Professor Shi Xiaoming's Team: Application of DKutting® LL in Long Lesion Occlusion of the Superficial Femoral Artery

DK Medtech
Vascular Interventional Balloon Product Developer
DKutting®LL continues to use DK Medtech's unique patented triangular nitinol winding technology, combined with the actual clinical needs of lower limb arteries. It significantly increases the length of the scoring element (up to 150mm) and develops a brand-new fully coaxial balloon delivery system compatible with 0.014"/0.018" guidewires, enriching the selection of balloon diameters at 0.5mm intervals.
DK Medtech's exclusive directional scoring balloon boasts comprehensive performance with robust radial expansion and flexible axial bending. Its clinical performance has been widely recognized in both the coronary and hemodialysis access fields. The latest development, DKutting...®LL Scoring Balloon is specifically designed for lower limb arterial intervention, demonstrating significant clinical advantages in directional expansion mechanisms, and setting a new standard for peripheral vascular pre-dilation.
DK Medtech Special Release[Professor Shi Xiaoming's Team: DKutting®Application of LL in Long Segment Occlusion of the Superficial Femoral Artery: Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
DKutting®Application of LL in Long Segment Occlusion Lesions of the Superficial Femoral Artery
Shi Xiaoming, Ding Dianzhu, Hebei Provincial People's Hospital
Patient Information
Basic Information:Male, 81 years old.
Chief Complaint:Left foot ulceration for 14 days.
History of Present Illness:The patient developed skin ulceration on the left foot 14 days ago after "soaking feet in hot water," with ulcerations occurring on the dorsum of the foot and the tips of the toes. After self-applying topical treatments such as povidone-iodine and erythromycin ointment, the condition did not improve. The patient subsequently developed a fever along with purulent discharge from the foot. Seeking treatment, the patient visited our hospital and was admitted to the outpatient department with a diagnosis of "type 2 diabetic foot."
Past Medical History:History of hypertension for over 7 years, with the highest blood pressure recorded at 170/90 mmHg. Currently not taking any antihypertensive medication; blood pressure control status is unknown. History of coronary heart disease for over 8 years, including a previous acute myocardial infarction treated with coronary artery stent implantation at our hospital. Atrial fibrillation for 2 years and a history of cerebral hemorrhage for 8 months.
Physical Examination:No edema in both lower limbs, swelling in the left foot with black-purple skin. Skin ulceration is observed between the toes, on the sole, and on the outer side of the left foot, accompanied by purulent discharge and a foul odor. The temperature of the left foot skin is low. Dorsalis pedis artery and posterior tibial artery pulses are not palpable on either side.
Admission Diagnosis:
Diabetic Foot (CLTI, W3I3Fi3);
Type 2 Diabetes;
Coronary Atherosclerotic Heart Disease After Coronary Stent Implantation;
Old myocardial infarction;
Atrial Fibrillation;
Hypertension Grade 2.
Preoperative Analysis
Preoperative Analysis:The patient is an elderly male with a CLTI case. According to the WIFi classification, the amputation risk is high. The ulcer areas are designed on the lateral dorsum of the foot and multiple toes. The surgery needs to open as many infrapopliteal arteries as possible or ensure the opening of the plantar arch.
Surgical Objective:
Main Objectives:Open the superficial femoral artery and infrapopliteal artery to ensure blood flow directly reaches the wound;
Secondary Objectives:Avoid flow-limiting dissection in the superficial femoral artery and reduce the chance of stent implantation. For infrapopliteal arteries, aim for 1 and strive for 2.
Surgical Strategy/Plan:
Antegrade puncture of the left common femoral artery, antegrade opening of the left superficial femoral artery, preparationPoplitealRetrograde arterial access, balloon angioplasty + drug-coated balloon dilation of the superficial femoral artery, with stent implantation as a backup.
Angiography of the arteries below the knee to clarify their condition, proceeding from easy to difficult, and opening as many arteries below the knee as possible;
Preoperative ultrasound examination of the dorsal pedis artery and posterior tibial artery lumen condition, preparation for retrograde puncture of the dorsal pedis artery and posterior tibial artery.
Surgical Description:
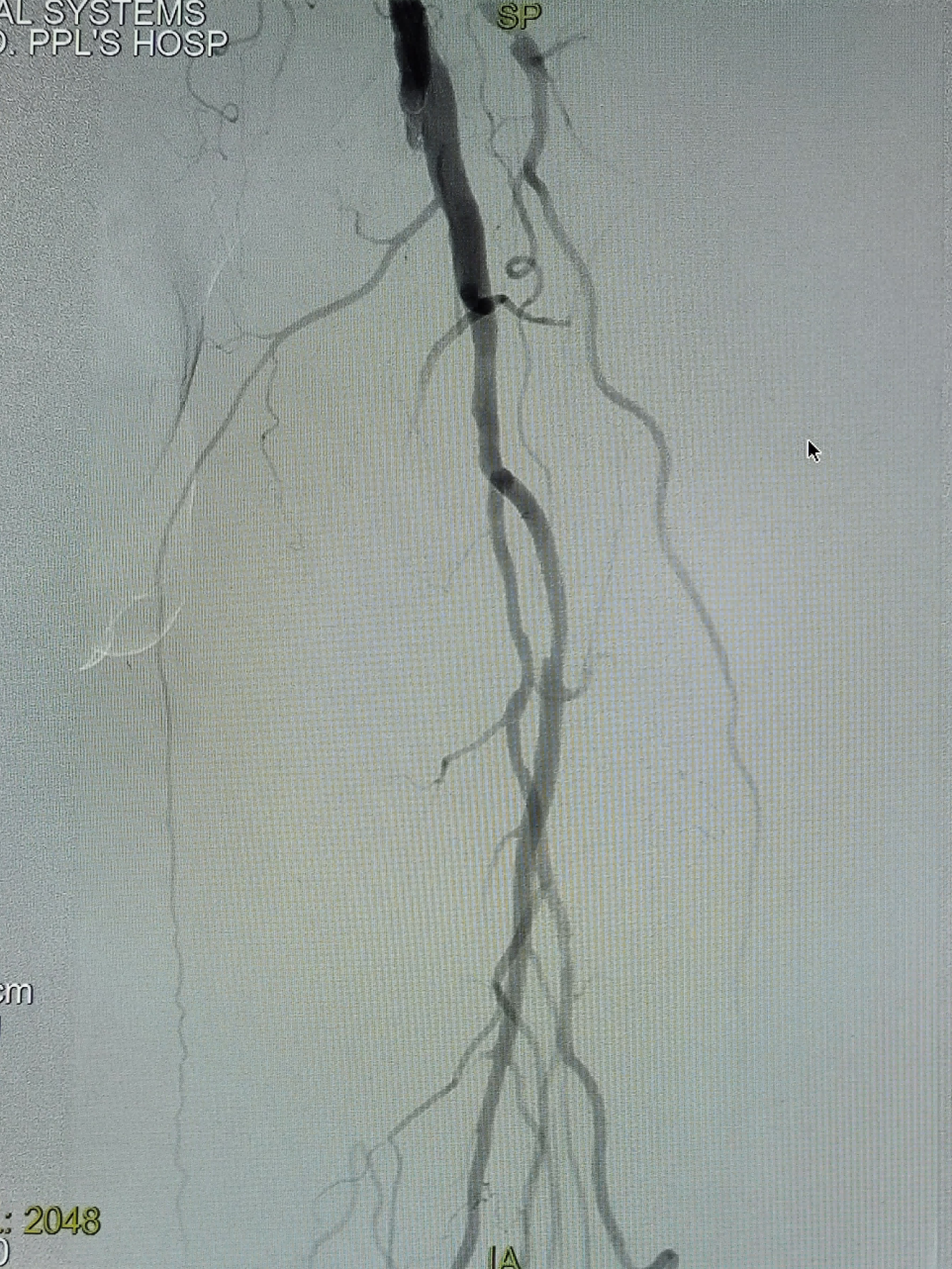
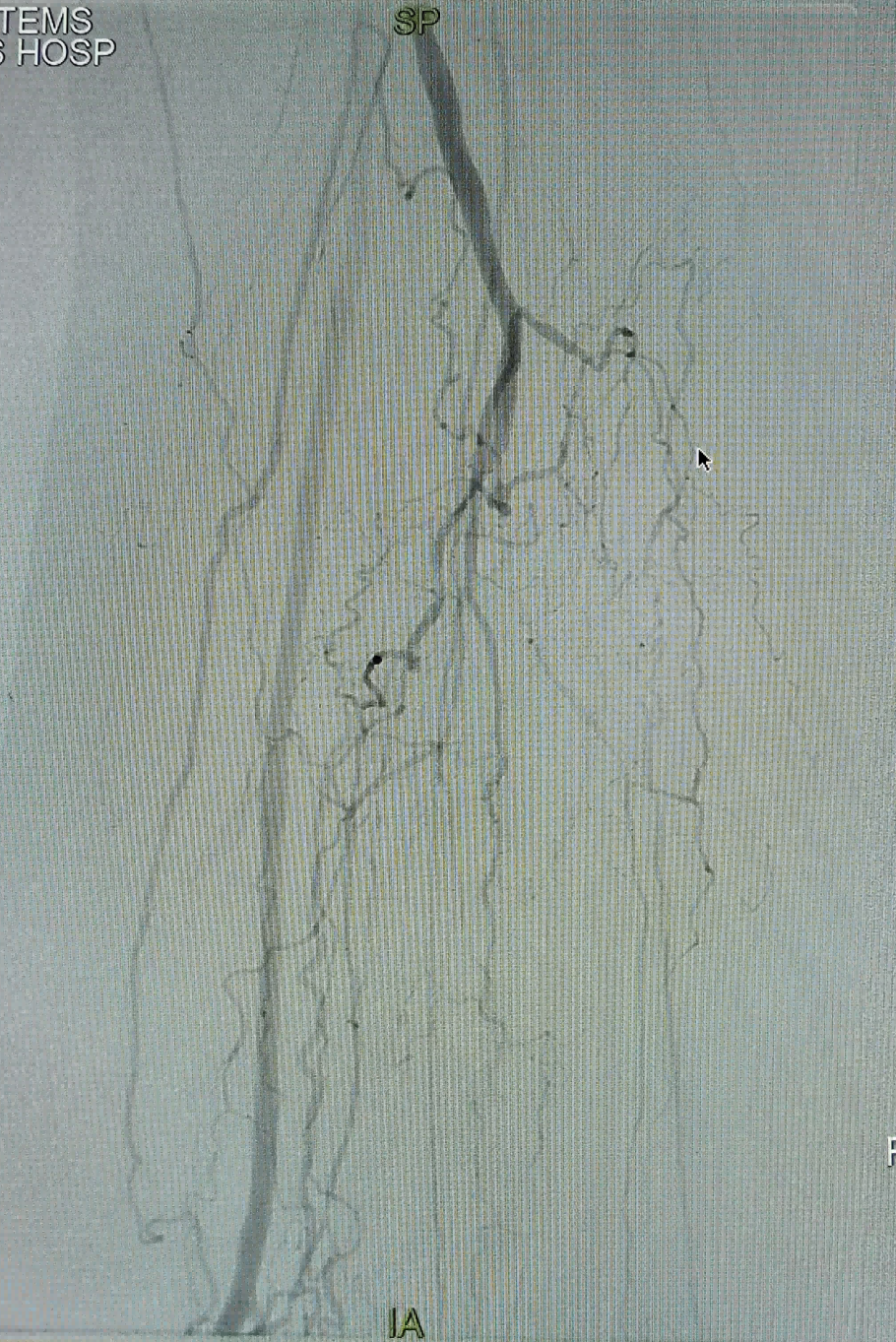
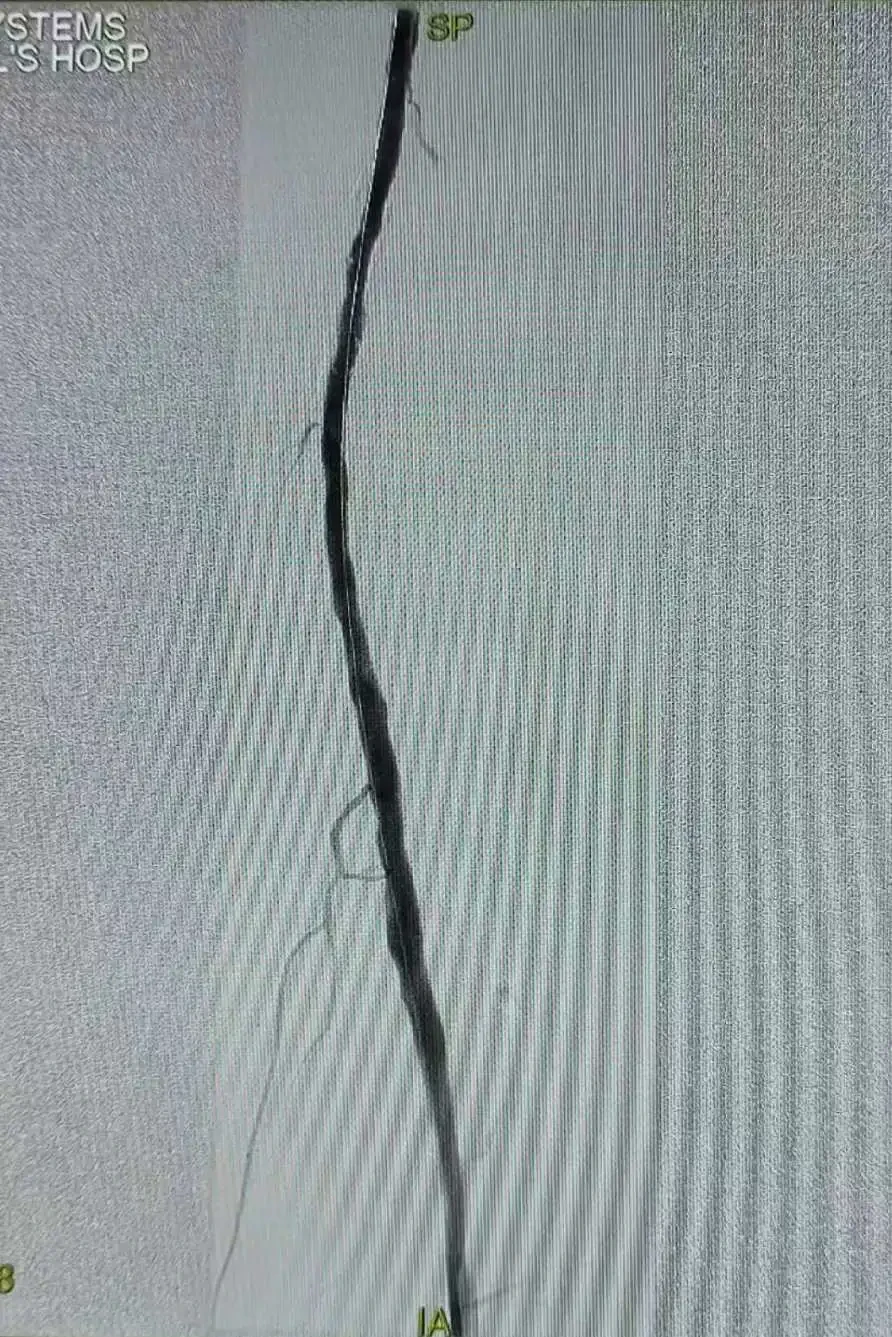
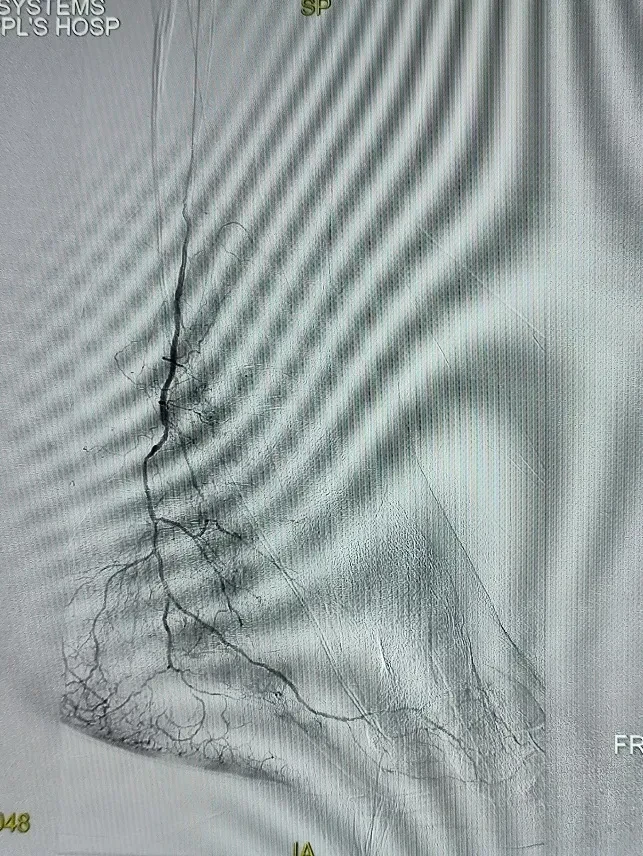
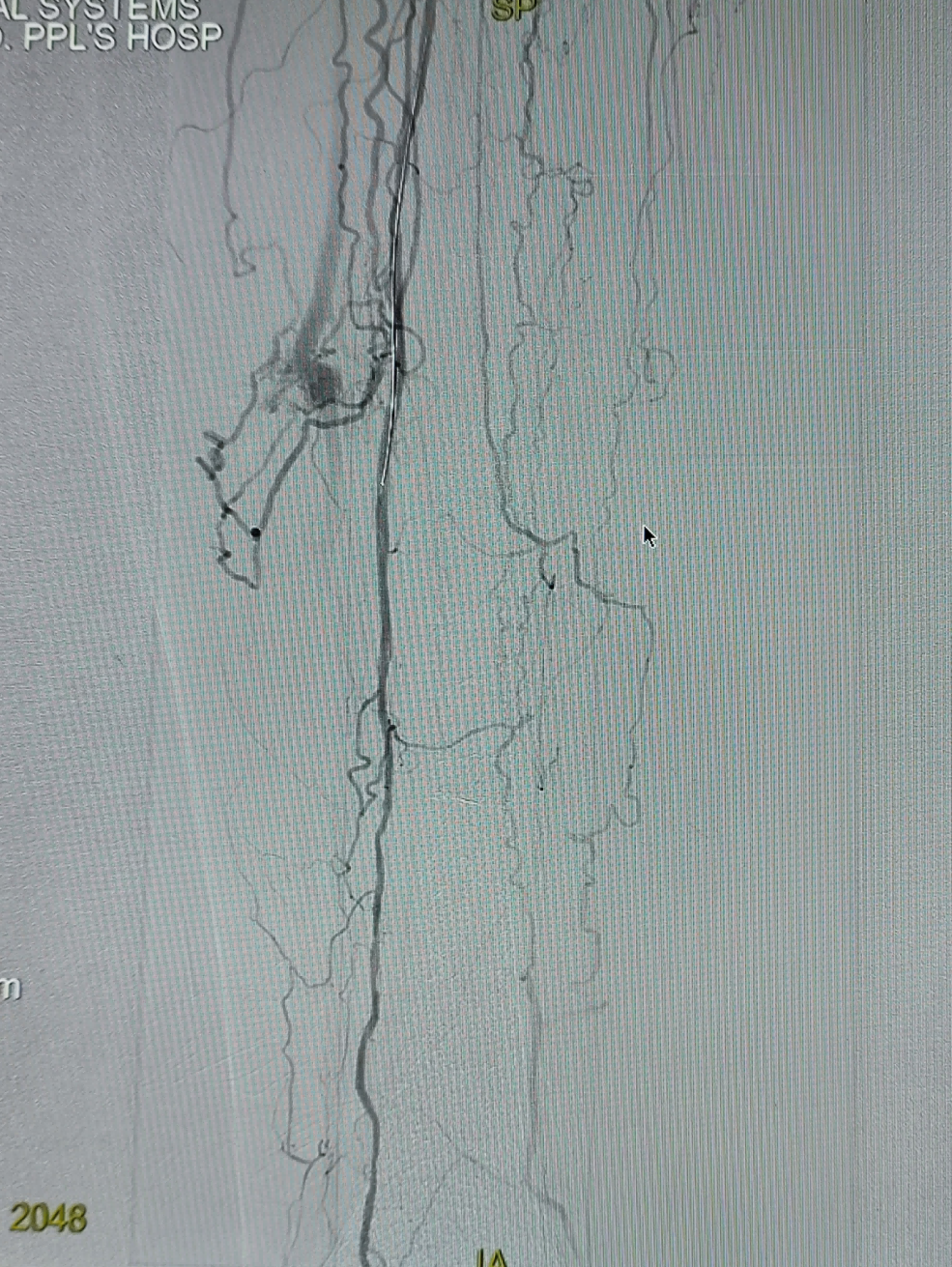
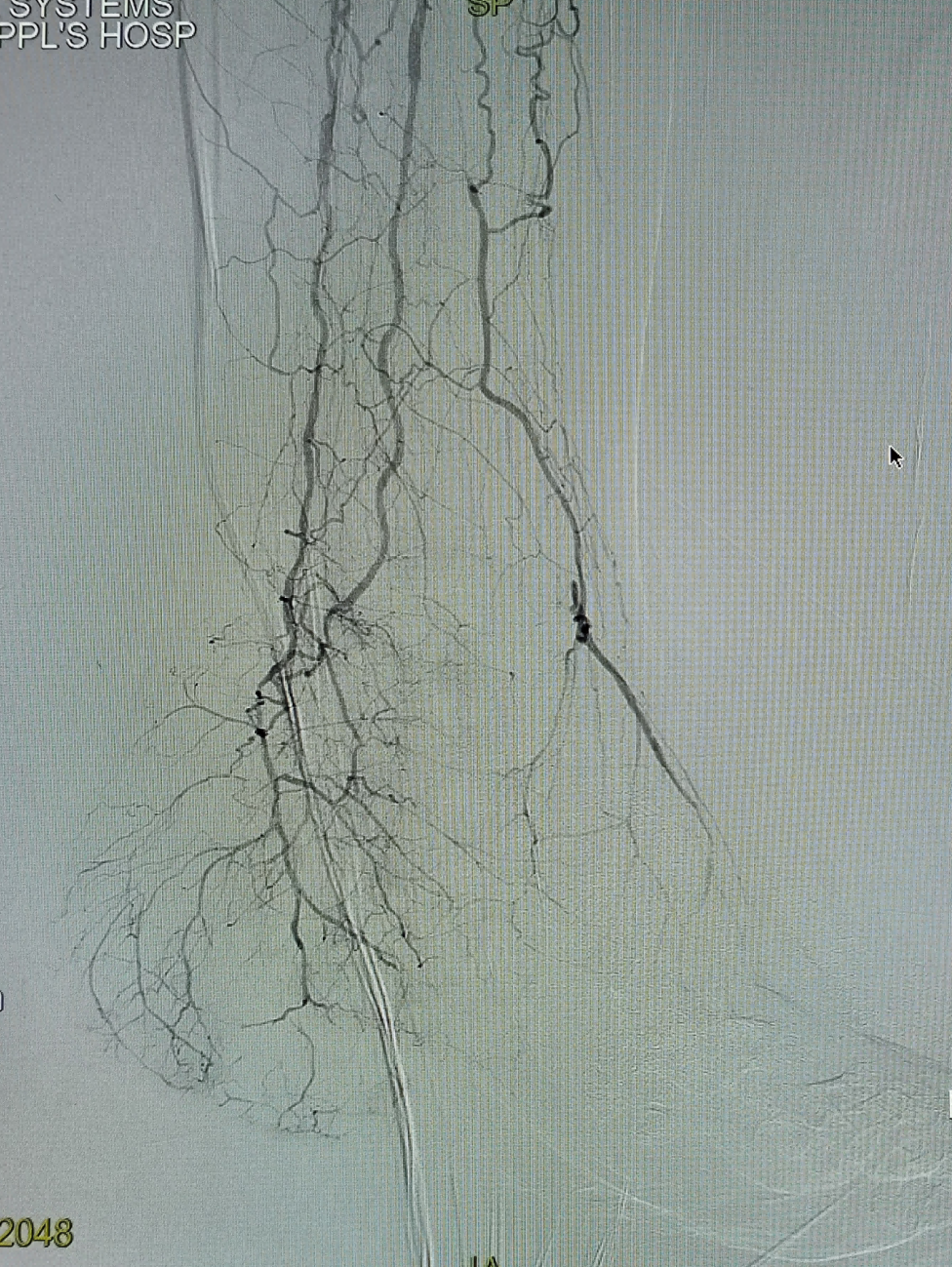
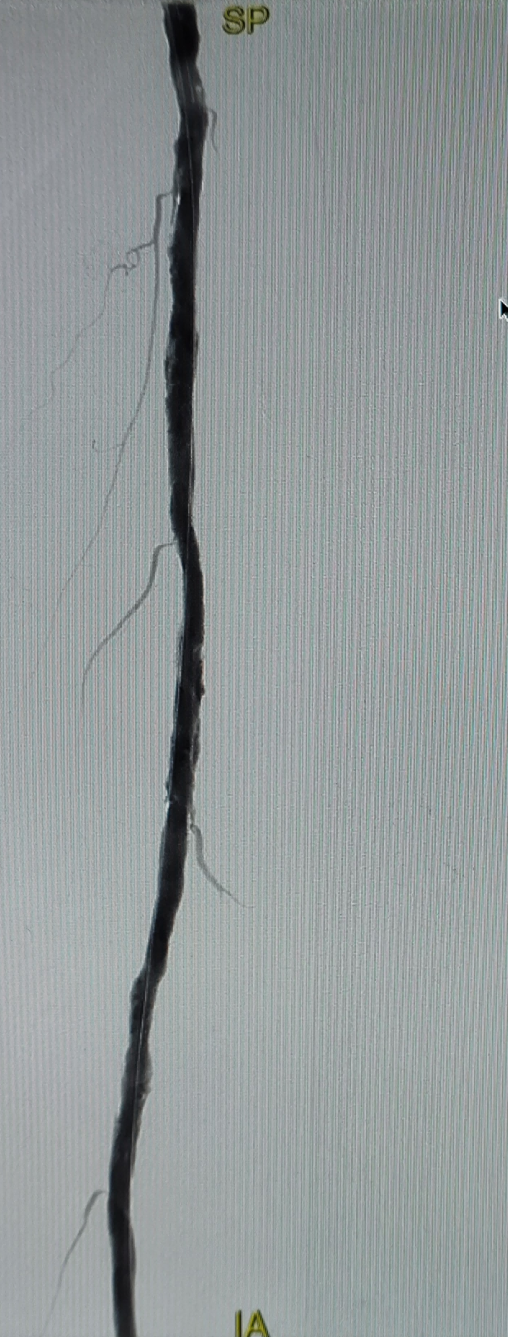
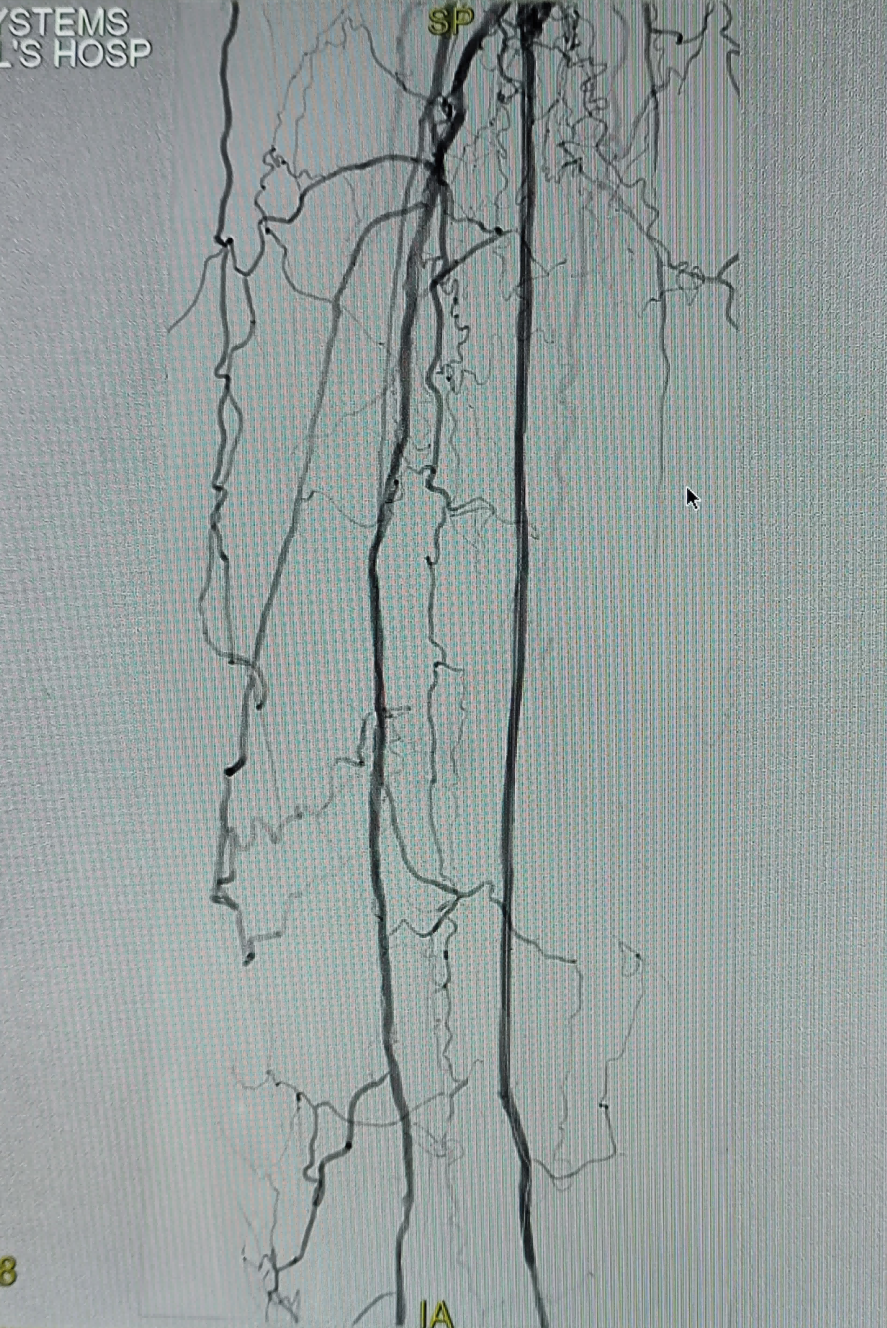
Successful antegrade puncture of the left common femoral artery under ultrasound guidance, followed by angiography of the left lower limb arteries: The lumens of the left common femoral artery and deep femoral artery are patent. The proximal approximately 1.5 cm lumen of the superficial femoral artery is patent, while there is a long segment occlusion in the middle part of the superficial femoral artery. The proximal superficial femoral artery in the adductor canal is visualized via collateral circulation.PoplitealNo abnormality in arterial blood flow, anterior tibial artery, posterior tibial artery, and peroneal artery occlusion, middle calfFarSegment 1 tortuous collateral forms an arteriovenous fistula with the posterior tibial vein, causing blood steal.FarThe distal tibial posterior artery and peroneal artery show faint opacification.
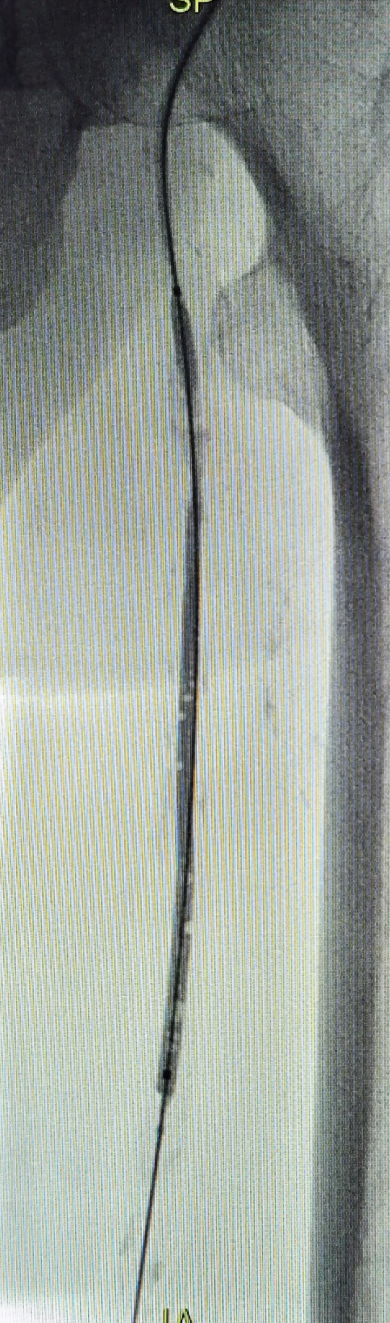
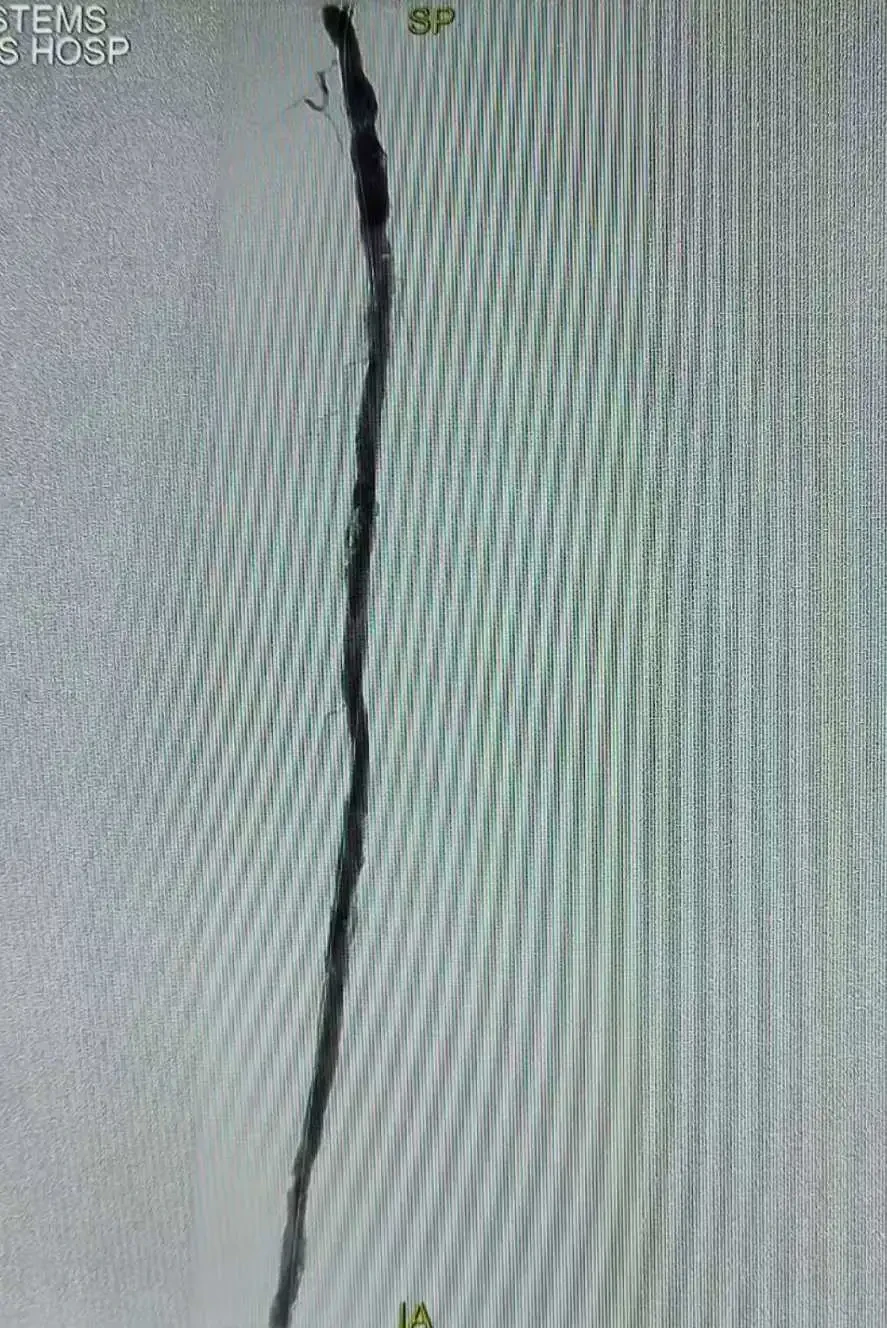
A single-bend catheter, 150 mudskipper guidewire, and Command 18 guidewire were used in coordination to successfully pass through the occluded segment of the superficial femoral artery in an antegrade manner. After angiography confirmed placement within the true lumen, a Boston Scientific Sterling 3mm balloon was used for pre-dilation of the superficial femoral artery lesion segment. Post-dilation angiography showed restored blood flow in the superficial femoral artery, achieving successful recanalization.FarEnd Lesion.
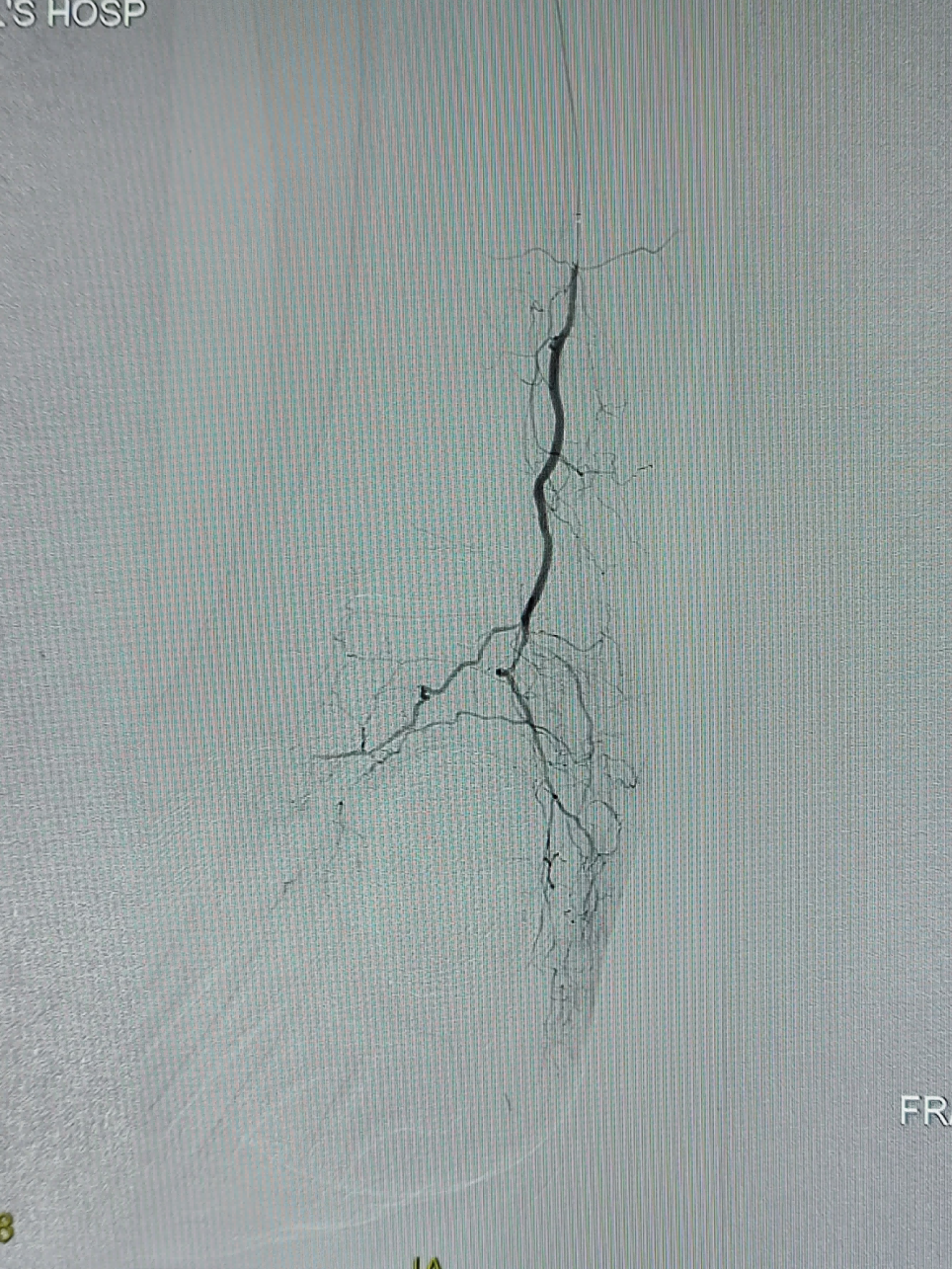
Single-bend catheter, support catheter, Gladius guidewire, and Command 18 guidewire were alternately used to antegradely open the posterior tibial artery. After angiography confirmed the true lumen, the posterior tibial artery was dilated with 2.0mm, 2.5mm, and 3mm balloons sequentially. Angiography after dilation showed restored blood flow.
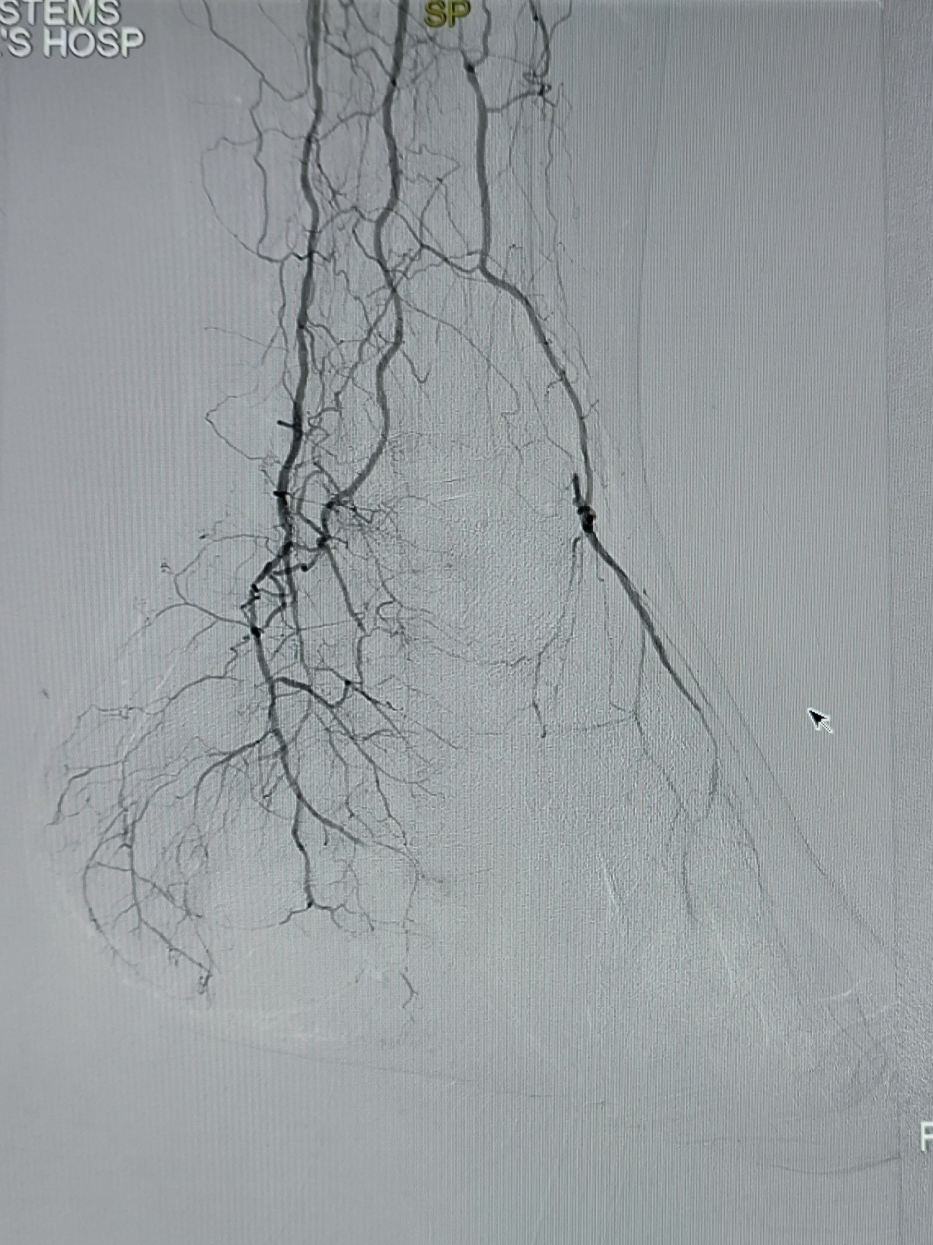
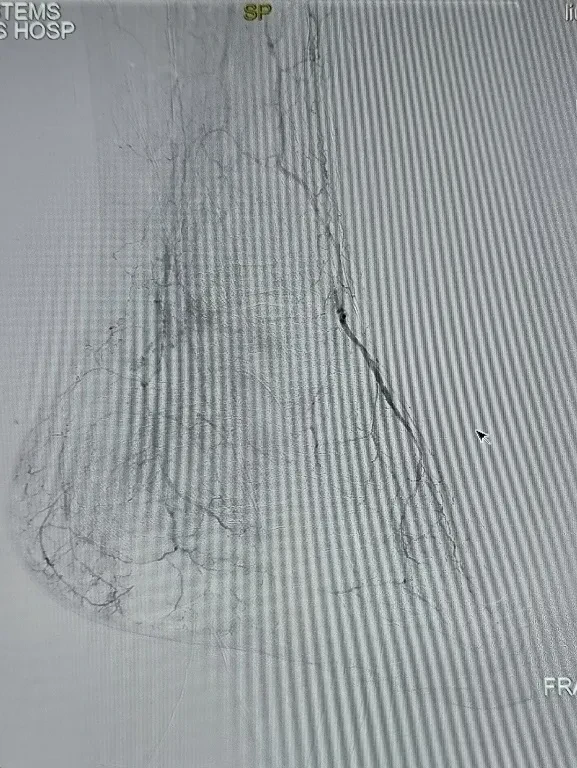
The catheter and guidewire were used again to antegradely recanalize the occluded segment of the peroneal artery, reaching the perforating branch artery at the foot and ankle. Angiography showed that the blood flow in the posterior perforating branch artery was smooth. Subsequently, balloon angioplasty of the peroneal artery was completed using 2.0mm and 2.5mm balloons. After dilation, another angiography revealed that the blood flow in both the posterior tibial artery and the peroneal artery had been restored smoothly. The medial and lateral plantar arteries could be quickly and directly visualized, while the dorsal pedal artery was slightly delayed in visualization through collateral circulation. The treatment of the infrapopliteal arteries was completed.
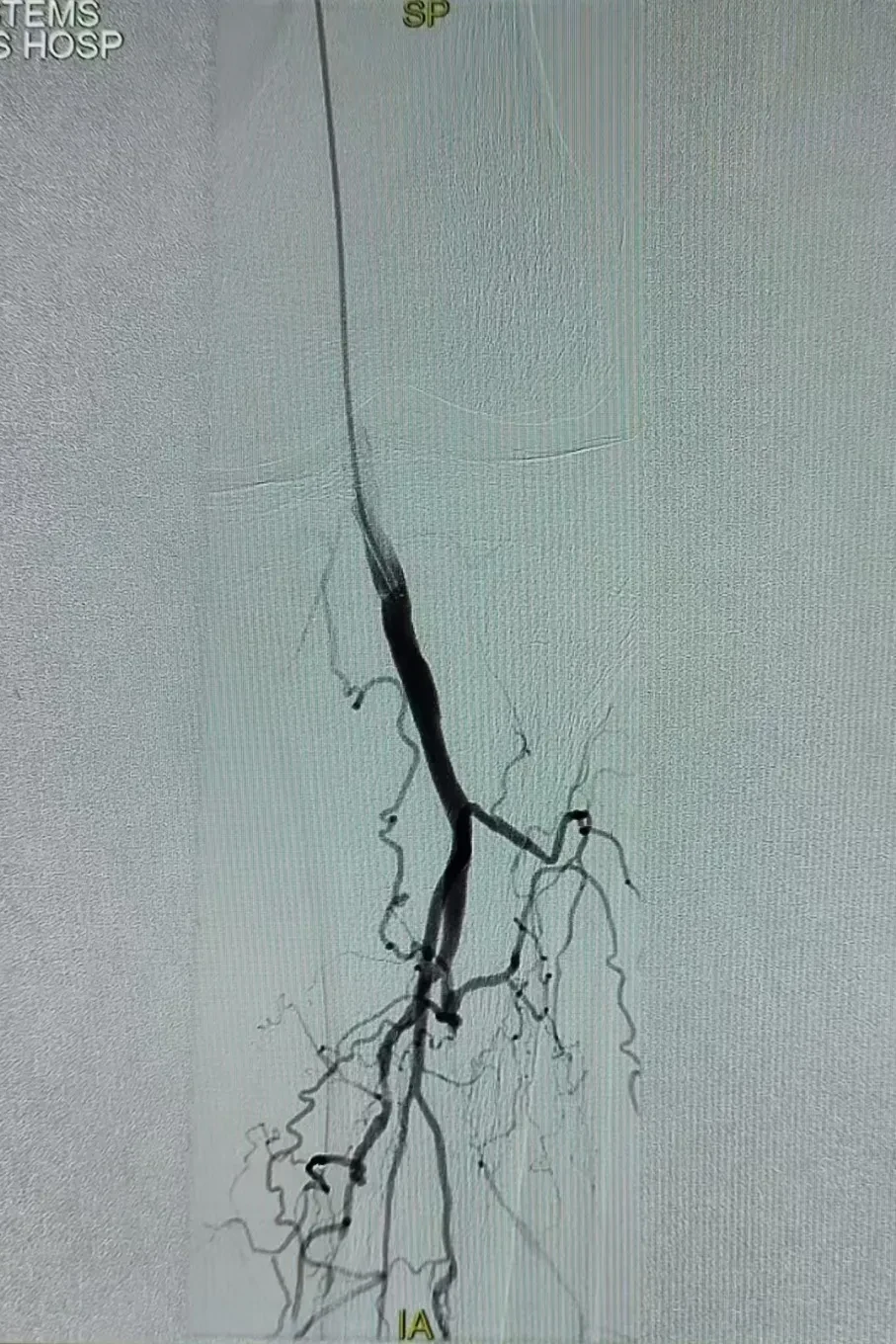
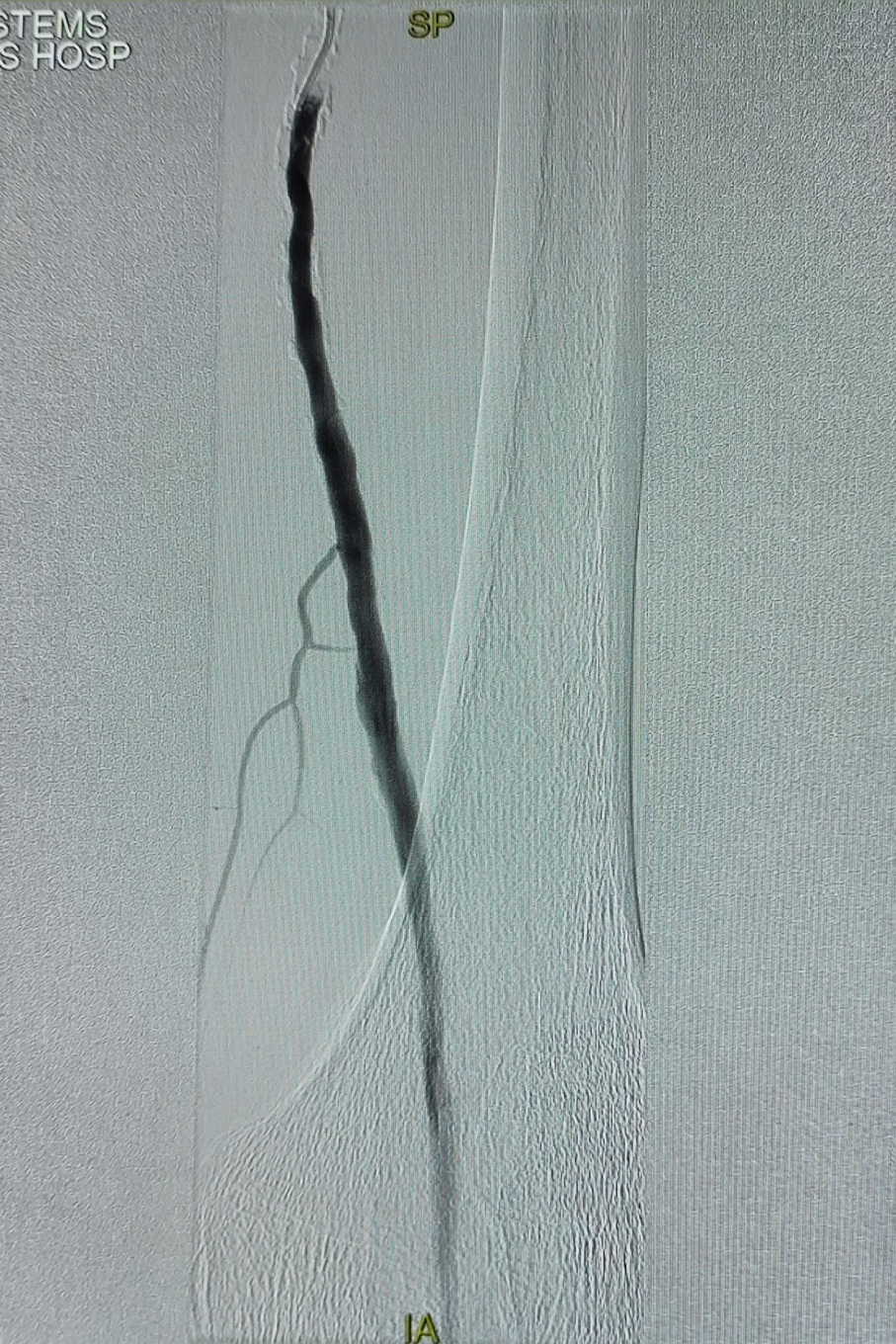
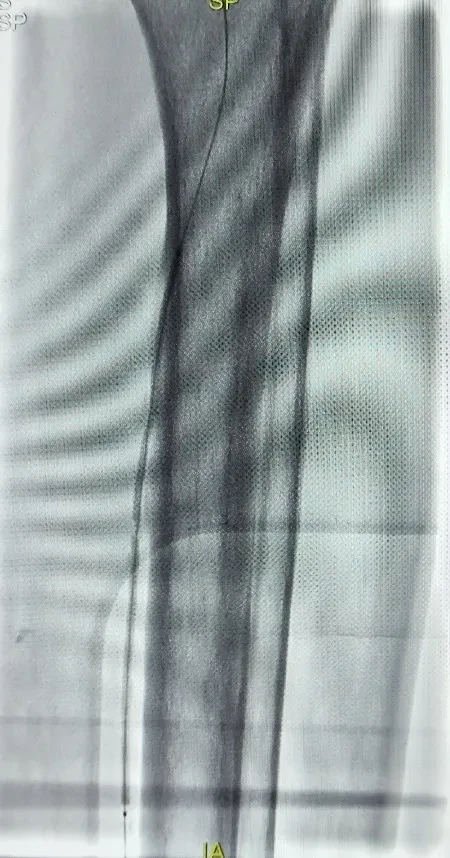
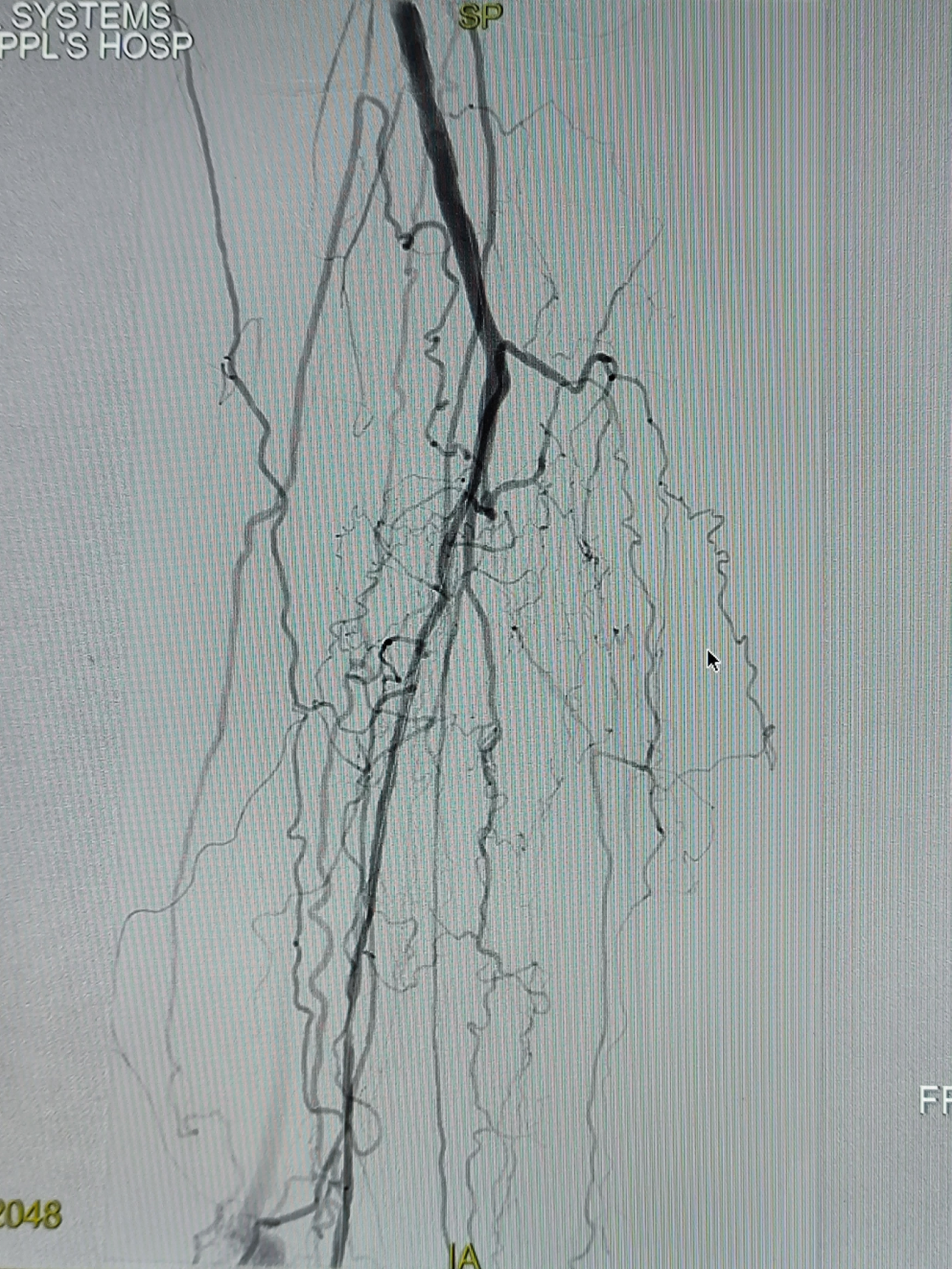
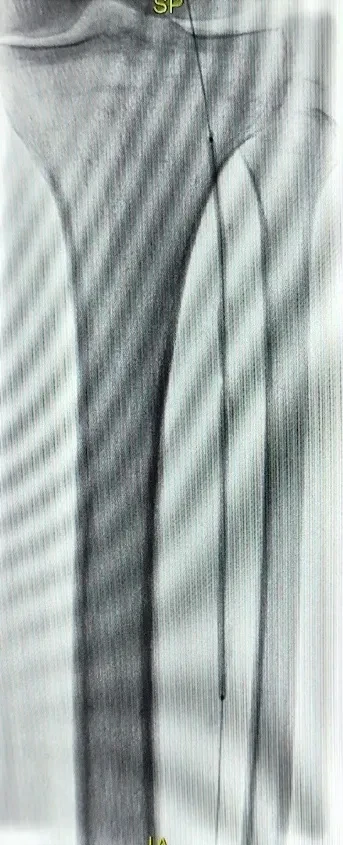
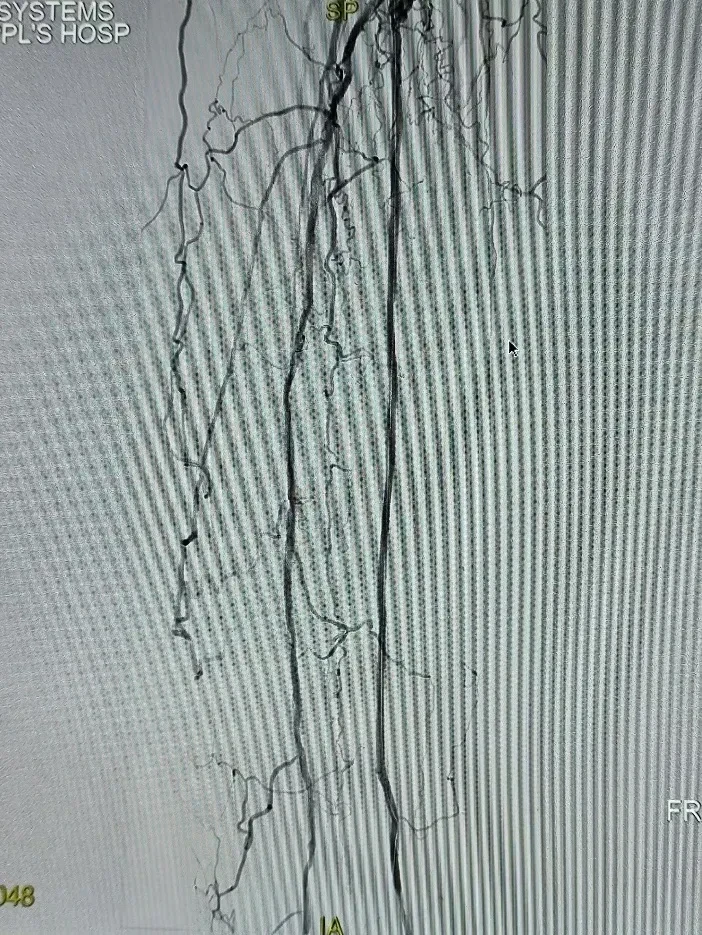
To reduce the risk of superficial femoral artery dissection and lower the stent implantation rate, useDKutting®LL 5*150mm Peripheral Scoring BalloonCompleted balloon angioplasty of the superficial femoral artery. Post-dilation angiography showed good blood flow in the superficial femoral artery without significant flow-limiting dissection. Subsequently, drug-coated balloons of 5mm*150mm and 5mm*80mm were used respectively for balloon dilation of the lesion segment of the superficial femoral artery. After dilation, angiography was performed again, showing smooth blood flow in the superficial femoral artery without flow-limiting dissection.FarNo obvious embolic events were observed at the distal end, and the arteriovenous fistula in the calf was still visible, with a significantly reduced shunt flow compared to before.
Surgical Procedure
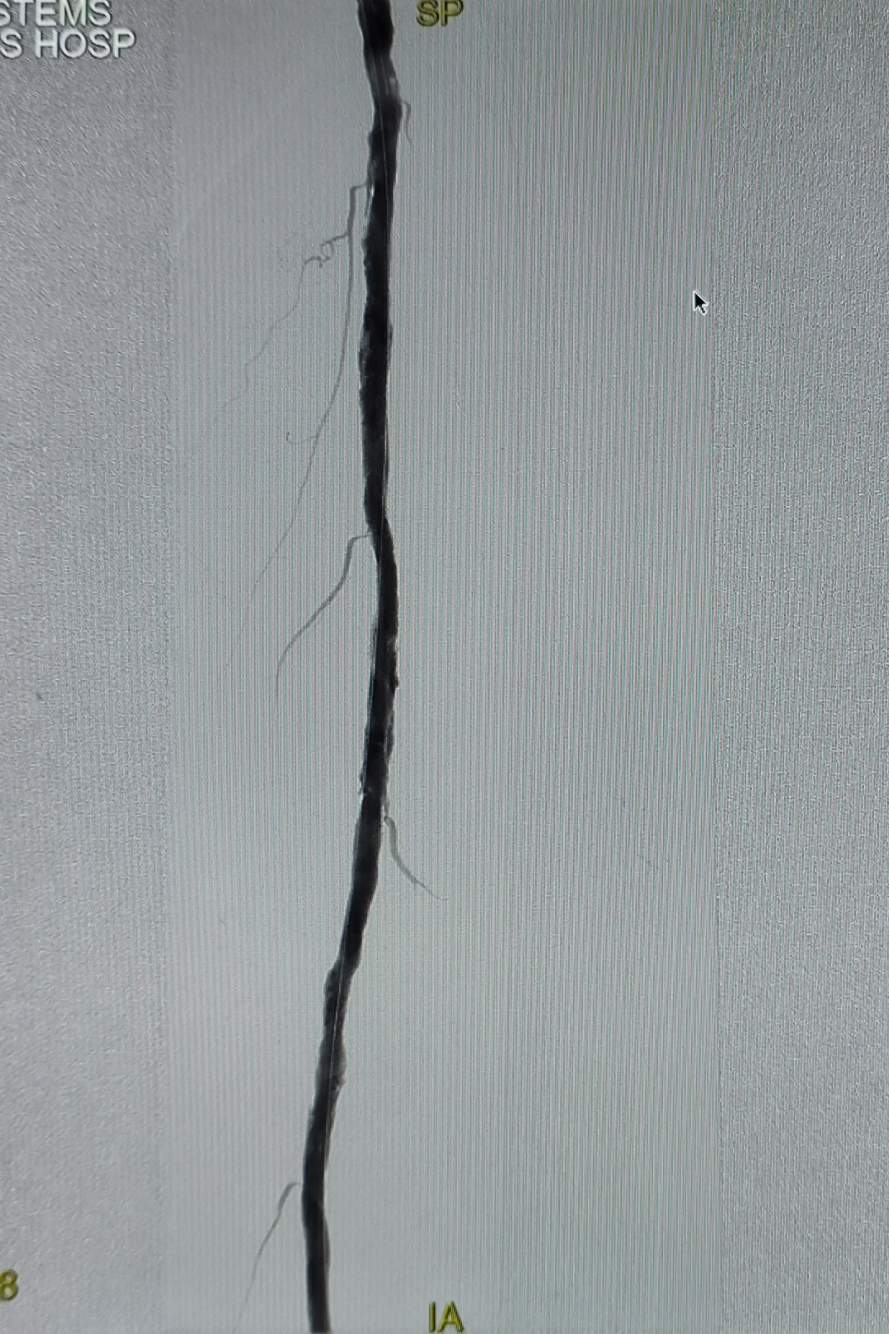
The superficial femoral artery is occluded from 1.5 cm above its origin to 5 cm below the adductor canal.
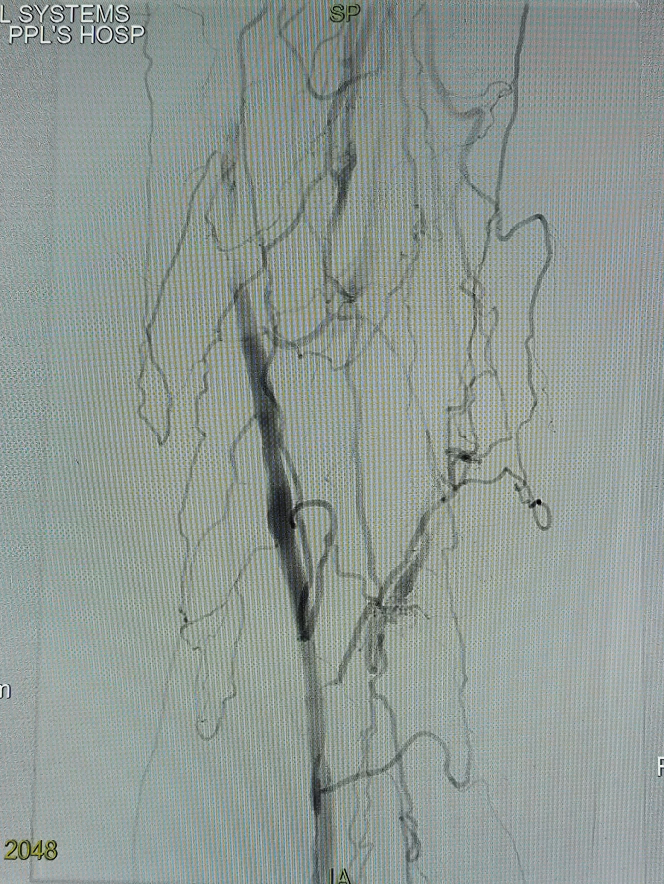
Anterior Tibial Artery, Posterior Tibial Artery, and Peroneal Artery Occlusion, Middle CalfFarSegment 1 tortuous collateral forms an arteriovenous fistula with the posterior tibial vein, causing blood steal.FarThe posterior tibial artery and peroneal artery show faint opacification.
The occluded segment of the superficial femoral artery was passed antegradely, and after angiography confirmed the true lumen, pre-dilation was performed using a 3mm balloon.
After pre-dilation angiography, the blood flow of the superficial femoral artery was restored.
The posterior tibial artery was antegradely opened, and angiography confirmed the true lumen. The posterior tibial artery was then dilated with 2.0mm, 2.5mm, and 3mm balloons respectively.
Contrast flow restored after dilation.
The antegrade recanalization of the peroneal artery occlusion segment reached the posterior perforating artery at the ankle. Angiography showed that the blood flow of the posterior perforating artery was smooth. Then, a 2.0mm and 2.5mm balloon was used to complete the peroneal artery balloon dilation.
After dilation, angiography was performed again, showing restored blood flow in both the posterior tibial artery and peroneal artery.
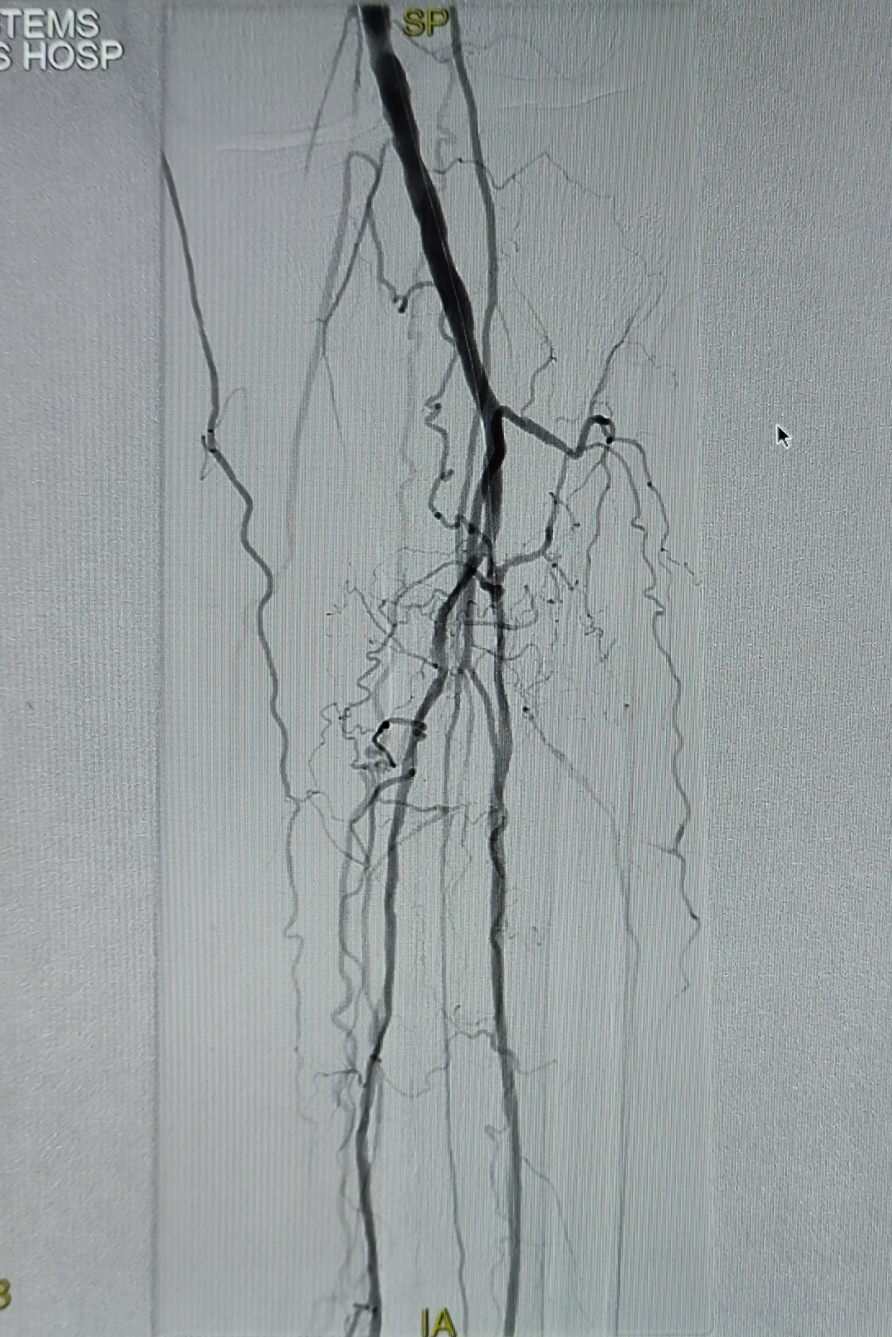
UseDKutting®LL 5*150mm Peripheral Scoring BalloonAfter completing the balloon angioplasty of the superficial femoral artery, a post-expansion angiogram showed no flow-limiting dissection. Subsequently, two drug-coated balloons, sized 5mm*150mm and 5mm*80mm respectively, were used to perform further balloon dilations on the lesion segment of the superficial femoral artery.

Final angiography shows patent blood flow in the superficial femoral artery, without flow-limiting dissection.FarNo obvious embolic events were observed at the distal end, and the posterior tibial artery, peroneal artery, plantar artery, and dorsal pedis artery were all visible.
Case Summary
Case Characteristics:Long-segment occlusion of the superficial femoral artery, multi-vessel and multi-segment occlusion of the infrapopliteal arteries, elderly patient, severe condition, complex surgery with high difficulty. History of cerebral hemorrhage, long-term dual antiplatelet or dual pathway antithrombotic therapy post-surgery, with a high risk of recurrent cerebral hemorrhage. For long-segment occlusive lesions of the superficial femoral artery, it is crucial to avoid stent implantation as much as possible and reduce the antithrombotic time window. The length of the superficial femoral artery lesion is approximately 200mm.DKutting®LL Peripheral Scoring BalloonAfter treatment, no significant flow-limiting dissection was observed.DKutting®LL Peripheral Scoring BalloonThe effect of lumen preparation was very satisfactory.
Surgical Strategy/Technical Key Points:Try to open the true lumen, slowly expand the balloon, and avoid the formation of flow-limiting dissections.
Device Features/Usage Tips:The balloon reaches the lesion site, first inflating to 3atm and maintaining for at least 30 seconds to ensure minimal shear force during balloon expansion. Then, the balloon is expanded to the nominal pressure of 8atm/10atm and maintained for at least 120 seconds.

Expert Introduction


Professor Shi Xiaoming
Director of Vascular Surgery
Director of the Vascular Surgery Department, Hebei Provincial People's Hospital;候任主任委员 of Hebei Branch, China Division, International Vascular Alliance;Standing Committee Member of the Diabetic Foot Branch of the China International Exchange and Promotive Association for Medical and Health Care;Member of the Vascular Surgery Branch of the Chinese Medical Doctor Association;Member of the Expert Committee on Pan-Vascular Medicine;候任主任委员 of the Vascular Surgery Branch of the Hebei Medical Association;Vice Chairman of the Vascular Surgery Branch of the Hebei Provincial Medical Association;Vice Chairman of the Endovascular Specialty Physicians Branch of the Hebei Province Medical Association;Vice Chairman of the Varicose Veins Professional Committee of Hebei Vascular Health and Technology Association;Vice Chairman of the Peripheral Vascular Disease Professional Committee of the Hebei Integrated Traditional and Western Medicine Association;Vice Chairman of the Vascular Surgery Branch of Shijiazhuang Medical Association.
Skilled in the treatment of various vascular diseases such as thoracic and abdominal aortic aneurysms, vascular occlusive diseases, Budd-Chiari syndrome, and vasculitis, etc. Experienced in the treatment of benign and malignant tumors in the abdomen, gastrointestinal tract, neck, combined organ resection, and critical care in general surgery. Holds key positions including Chairman of the Vascular Surgery Branch of the Hebei Preventive Medicine Association, President-elect of the Hebei Branch of the International Union of Angiology (China Section), Standing Committee Member of the Diabetic Foot Branch of the China International Exchange and Promotive Association for Medical and Healthcare, Vice Chairman of the Vascular Surgery Branch of the Hebei Medical Doctor Association, Standing Committee Member and Leader of the Thrombosis Prevention and Treatment Group of the Vascular Surgery Branch of the Hebei Medical Association, Vice Chairman of the Varicose Veins Professional Committee of the Hebei Vascular Health and Technology Association, and Vice Chairman of the Peripheral Vascular Disease Professional Committee of the Hebei Integrative Traditional and Western Medicine Society. As the principal investigator, has led 9 research projects, published 91 papers including 10 SCI papers, co-authored 6 books, and received multiple scientific and technological progress awards.
Professor Ding Dianzhu
Surgeon of This Case
Vascular Surgery Attending Physician and Team Leader, Hebei Provincial People's Hospital;Member of the Youth Committee of the China Branch of the International Vascular Union;Member of the Vascular Surgery Branch of Hebei Provincial Preventive Medical Association;Member of the Varicose Veins Group, Peripheral Vascular Disease Professional Committee, Chinese Society of Microcirculation;Member of the Varicose Veins Committee of the Hebei Vascular Health and Technology Association.

Department Introduction

The Vascular Surgery Department of Hebei Provincial People's Hospital, a key discipline in Hebei Province and a national clinical drug trial unit, is equipped with advanced hybrid operating rooms and interventional catheterization labs in China. It routinely conducts diagnosis and treatment for various peripheral vascular diseases, including: thoracic and abdominal aortic dissection, abdominal aortic aneurysm, iliac artery aneurysm, lower extremity arterial sclerosis occlusion, diabetic foot, carotid artery stenosis, subclavian artery stenosis, renal artery stenosis, varicose veins of the lower extremities, deep vein thrombosis of the lower extremities, pulmonary embolism, and other vascular diseases through interventional and open surgical treatments, as well as interventional treatment for gastrointestinal bleeding caused by portal hypertension.
