 Abstract:Recently, "Nature Medicine》published a groundbreaking study jointly completed by teams from GSK, Stanford University, and other institutions. They analyzed data from over100 Million People's Electronic Health Records (EHR), tracked for a full16 Years (2007-2023), and controlled nearly 400 influencing factors (such as age, pre-existing conditions, medical consultation habits, etc.). The final findings revealed:Varicella-Zoster Virus (VZV) Reactivation(such as herpes zoster) andDementia RiskClosely Related —— People who repeatedly suffer from shingles have a 7-9% higher risk of dementia compared to those who have had it only once; getting the shingles vaccine can significantly reduce this risk.Reduce the Risk of Dementia, especially the two doses of recombinant vaccine (RZV), which showed better effects. More importantly, this study listed VZV reactivation as an "intervenable dementia risk factor," providing a new direction for middle-aged and elderly people to prevent dementia.
Abstract:Recently, "Nature Medicine》published a groundbreaking study jointly completed by teams from GSK, Stanford University, and other institutions. They analyzed data from over100 Million People's Electronic Health Records (EHR), tracked for a full16 Years (2007-2023), and controlled nearly 400 influencing factors (such as age, pre-existing conditions, medical consultation habits, etc.). The final findings revealed:Varicella-Zoster Virus (VZV) Reactivation(such as herpes zoster) andDementia RiskClosely Related —— People who repeatedly suffer from shingles have a 7-9% higher risk of dementia compared to those who have had it only once; getting the shingles vaccine can significantly reduce this risk.Reduce the Risk of Dementia, especially the two doses of recombinant vaccine (RZV), which showed better effects. More importantly, this study listed VZV reactivation as an "intervenable dementia risk factor," providing a new direction for middle-aged and elderly people to prevent dementia.
 1. First, understand: This virus related to dementia is actually something you've known for a long time.
1. First, understand: This virus related to dementia is actually something you've known for a long time.
Most of us had chickenpox when we were kids. After recovery, the varicella-zoster virus (VZV) does not completely disappear from the body but instead "hides" in the nerve ganglia, such as those in the spinal cord or head, where it can remain for decades.When we get older, our immunity declines, or when we encounter high stress, illness, and other situations, this "dormant" virus may "reactivate" – in medical terms, it's calledVZV Reactivation. After the virus reactivates, it will spread along the nerves, most commonly causingHerpes Zoster (HZ, commonly known as "shingles"): A string of painful blisters appears on the skin, which can be so painful that even contact with clothing may cause discomfort, and it may also leave behind long-term neuropathic pain as a sequela.Previous studies have suspected that the reactivation of VZV might be associated with dementia. For instance, some labs found that VZV infection could lead to increased production of "amyloid-β protein" (the main component of “senile plaques” in the brains of Alzheimer’s patients) in nerve cells and may also activate another herpes virus (HSV-1), indirectly harming the brain. However, these were all laboratory findings. Whether there is a clear link between VZV reactivation and dementia in real-world populations—and if so, how strong that link is—has remained uncertain. This study aims to address that question.2. 100 Million People's Data "Speaks": What's the Relationship Between Shingles and Dementia?
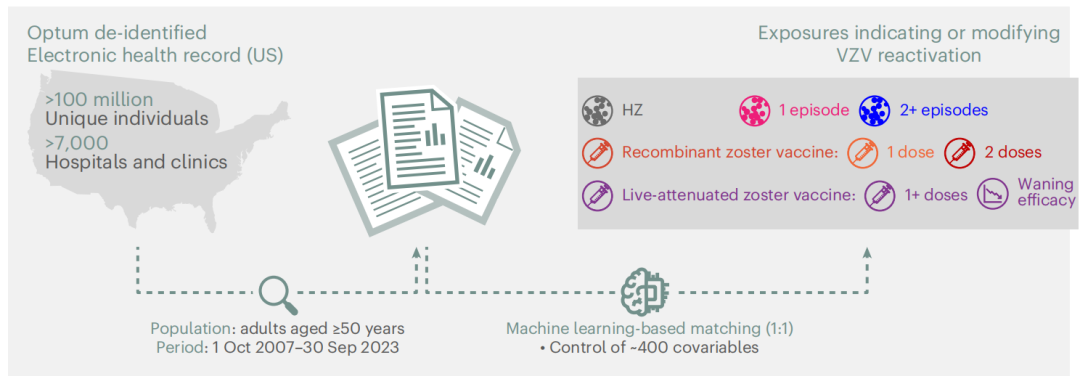
The research team used information from the American Optum database, which contains medical records of over 100 million people, covering more than 7,000 hospitals and clinics. They specifically focused on the population aged over 50 (since both dementia and shingles are highly prevalent in this age group). By using the "propensity score matching" method, they ensured that the comparison groups were similar in nearly 400 factors such as age and pre-existing conditions, making the results reliable.Figure 1 Study Design Diagram1. Recurrent Shingles, Dementia Risk Silently Rises
First, look at the relationship between "the burden of VZV reactivation" and dementia: if a person has hadMore Than Two Episodes of Herpes Zoster, compared to those who have only experienced it once, the risk of developing dementia 3-9 years later is 7-9% higher (relative risk RR=1.07-1.09, 95% confidence interval includes 1.02-1.17, indicating statistical significance).Simply put, the more frequently the virus is activated, the greater the "cumulative damage" to the brain may be, and the higher the risk of dementia in the future. The graph below clearly contrasts the cumulative risk of dementia between individuals with recurrent shingles and those with a single episode (the orange line represents the recurrent group, while the blue line represents the single-episode group; the orange line remains consistently above, indicating a higher risk):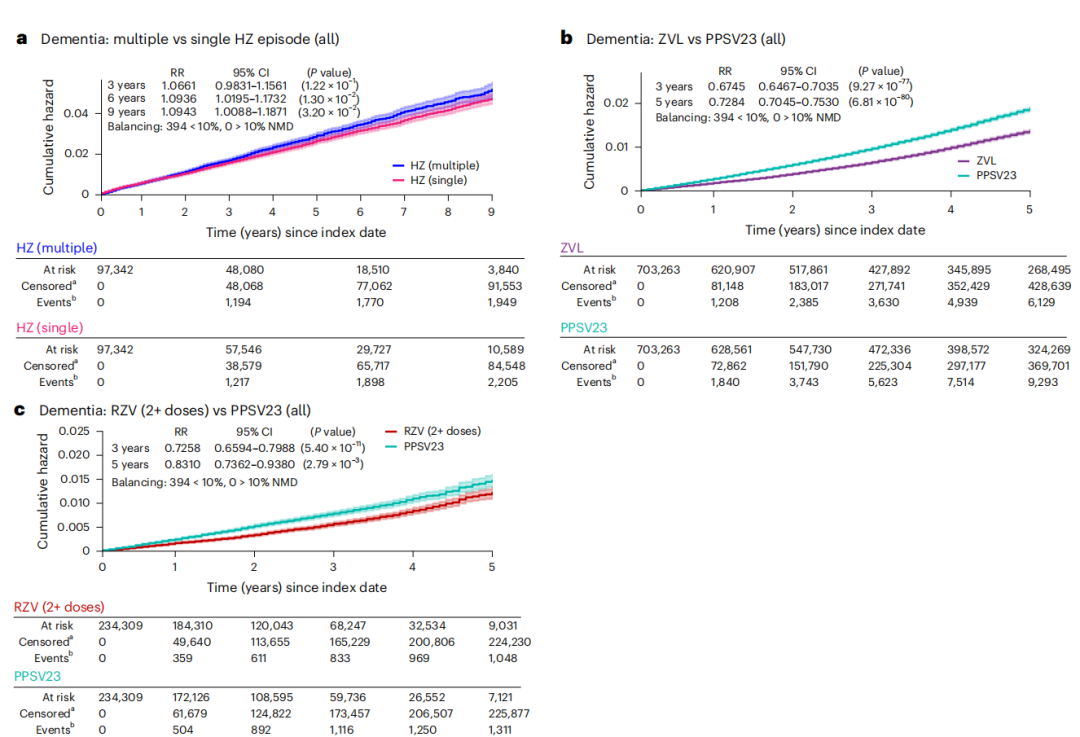 Figure 2 Comparison Chart of Exposure Factors and Dementia Risk
Figure 2 Comparison Chart of Exposure Factors and Dementia RiskNote: The Y-axis in the figure represents "Cumulative Hazard," indicating the total probability of developing dementia during the follow-up period; the X-axis represents follow-up time (years). The table shows follow-up data for two groups: "At risk" refers to the number of individuals still under follow-up at each time point, "Censored" refers to the number lost to follow-up or deceased, and "Events" refers to the number of individuals who developed dementia.
2. The Right Shingles Vaccine Can "Hit the Brakes" on Dementia
Since the reactivation of VZV increases the risk of dementia, can getting the shingles vaccine and reducing viral activation lower the risk of dementia? The research team conducted a "control experiment": using23-valent pneumococcal polysaccharide vaccine (PPSV23)When "reference" – this vaccine and the shingles vaccine have similar recommended populations (both are for people over 50 years old), but this vaccine does not prevent shingles, thus eliminating the interference of the idea that "people who get vaccinated pay more attention to their health, so they have a lower risk of dementia."StrikeLive Attenuated Zoster Vaccine (ZVL)People who received the vaccine had a 33% lower risk of developing dementia 3 years later compared to those who received the pneumonia vaccine (RR=0.67, 95% CI=0.65-0.70), and still had a 27% lower risk after 5 years (RR=0.73);
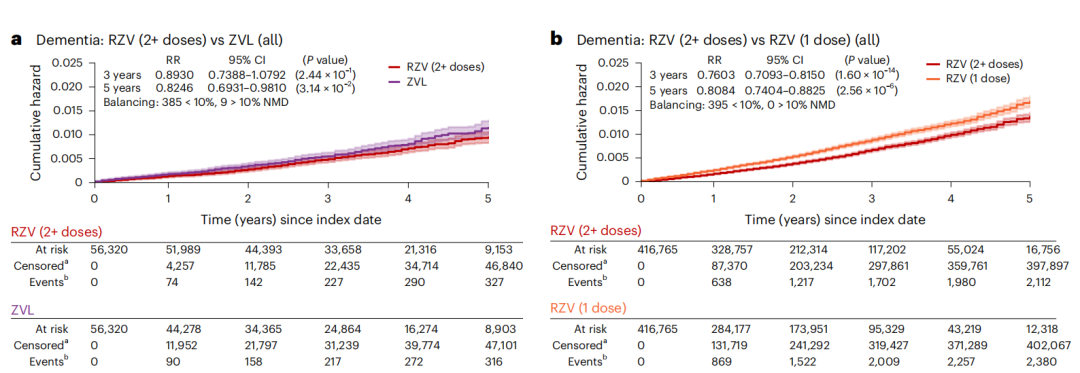
StrikeTwo doses of Recombinant Zoster Vaccine (RZV)People who received the vaccine had a 27% lower risk of dementia after 3 years (RR=0.73, 95% CI=0.66-0.80), and two doses were more effective than one — those who received two doses had a 24% lower risk of dementia after 3 years and a 19% lower risk after 5 years compared to those who received only one dose.
The two figures below respectively show the comparison between ZVL and RZV and the pneumonia vaccine. The blue line (vaccine group) is always below the red line (pneumonia vaccine group), indicating a lower risk of dementia:Figure 3 Comparison of Vaccine Types/Doses and Dementia RiskMore surprisingly, the effect of RZV is even better than ZVL: people who received two doses of RZV had an 18% lower risk of dementia after five years compared to those who received ZVL (RR=0.82, 95% CI=0.69-0.98). This is also consistent with previous understanding — RZV is a new generation vaccine, and its efficacy in preventing shingles is inherently stronger than ZVL (in clinical trials, RZV showed over 90% efficacy in preventing shingles, while ZVL only had 38%-70%).3. Vaccine protection can "expire," and the risk of dementia may "return."
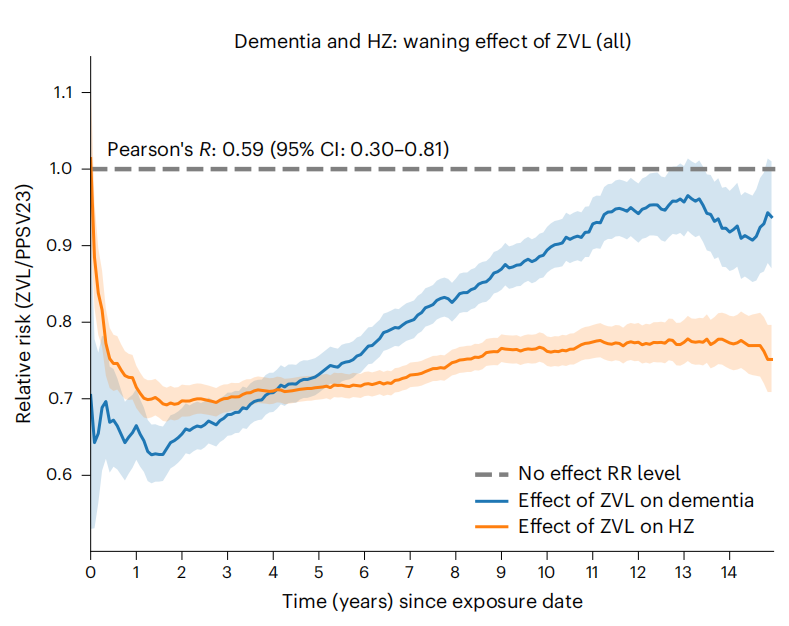
However, there is one point to note: the protective efficacy of ZVL diminishes over time. Research tracking over 15 years found that the effectiveness of ZVL in preventing shingles almost disappears after 10 years, and its effect in reducing dementia risk also "shrinks" — as the vaccine's protection wanes, the risk of dementia gradually returns to levels similar to those who did not receive the vaccine (relative risk RR approaches 1.0).The following figure shows this "synchronous attenuation": the orange line represents the effect of ZVL in preventing shingles, and the blue line represents the effect in preventing dementia. The trends of the two lines are almost identical, with a correlation coefficient (Pearson’s R) reaching 0.59, indicating a strong association between the two.Figure 4: ZVL Protection Efficacy Decay Over TimeNote: The Y-axis represents "Relative Risk (ZVL/PPSV23)", with values less than 1 indicating a lower risk in the vaccine group; the X-axis represents follow-up time (years). The dashed line indicates the "no-effect line (RR=1.0)", where the vaccine's effect disappears as the curve approaches this line.The research team speculated that this might be because the vaccine merely "delays" the progression of dementia, rather than "preventing" it – when the vaccine's protection is strong, the virus remains inactive and brain damage slows down; but once the protection wanes, the virus becomes active again, accelerating the progression of dementia.4. These Two Groups Benefit More from Vaccines in Preventing Dementia
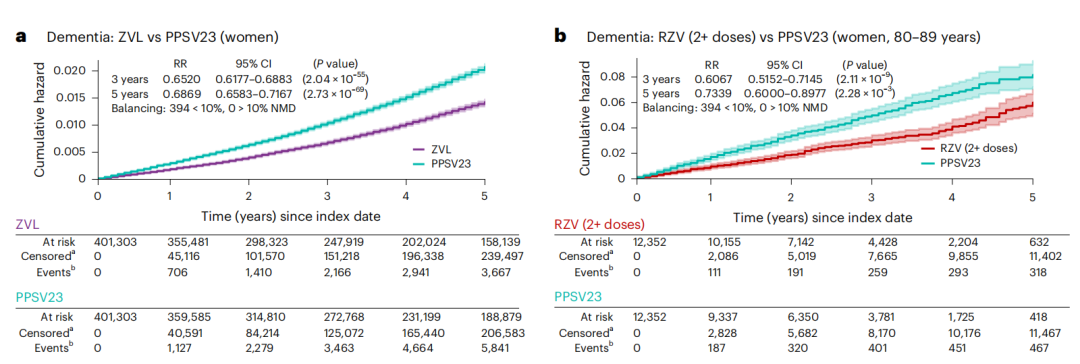
Another important finding:FemaleAndElderly People(especially those over 80 years old) This "high-risk group for shingles" shows a more significant reduction in dementia after vaccination.Women over 50 who receive ZVL have a 35% lower risk of dementia within 3 years compared to those who receive the pneumonia vaccine (33% in the general population), and a 31% lower risk within 5 years (27% in the general population).
Women aged 80-89 who receive two doses of RZV have a 39% lower risk of dementia over 3 years (27% in the general population) and a 27% lower risk over 5 years (17% in the general population).
This is easy to understand: such people inherently have a higher risk of VZV reactivation and more vulnerable brains, so the "protective benefits" from the vaccine are naturally greater. The chart below shows the comparison of dementia risk between women aged 80-89 who received the RZV and pneumonia vaccines:Figure 5 Comparison of Vaccine Effectiveness in High-Risk Populations3. Is the Research Reliable? Look at Its "Confidence" and "Regrets"
1. Why is this study highly credible?
First isLarge amount of data: More than 100 million people's real medical records, which are more convincing than previous small sample studies; secondlyStrictly Controlled: Nearly 400 influencing factors were matched, and the varicella vaccine was compared with the pneumonia vaccine to exclude the interference of "healthier people are more likely to get vaccinated"; finally,Consistent Results: Whether considering the number of viral reactivations, or vaccine type, dosage, and timing, the conclusion consistently points to "VZV reactivation increases dementia risk, while vaccines reduce the risk," with no contradictions.2. What other issues remain unresolved?
Of course, the research is not perfect either. For example:It isRetrospective Study: Can only look at "what happened in the past" and cannot randomly group like clinical trials, so it is impossible to 100% confirm that "VZV reactivation is the direct cause of dementia" (there may be undiscovered factors playing a role in between).
RZV has a short follow-up period: RZV was launched in the U.S. in 2017, and currently, there is a maximum of 6 years of follow-up data; the long-term effects still need to be awaited.
Not consideredGenetic Factors: For example, the APOE gene (a risk gene for Alzheimer's disease) was not included in the analysis;
No research on "subclinical reactivation": Some VZV reactivations do not cause shingles (referred to as "subclinical reactivation"), and it is still unclear whether such reactivation increases the risk of dementia.
4. What Should Ordinary People Do? Practical Advice for Middle-aged and Elderly People
Although the research has limitations, it already provides very clear guidance for us ordinary people (especially middle-aged and elderly individuals):People aged 50 and above should prioritize getting the shingles vaccine.: Especially for women and individuals with underlying health conditions (such as diabetes, cardiovascular diseases) — it not only prevents the severe pain associated with shingles but may also reduce the risk of dementia. If given a choice, prioritize RZV, and ensure receiving the recommended two doses (typically administered 2-6 months apart);
People who have received ZVL should pay attention to follow-up.: If ZVL was previously administered more than 10 years ago, consult a doctor about whether a booster is needed (there is currently no unified guideline for boosters, but subsequent research can be monitored);
People who have had shingles should not let their guard down: Especially for those who repeatedly experience it, pay more attention to your cognitive state (e.g., whether memorizing things or solving problems has slowed down) and undergo regular cognitive screenings.
Don't Neglect "Immunity": The core trigger for VZV reactivation is decreased immunity, so maintaining a regular routine, moderate exercise, and a balanced diet to keep immunity stable is also key to prevention.
5. Conclusion
This research serves as a wake-up call: the "latent virus" left over from childhood chickenpox could be a "hidden threat" for dementia. Fortunately, we have a simple intervention — getting the shingles vaccine. While it may not completely "eliminate" the risk of dementia, it can turn an "uncontrollable" risk into a "preventable" one. For the growing number of middle-aged and elderly people, this is already valuable news.Hopefully, more research in the future will clarify the causal relationship between VZV and dementia, and we also look forward to the emergence of longer-lasting vaccines — so that we can not only stay away from the pain of shingles but also more confidently protect brain health.Scan the WeChat QR code to add.Medicine Space-TimeEditorPlease indicate: Name + Research Direction!