Application of DKutting® LL Peripheral Scoring Balloon in Diabetic Infrapopliteal Artery Lesions to Combat Elastic Recoil: A Case Series by Professor Huang Yuanliang’s Team

DK Medtech
Vascular Interventional Balloon Product Developer
DKutting®LL continues to use DK Medtech's unique patented triangular nitinol coil technology, combined with the actual clinical needs of lower limb arteries. It significantly increases the length of the scoring element (up to 150mm) and develops a brand-new fully coaxial balloon delivery system compatible with 0.014"/0.018" guidewires, enriching the selection of balloon diameters at 0.5mm intervals.
DK Medtech's exclusive directional scoring balloon boasts comprehensive performance with robust radial expansion and flexible axial bending. Its clinical performance has been widely recognized in both the coronary and hemodialysis access fields. The latest development, DKutting®LL Scoring Balloon Designed Specifically for Lower Limb Arterial Interventions Demonstrates Significant Clinical Advantages in Directional Dilation Mechanism, Setting a New Standard for Peripheral Vascular Pre-dilation.
DK Medtech Special Release[Professor Huang Yuanliang's Team: DKutting®Application of LL Peripheral Scoring Balloon in Anti-Recoil for Diabetic Below-the-Knee Artery Lesions: Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
DKutting®LL Peripheral Scoring Balloon
Application of Anti-Rebound in Diabetic Infrapopliteal Artery Disease
The First Affiliated Hospital of Xiamen University
Yuefeng Fan, Junmou Hong, Yuanliang Huang
Patient Information
Basic Information:Male, 73 years old.
Chief Complaint:Blood glucose elevation for 20 years, right foot ulceration for 10 days.
History of Present Illness:20 years ago, the patient developed dry mouth and polydipsia without obvious cause. The local hospital diagnosed "type 2 diabetes" and provided symptomatic treatment such as hypoglycemic therapy. In the past 5 years, the patient has repeatedly visited the local hospital for blood glucose control. Due to poor control with oral hypoglycemic agents, the patient currently uses insulin to control blood glucose. The regimen is: insulin glargine 12u qn, insulin aspart 6u tid (before meals). Blood glucose control status: 6-8 mmol/L (fasting), 14-18 mmol/L (postprandial). Two years ago, the patient experienced numbness and discomfort in the distal parts of both lower limbs, presenting a stocking-like sensation, with reduced pain, temperature, and vibration sensations in the lower limbs, accompanied by weakness and discomfort. Walking 100 meters already caused generalized soreness, and exercise tolerance gradually decreased. About 10 days before admission, ulcerations appeared on the ankle and metatarsal areas of the right lower limb. For further diagnosis and treatment, the patient visited our hospital, and the outpatient department admitted the patient to our department with diagnoses of "1. Diabetic foot 2. Type 2 diabetes."
Past Medical History:A 40-year history of hypertension, with a peak of 200/100 mmHg, managed with amlodipine. In the past month, blood pressure has decreased, with a minimum of 80/30 mmHg.
Physical Examination:
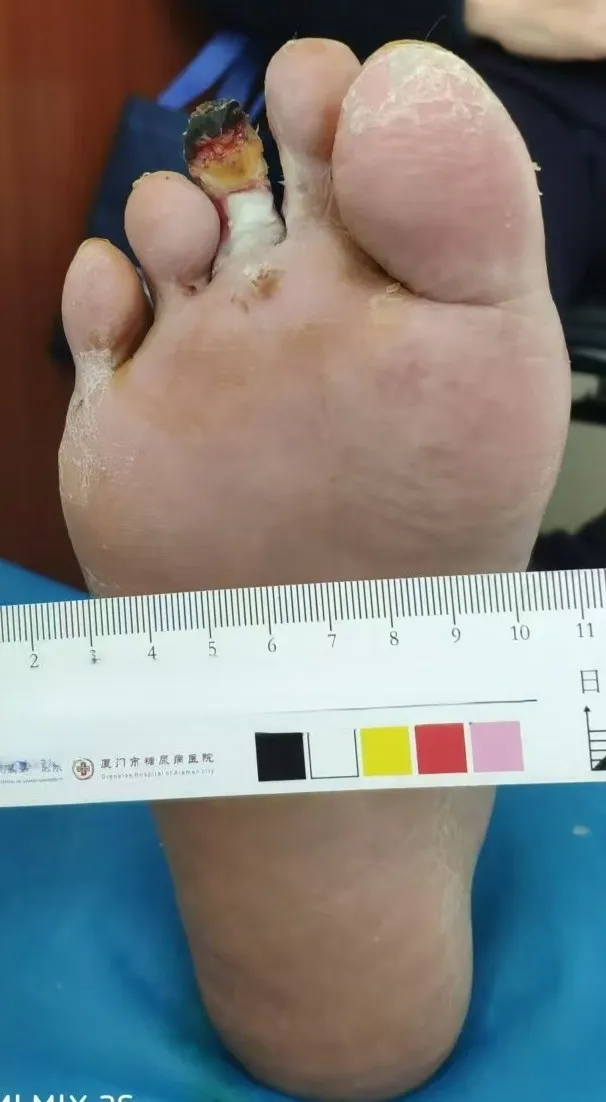
The distal end of the first phalanx of the second toe of the right foot has an ulcer, measuring 1×1 cm, with purulent secretions on the wound surface and a depth of 5 mm without bone exposure; redness and swelling are confined to the area distal to the proximal interphalangeal joint.
A 2cm×2cm ulcer with a shallow and dry appearance, and a small amount of white purulent secretion at the base, is visible on the lateral malleolus.
Arterial Palpation: Right Femoral Artery (+) Right Popliteal Artery (+) Right Anterior Tibial Artery (-) Right Posterior Tibial Artery (-).
Admission Diagnosis:
Diabetic Foot;
Lower Extremity Arteriosclerosis Obliterans;
Type 2 Diabetes with Peripheral Neuropathy;
.Renal insufficiency (CKD Stage 3);
Renal Anemia (Moderate);
Hypoproteinemia;
Hyperuricemia;
Hypertension Grade 3, Very High Risk.
Previous interventional treatment
Time | Main Treatment Process |
2025.01.09 | Lower Extremity Arteriography |
2025.01.13 | Balloon Angioplasty of the Right Lower Limb Arteries (Tibioperoneal Trunk, Posterior Tibial Artery, Anterior Tibial Artery) |
Preoperative Analysis
Preoperative Analysis:The patient is diagnosed with diabetic foot, primarily involving infrapopliteal lesions. Based on the ulcer condition, it is necessary to enhance blood perfusion of the plantar arch. The posterior tibial artery occlusion is associated with an external ankle ulcer and is an important target vessel. The patient has peripheral vascular disease due to diabetes, affecting the tunica media and intima, and elastic recoil is a significant factor impacting postoperative blood flow.
Surgical Objective:
Main Objectives:Open the anterior tibial artery and posterior tibial artery below the knee, and open the plantar arterial arch if necessary;
Secondary Objective:At least one artery should be opened to reach the sole of the foot.
Surgical Strategy/Plan:
Antegrade Approach: The patient's common femoral artery condition is relatively good, and the antegrade approach can reduce the operating distance and improve guidewire maneuverability;
0.014 Guidewire for Opening Below-the-Knee Vessels:In this case, the patient's infrapopliteal lesions are mostly segmental occlusions. A finer guidewire combined with a microcatheter can more easily pass through the following pseudo-occluded vessels; for CTO lesions, the guidewire can be replaced if necessary.
Using DKutting®LL Peripheral Scoring Balloon Reduces Elastic Recoil.
Surgical Procedure

The common femoral artery and superficial femoral artery are patent.
The superficial femoral artery and popliteal artery are patent; the anterior tibial artery shows severe stenosis at the ostium, occlusion in the middle segment with an occluded length of approximately 15 cm, and severe stenosis distally, with collateral circulation visible during the delayed phase; the tibioperoneal trunk exhibits severe stenosis with restricted blood flow; the posterior tibial artery shows severe stenosis at the ostium and is completely occluded throughout; the peroneal artery has multiple moderate stenoses along its entire course, and both the anterior and posterior communicating arteries are underdeveloped. The plantar arteries remain intact.
Antegrade puncture of the right common femoral artery was performed, and after confirmation by angiography, a 6F 55cm COOK vascular sheath was inserted into the P3 segment of the popliteal artery.

Command ES guidewire cooperated with COOK CXI catheter to pass through the occluded segment of the anterior tibial artery, and angiography confirmed; a 2.5*200mm balloon was introduced to fully dilate the anterior tibial artery.Obvious elastic recoil was observed in multiple segments of the anterior tibial artery.。
Command ES guidewire配合COOK CXI catheter passed through the occluded segment of the posterior tibial artery and confirmed by angiography; a 2.5*200mm balloon was introduced for full-length dilation of the tibioperoneal trunk and posterior tibial artery; obvious elastic recoil was observed in multiple segments of the posterior tibial artery and anterior tibial artery, with high resistance to blood flow.
Reintroduction3.0*150mm DK Cutting®LL Peripheral Scoring Balloon, fully dilating the anterior tibial artery, posterior tibial artery, and tibioperoneal trunk artery.
Angiography showed a significant reduction in elastic recoil of the anterior tibial artery, posterior tibial artery, and tibioperoneal trunk, with marked improvement in high-resistance blood flow compared to before; the plantar arch was intact with significantly improved blood flow.
Follow-up
Discharge Status:
The pulse of the patient's dorsal artery of the foot and posterior tibial artery is good; the symptom of rest pain has disappeared;
In the patient group, the wounds at the toes and lateral malleolus showed newly formed granulation tissue at the base; significant growth of the wound edges was observed.

Preoperative
One Week Postoperatively
Case Summary
Case Characteristics:
Elderly male, admitted to the hospital with a chief complaint of diabetic foot;
Revascularization of infrapopliteal arteries in diabetic foot is of great significance for wound healing.
Patients with diabetic peripheral vascular disease experience significant elastic recoil after simple balloon angioplasty.
Wound healing requires collaborative treatment involving medical therapy, wound management, vascular opening, and lumen maintenance.
Preoperative Assessment Key Points:
Infrapopliteal artery disease, multiple roots, multiple segmental occlusive lesions;
Angiosome Theory: The posterior tibial artery is an important target vessel;
Managing vascular elastic recoil and reducing no-reflow are crucial factors affecting surgical outcomes.
Surgical Strategy/Technical Key Points:
Antegrade approach, enhanced guidewire and catheter maneuverability;
0.014 guidewire passes through pseudo-occlusive lesions, CTO guidewire passes through occlusive lesions;
Peripheral scoring balloon reduces elastic recoil, achieving good lumen preparation can improve DCB treatment outcomes.
Device Features / Usage Tips:DK Medtech's Peripheral Scoring Balloon: The three scoring elements are fixed at 120° intervals on the working segment of the balloon. Upon reaching the lesion site and during expansion, the pressure from the three scoring elements focuses on the intima to achieve targeted and regular tearing. The triangular scoring elements remain fixed, applying high pressure to the vessel wall during expansion to sever the fibrous tissue in the intima, reducing random compression. Efficient expansion minimizes elastic recoil. Targeted and regular tearing of the vessel intima reduces the occurrence of dissections.

Expert Introduction

Professor Huang Yuanliang
Director of Vascular Surgery
Head of the Vascular and Tumor Intervention Department, Chief Physician, First Affiliated Hospital of Xiamen University;Member of the Interventional Physicians Branch of the Chinese Medical Doctor Association; Chairman of the Interventional Medicine Professional Committee of the Xiamen Medical Association; Vice Chairman of the Tumor Intervention Specialty Committee of the Fujian Anti-Cancer Association; Member of the Interventional Medicine Branch of the Non-Public Medical Institutions Association in China; Standing Committee Member of the Hemorrhage Specialty Committee of the Chinese Research Hospital Association; Member of the Interventional Medicine Branch of the Fujian Medical Association; Standing Committee Member of the Tumor Rehabilitation Specialty Committee of the Fujian Rehabilitation Medical Association; Standing Director of the Fujian Innovation Alliance of the National Interventional Medicine Innovation Alliance; Member of the Interventional Study Group of the Radiology Branch of the Fujian Medical Association; Director of the Integrated Traditional Chinese and Western Medicine Intervention Branch of the Chinese Medicine Information Society.

Professor Yuefeng Fan
Surgeon of This Case
The First Affiliated Hospital of Xiamen University,M.D., Associate Chief Physician.
Graduated from the Interventional Radiology program at Peking University in 2010, with nearly 20 years of experience in vascular and tumor interventions. Proficient in conventional diagnosis and treatment as well as minimally invasive interventional techniques for various vascular and tumor diseases. Specializes in minimally invasive interventional diagnosis and treatment of lower extremity arterial occlusive disease, chronic venous insufficiency, deep vein thrombosis, visceral artery diseases, and portal hypertension. Performs nearly 1,000 interventional surgeries annually.
Member of the Medical Device Special Committee of the China Pharmaceutical Education Association; Editorial Board Member of the journal "Chinese Journal of Interventional Imaging and Therapy"; Member of the Radiology Intervention Branch of the Fujian Medical Association; Member of the Intervention Branch of the Fujian Anti-Cancer Association; General Secretary of the Intervention Branch of the Xiamen Medical Association; Member of the Intervention Branch of the Xiamen Medical Association.

Professor Hong Junmou
Surgeon of This Case
The First Affiliated Hospital of Xiamen University,Ph.D., Attending Physician.
Expertise: 1) Venous diseases: Minimally invasive treatment of varicose veins in the lower extremities, pelvic venous diseases, and venous thrombosis, with over 2000 related surgeries completed; 2) Lower extremity arterial diseases: Minimally invasive treatment of arteriosclerosis obliterans and arterial thrombosis in the lower extremities, with over 800 related surgeries completed; 3) Diagnosis and treatment of aortic diseases and visceral artery diseases, with 200 related surgeries completed.
Principal Investigator of 1 project funded by the Natural Science Foundation of Fujian Province; Participant in 1 key science and technology project of Fujian Province; Principal Investigator of 1 key science and technology project of Xiamen City;
Member of the Vascular Surgery Specialty Group, Fujian Strait Medical and Health Exchange Association

Department Introduction

I. Overview of the Department
The Department of Vascular and Tumor Interventional Radiology at the First Affiliated Hospital of Xiamen University was established in 2010, consisting of clinical surgical wards, a catheterization lab, and an interventional outpatient clinic. After more than a decade of development and accumulation, the department has a strong foundation in interventional diagnosis and treatment as well as extensive clinical experience, with its comprehensive strength consistently ranking among the top in Fujian Province.
2. Medical Team
The department has a skilled, experienced, and well-structured medical team. The department currently has 9 doctors, including 1 chief physician, 4 associate chief physicians, 2 attending physicians, and 1 resident physician; 8 nurses, with 1 senior title, 4 intermediate titles, and 3 junior titles. There are 4 technicians, 2 of whom hold intermediate titles. The department includes 4 individuals with doctoral degrees and 2 with master's degrees.
3. Medical Devices
The department is equipped with a series of advanced medical devices, including four digital subtraction angiography machines, one each of intravascular ultrasound, microwave, and radiofrequency ablation instruments, as well as various high-end equipment such as ventilators and defibrillators. These advanced devices provide strong technical support for the department to carry out diagnosis and treatment of various complex diseases, meeting the diverse needs of patients and greatly improving the accuracy of disease diagnosis and the success rate of treatment.
4. The department currently performs over 2,600 surgeries annually, covering: 1. Endovascular interventional therapy, radioactive particle, radiofrequency, and microwave treatments for various benign and malignant tumors; 2. Minimally invasive surgery, open surgery, and hybrid surgery for peripheral arterial diseases; 3. Treatment of related conditions caused by cirrhosis: TIPSS procedure; 4. Minimally invasive treatment for varicose veins in the lower limbs; 5. Sclerotherapy for hemangiomas and vascular malformations; 6. Embolization therapy for acute massive bleeding.
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints, but is solely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. The information is intended for healthcare professionals to use as a reference, and should not be considered a substitute for professional medical guidance or be regarded as medical advice. If such information is used for purposes other than understanding updates, neither this platform nor the authors assume any responsibility.Contact email for collaboration:vascular@edoctor.work。
