus aspiration can effectively prevent post-thrombotic syndrome. Our department now mostly adopts advanced endovascular debulking techniques such as drug-coated balloons and plaque excision for peripheral vascular surgeries, which can greatly reduce stent implantation and ensure long-term vascular patency.
Mainly engaged in peripheral arterial and venous vascular diseases, including: 1. Thoracic and abdominal aortic dissection and aneurysmal dilation, 2. Lower limb ischemia caused by various reasons, diabetic foot, carotid artery, vertebral artery, subclavian artery stenosis or occlusive diseases, 3. Renal artery stenosis-induced hypertension, renal artery stenosis-induced renal insufficiency, 4. Deep vein thrombosis of the lower extremities, varicose veins of the lower extremities, leg swelling caused by iliac vein stenosis, 5. Establishment and maintenance of dialysis access for patients with renal failure.
