Firehawk® Stent System Enables First-Ever DAPT De-escalation in Low-Risk AMI Patients

MicroPort
High-end Medical Device R&D and Manufacturer
Editor's Note:
MicroPort®Firehawk®/Firehawk®The TARGET-FIRST study of the series stent was simultaneously published in the New England Journal of Medicine (NEJM) and at the ESC 2025 Congress. Within less than two months, the one-year results of its TARGET SAFE study were presented at TCT 2025, providing substantial clinical evidence for shortening the duration of dual antiplatelet therapy (DAPT) in post-PCI patients. This was reported by Singularity Hub.
Firehawk®/Firehawk®Series of Stents Create New Waves.
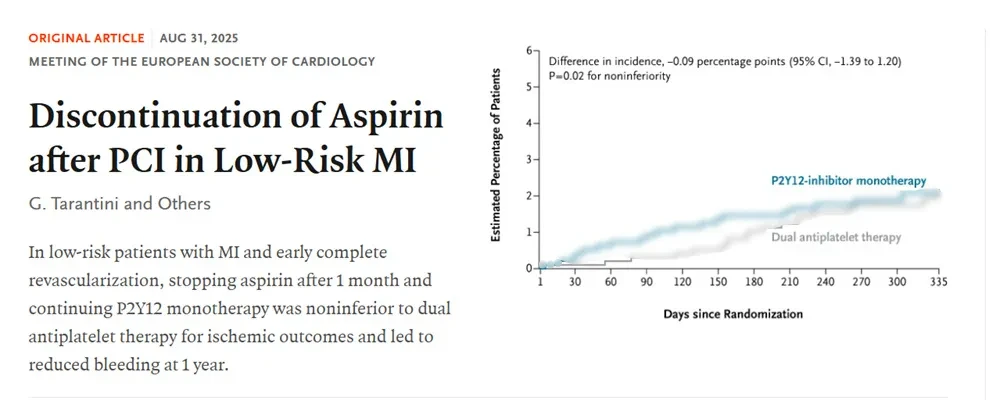
At the European Society of Cardiology Annual Congress 2025 (ESC 2025), the TARGET-FIRST study, led by Giuseppe Tarantini's team from the University of Padua, Italy, showed that for low-risk acute myocardial infarction (AMI) patients,When using Firehawk®/Firehawk®After complete revascularization with the series of stents, only one month of dual antiplatelet therapy (DAPT) is required before aspirin can be discontinued, leaving only P2Y maintenance.12Receptor Inhibitor Monotherapy;This not only does not increase the risk of ischemic events but also reduces the risk of bleeding by 54%.[1]。
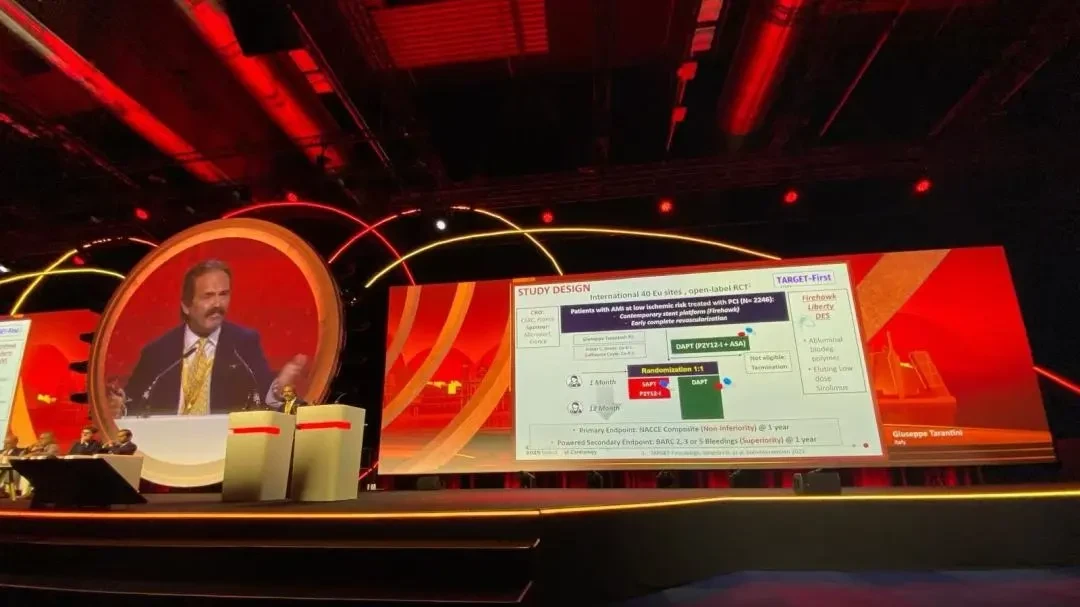
▲Release of TARGET-FIRST Study Data at ESC 2025
It is reported that the TARGET-FIRST study is also a scientistFirstIt has been confirmed in a population specifically with low-risk AMI that the DAPT course after percutaneous coronary intervention (PCI) can be shortened from 1 year to 1 month, filling the clinical gap.It is worth mentioning that this research achievement was not only published simultaneously in the top medical journal, The New England Journal of Medicine,[2], and also received recognition from the American College of Cardiology[3]And the American Heart Association[4]This has drawn attention from renowned organizations, which speaks volumes about its clinical importance.
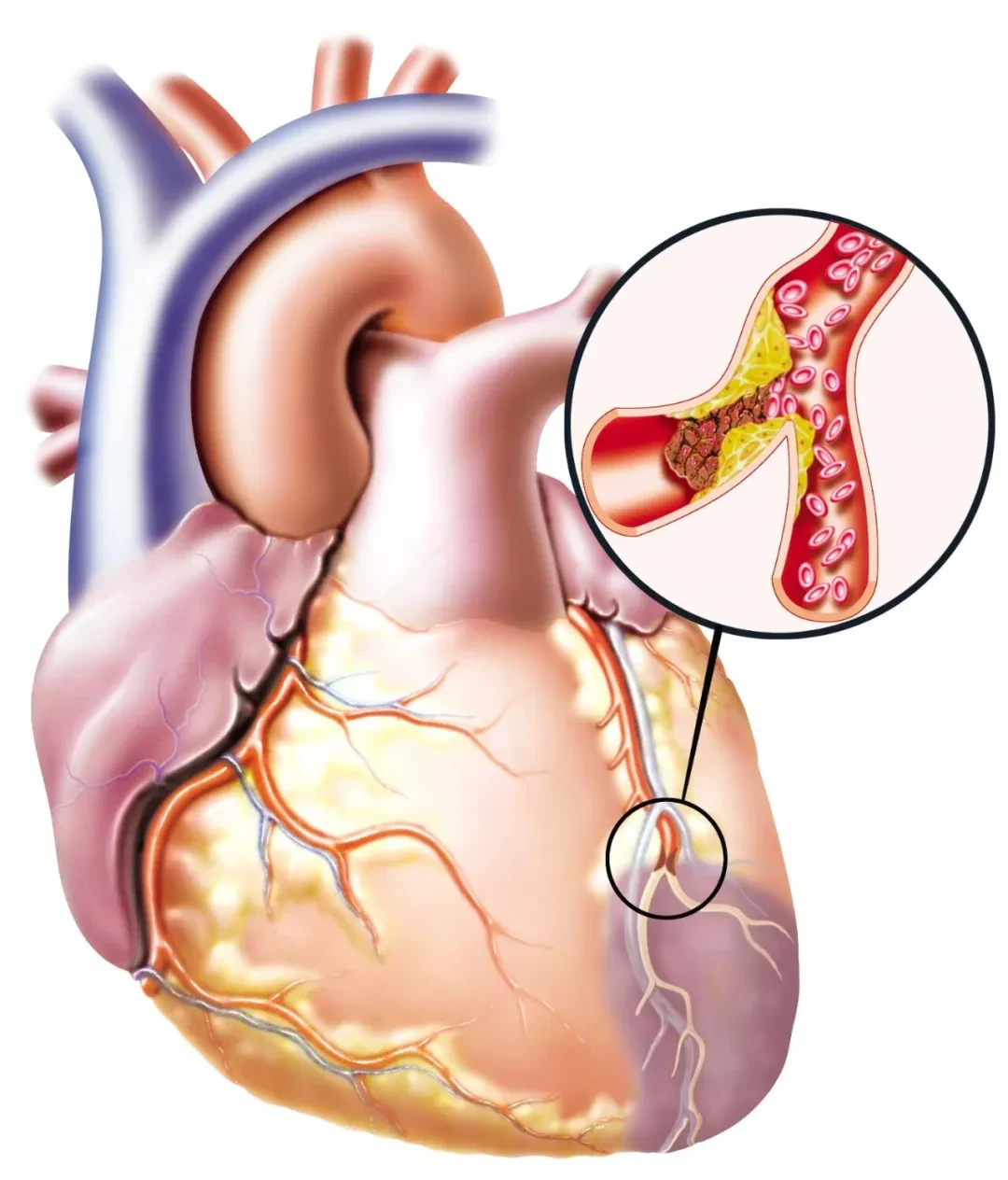
To understand why the TARGET-FIRST study has attracted such high attention, we must start with coronary atherosclerotic heart disease (coronary heart disease).
The Balancing Act of Encircling the "Number One Killer" of Human Health
Coronary heart disease, known as the "No. 1 killer" of human life and health.
According to statistics, 315 million people worldwide suffered from coronary heart disease in 2022.[5]According to the "Report on Cardiovascular Health and Diseases in China (2023)" released by China's National Center for Cardiovascular Diseases, the number of coronary heart disease patients in China has reached 11.39 million.[6]。
Although many people think that coronary heart disease is a modern illness, it is actually a very ancient disease. In 2013, researchers used CT scans on 137 mummies from 4,000 years ago and found that 34% had atherosclerosis.[7]Based on this, the researchers inferred that coronary heart disease might have already existed in pre-modern humans.
Over the past two centuries, with the acceleration of industrialization, human lifestyles and approaches to combating diseases have undergone tremendous changes. Reduced working hours, excessive calorie intake, and decreased physical activity, coupled with significantly extended life expectancy, led to coronary heart disease becoming the "number one killer" of human health by the mid-20th century.
Before the 1960s, patients with coronary heart disease suffering from acute myocardial infarction could only lie in a hospital bed waiting to die, even if they managed to reach the hospital alive. The mortality rate during hospitalization was as high as 30%. The advent of coronary angiography paved the way for the emergence of coronary artery bypass grafting (heart bypass surgery). In May 1960, the first heart bypass surgery was successfully performed.[8]; One year after this, the coronary care unit was introduced, reducing the inpatient mortality risk by half.[9]。
In 1977, German cardiologist Andreas Grüntzig performed the first percutaneous coronary angioplasty by dilating a narrowed vessel with a balloon.[8]However, the dilated area still faces issues of post-dilation occlusion and restenosis; a decade later, Ulrich Sigwart effectively addressed the problem of acute vascular occlusion after balloon dilation by implanting bare stents following the balloon expansion.[10]Today, the now widely recognized PCI was thus born.
Early PCI Used Bare-Metal Stents Fully Exposed to Blood Flow, Without Drug Coating or Polymer Protection, Causing Endothelial Damage Upon Implantation; Platelets and Coagulation Factors Contact the Exposed Metal, Easily Triggering Thrombosis. Therefore, Clinically, Aspirin + Anticoagulants (Such as Warfarin/Heparin) Were Used to Reduce Thrombosis. However, Later Studies Found That Anticoagulation May Be Unnecessary for Preventing Thrombosis, While Antiplatelet Therapy Is Key. It Was Also Proven That Compared with Traditional Anticoagulation Therapy, Using DAPT After PCI Reduces Cardiac Events as Well as Bleeding and Vascular Complications.[11]。In 1998, scientists compared three different antithrombotic regimens (aspirin alone, aspirin combined with warfarin, and aspirin combined with ticlopidine), confirming that DAPT was more effective with less bleeding.[12]`, establishing the treatment standard of preferring DAPT over long-term anticoagulation after PCI`。
However, due to reasons such as intimal hyperplasia, the restenosis rate of bare stents remains high.[13]To address this issue, drug-eluting stents loaded with anti-angiogenic drugs (such as sirolimus or paclitaxel) emerged in the early 21st century, significantly reducing the incidence of restenosis. The incidence of restenosis six months after treatment can even be reduced to 0%, compared to 26.6% with bare-metal stents.[14]Unexpectedly, 0% does not mean absolute safety, and other risks still exist. Not long after, there were research reports on the issue of late thrombosis (335 to 442 days after stent implantation) with drug-eluting stents.[15]In 2006, at the European Society of Cardiology Congress, data published by Edoardo Camenzind showed that first-generation drug-eluting stents might have higher rates of mortality and myocardial infarction compared to bare-metal stents.[16-18]The BASKET-LATE study, published in the same year, also showed that after discontinuing DAPT at 6 months post-operation, the drug-eluting stent group had a higher risk of myocardial infarction and cardiac death during the 7-18 month follow-up.[19,20]。
Due to concerns about the high risk of stent thrombosis, major guidelines worldwide have begun recommending that patients implanted with drug-eluting stents receive at least 12 months of DAPT. However,The use of DAPT can reduce the risk of thrombosis, but it also increases the risk of bleeding in patients. There was already research linking DAPT after PCI to an increased risk of bleeding and all-cause mortality.Come[21,22]"Pressing down the gourd floats the dipper," balancing ischemia and bleeding in CAD patients after PCI is indeed not that easy.
Ischemia and Blood Loss: Continuously Improving Balance Strategies
With the emergence of a new generation of drug-eluting stents featuring lower drug dosages and better biocompatibility, the risk of late stent thrombosis has been further reduced, reigniting scientists' interest in improving antiplatelet therapy strategies. They have begun attempting to shorten the duration of DAPT by focusing on different risk populations.
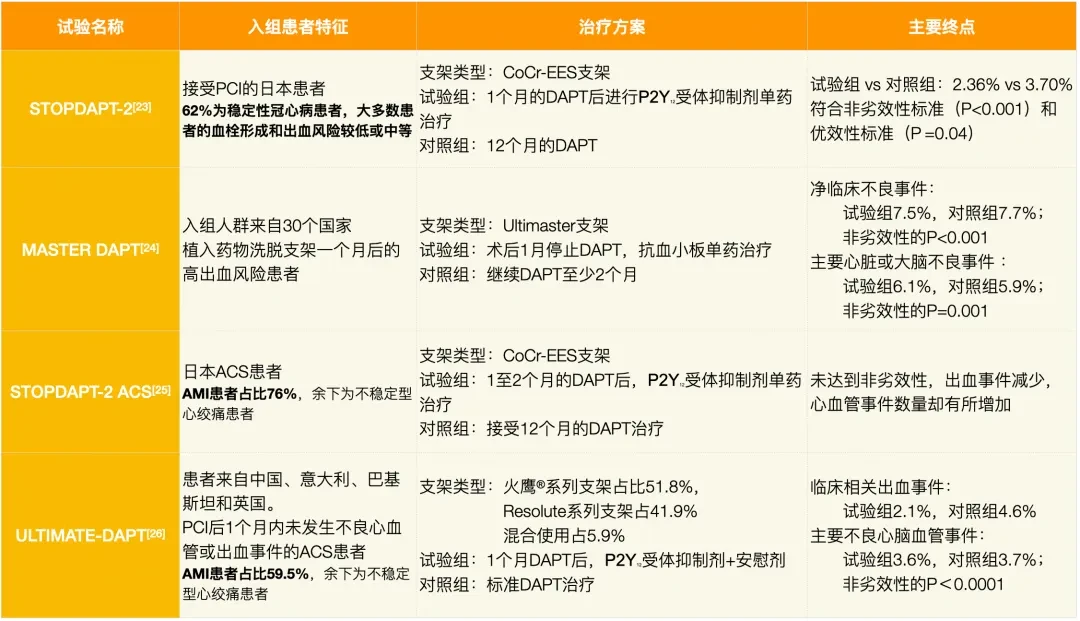
▲Some representative studies on the shortening of DAPT (Click to view larger image)
For example, as shown in the table above, the STOPDAPT-2 trial initiated in 2015[23]Indicates,For patients with stable coronary heart disease and low to moderate risk of thrombosis or bleeding, a 1-month course of DAPT may be sufficient.; The MASTER DAPT trial, initiated in 2017[24]Confirmed,In high bleeding risk populations, one month of DAPT can reduce the incidence of major bleeding or clinically relevant non-major bleeding without increasing net clinical adverse events and major cardiac or cerebral adverse events (6.5% vs 9.4%).。
However, in the high-risk group of AMI (including STEMI and NSTEMI) with a higher risk of ischemia, there are no targeted randomized controlled trials. Only a few studies have explored the impact of shortening DAPT in the broader population of acute coronary syndrome (ACS, including unstable angina and AMI), but the results have been inconsistent.
For example, the STOPDAPT-2 ACS study[25]Display,For ACS patients who have successfully undergone PCI, receive P2Y after 1 to 2 months of DAPT12Receptor Inhibitor Monotherapy Did Not Achieve Non-Inferiority in Net Clinical Benefit Rate Compared to 12-Month DAPT, Although Bleeding Events Decreased (0.54% vs 1.17%), the Number of Cardiovascular Events Increased (2.76% vs 1.86%).. The ULTIMATE-DAPT study, led by the team from Nanjing Hospital affiliated with Nanjing Medical University, found that[26],In ACS patients who underwent PCI treatment and used 1 month of DAPT without severe adverse events, compared with continuing DAPT, subsequent switching to P2Y12Receptor inhibitor monotherapy significantly reduced the risk of clinically relevant bleeding, and the two treatment groups had similar rates of major adverse cardiovascular and cerebrovascular events.
However, the proportions of AMI patients in the two studies mentioned above (76% and 59.5%) differ significantly, and the P2Y used12There are also differences in receptor inhibitors, and the results are inconsistent, making attempts to shorten DAPT duration for AMI patients still fraught with uncertainty. There is an urgent need for more targeted prospective clinical studies to explore the impact of shortening DAPT on AMI patients.
Fill the Gap
The multicenter, open-label, randomized controlled clinical trial initiated in 2021 (TARGET-FIRST study) filled the aforementioned gap.[2]。
The study recruited 2,246 patients with AMI across 40 research centers in Europe. All patients were required to undergo PCI treatment within 7 days of onset and achieve complete revascularization (all significant stenotic lesions treated, with stents provided by MicroPort).®Independently Developed Firehawk®/Firehawk®Series Coronary Rapamycin Drug-Targeted Eluting Stent System), followed by one month of standard DAPT (aspirin combined with a potent P2Y12 receptor inhibitor, where 74% used ticagrelor, 20.9% used prasugrel, and 5.1% used clopidogrel) post-procedure. Subsequently, patients without ischemic or major bleeding events were randomly assigned to two groups: one group received monotherapy with a P2Y12 receptor inhibitor (73.5% used ticagrelor, 21.7% used prasugrel, and 4.8% used clopidogrel) for 11 months, while the other group continued DAPT treatment for 11 months. A total of 1,942 patients completed randomization.
▲Firehawk®/Firehawk®TARGET-FIRST Study
Published in The New England Journal of Medicine
The primary endpoint of the study was a composite endpoint consisting of all-cause death, myocardial infarction, stent thrombosis, stroke, or major bleeding (Bleeding Academic Research Consortium [BARC]–defined type 3 or type 5 bleeding events) over 11 months after randomization; the main secondary endpoint was BARC type 2, 3, or 5 bleeding (clinically relevant bleeding events) at 11 months after randomization.
In terms of the primary endpoint,P2Y12The primary composite endpoint event rate was 2.1% in the receptor inhibitor monotherapy group and 2.2% in the continued DAPT group, meeting the non-inferiority hypothesis (non-inferiority P=0.02); the incidence of clinically relevant bleeding events was 2.6% and 5.6%, respectively (HR=0.46, superiority P=0.002), indicating P2Y12The risk of bleeding in the receptor inhibitor monotherapy group was reduced by 54% compared to the continued DAPT therapy group.。
As is known to all, there is an "East Asian Paradox" in the field of coronary heart disease, which means that compared with Western populations, East Asian patients with coronary heart disease have a lower risk of cardiovascular events during antiplatelet therapy but a higher risk of severe bleeding.[27]Therefore, for AMI patients in China, prolonged DAPT may bring a higher risk of bleeding, making the need to shorten the DAPT course extremely urgent. The results of the TARGET-FIRST study hold significant reference value for the clinical treatment of AMI patients in China.
The breakthrough results of the TARGET-FIRST study may be related to Firehawk.®/Firehawk®Firehawk®/Firehawk®The innovative design of the series of stents is inseparable. Firehawk®/Firehawk®The series stent is the third-generation coronary drug-eluting stent system independently developed by Chinese enterprises. Compared with existing drug-eluting stents,Firehawk®/FireHawk®The design of the series stent is very unique, featuring an intermittent single-sided groove drug-loading and polymer-controlled release design.,Can ensure that the drug/polymer coating encapsulated in the groove is released only after reaching the vascular lesion area.
This design significantly reduces the drug dosage while ensuring the drug's efficacy, requiring only one-third of the drug-loading capacity of similar products to achieve equivalent therapeutic effects, and greatly enhances safety. It combines the "low restenosis rate" characteristic of drug-eluting stents with the "extremely low late thrombosis rate" advantage of bare-metal stents.[28]In the TARGET-FIRST study, the incidence of stent thrombosis during the follow-up period was very low, with only one event occurring.[2]. There is no doubt that the success of the TARGET-FIRST study is a testament to Firehawk®/FireHawk®Another validation of the safety and effectiveness of the unique design of the series of stents.
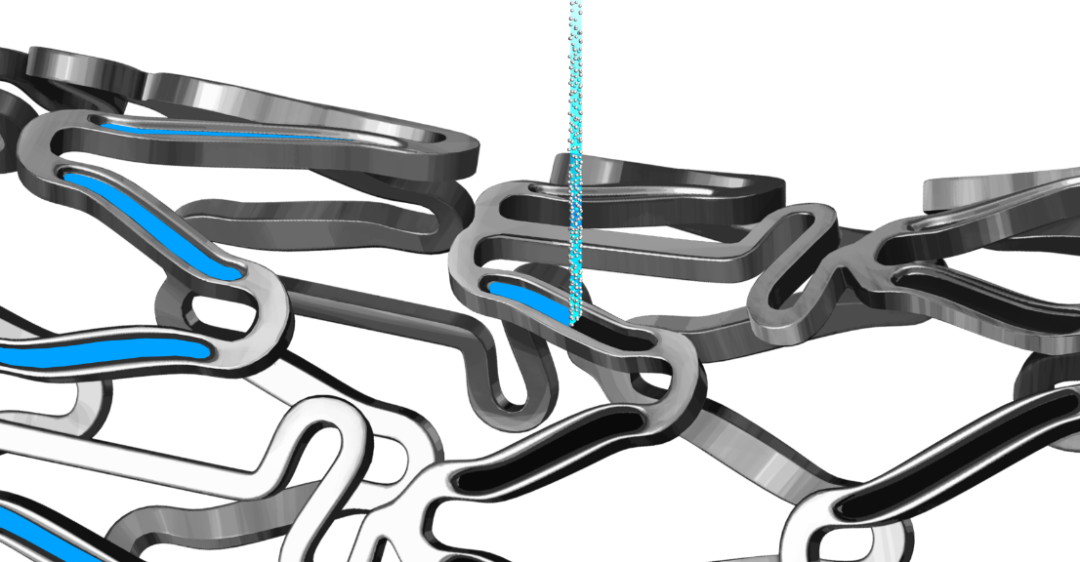
▲Firehawk®/Firehawk®Series Stent
In fact, in terms of DAPT de-escalation, Firehawk®/Firehawk®The series of stents have conducted a total of three different types of research, including TARGET-FIRST.
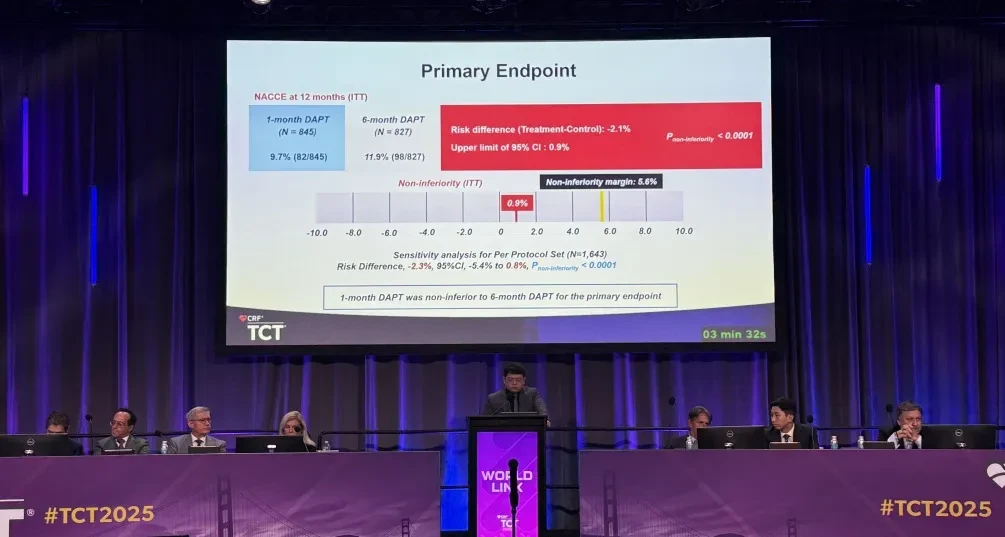
On October 25, the TARGET SAFE study led by Academician Han Yaling and her team was released at the 2025 Transcatheter Cardiovascular Therapeutics (TCT 2025) conference:High bleeding risk patients implanted with Firehawk®/FireHawk®After the series of stents, shortening the DAPT course from 6 months to 1 month is safe and effective. The 12-month net adverse clinical cerebrovascular events (NACCE) rate was 9.7% in the 1-month DAPT group and 11.9% in the 6-month DAPT group (non-inferiority P<0.0001).[29]. This finding not only indicates that high bleeding risk populations did not experience increased ischemic risk with a shorter DAPT regimen, but also the bleeding risk in the 1-month DAPT group was numerically lower than that in the 6-month DAPT group.
▲Release of TARGET SAFE Study Data at TCT 2025
Moreover, at last year's TCT conference, the TARGET DAPT study based on real-world populations showed no significant difference in the primary endpoint events (18-month NACCE) between the 3-month DAPT group and the 12-month DAPT group (10.14% vs 10.90%; non-inferiority P=0.0003). The incidence of major bleeding events between 3 months and 18 months was significantly lower in the 3-month DAPT group compared to the 12-month DAPT group.[30], further proving that Firehawk®/Firehawk®The Safety and Efficacy of the Series Stent Under a Short-Term DAPT Strategy. These three studies all highlight Firehawk.®/Firehawk®The Safety and Innovative Value of the Series Stents in Global Clinical Practice.
▲ Data release session of the TARGET DAPT study at TCT 2024
Overall, with the advancement of modern PCI technology and drug therapy, DAPT is gradually moving from a "fixed duration" to an "individualized duration" tailored for specific patient populations.The success of the TARGET-FIRST study fills an important gap in clinical practice and provides strong clinical support for shortening the DAPT regimen in low-risk AMI patients.。It is worth mentioning that,Firehawk®/Firehawk®The three short-term DAPT studies of the series stents have cumulatively enrolled 6,500 patients, covering real-world populations, high bleeding risk patients, and low-risk myocardial infarction patient groups. These studies have accumulated substantial clinical evidence and demonstrated safe and robust efficacy.
It is foreseeable that, with the support of these clinical studies, individualized reduction of medication after PCI in patients with coronary heart disease is gradually becoming possible and deserves consideration in clinical practice.
References:
[1].https://www.escardio.org/The-ESC/Press-Office/Press-releases/Early-aspirin-discontinuation-linked-to-benefits-in-low-risk-patients-with-myocardial-infarction-undergoing-coronary-stenting
[2].Tarantini G, Honton B, Paradies V, et al. Early Discontinuation of Aspirin after PCI in Low-Risk Acute Myocardial Infarction. N Engl J Med. Published online August 31, 2025. doi:10.1056/NEJMoa2508808
[3].https://www.acc.org/latest-in-cardiology/articles/2025/08/26/11/47/sun-1045am-aspirin-esc-2025
[4].https://www.youtube.com/watch?v=edAnYwSp9h4
[5].Stark, B, Johnson, C, Roth, G. GLOBAL PREVALENCE OF CORONARY ARTERY DISEASE: AN UPDATE FROM THE GLOBAL BURDEN OF DISEASE STUDY. JACC. 2024 Apr, 83 (13_Supplement) 2320.
https://doi.org/10.1016/S0735-1097(24)04310-9
[6].https://www.nccd.org.cn/Sites/Uploaded/File/2024/12/%E4%B8%AD%E5%9B%BD%E5%BF%83%E8%A1%80%E7%AE%A1%E5%81%A5%E5%BA%B7%E4%B8%8E%E7%96%BE%E7%97%85%E6%8A%A5%E5%91%8A(2023)-%E6%9C%80%E5%90%8E%E7%89%88.pdf
[7].Thompson RC, Allam AH, Lombardi GP, et al. Atherosclerosis across 4000 years of human history: the Horus study of four ancient populations. Lancet. 2013;381(9873):1211-1222. doi:10.1016/S0140-6736(13)60598-X
[8].Doenst T, Thiele H, Haasenritter J, Wahlers T, Massberg S, Haverich A. The Treatment of Coronary Artery Disease—Current Status Six Decades After the First Bypass Operation. Dtsch Arztebl Int. 2022;119(42):716-723. doi:10.3238/arztebl.m2022.0277
[9].Nabel EG, Braunwald E. A tale of coronary artery disease and myocardial infarction. N Engl J Med. 2012;366(1):54-63. doi:10.1056/NEJMra1112570
[10].Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med. 1987;316(12):701-706. doi:10.1056/NEJM198703193161201
[11].Schömig A, Neumann FJ, Kastrati A, et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med. 1996;334(17):1084-1089. doi:10.1056/NEJM199604253341702
[12].Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators. N Engl J Med. 1998;339(23):1665-1671. doi:10.1056/NEJM199812033392303
[13].Burt HM, Hunter WL. Drug-eluting stents: a multidisciplinary success story. Adv Drug Deliv Rev. 2006;58(3):350-357. doi:10.1016/j.addr.2006.01.014
[14].Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stent with a standard stent for coronary revascularization. N Engl J Med. 2002;346(23):1773-1780. doi:10.1056/NEJMoa012843
[15].McFadden EP, Stabile E, Regar E, et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet. 2004;364(9444):1519-1521. doi:10.1016/S0140-6736(04)17275-9
[16].Camenzind E, Steg PG, Wijns W. Stent thrombosis late after implantation of first-generation drug-eluting stents: a cause for concern. Circulation. 2007;115(11):1440-1455. doi:10.1161/CIRCULATIONAHA.106.666800
[17].Nordmann AJ, Briel M, Bucher HC. Mortality in randomized controlled trials comparing drug-eluting vs. bare metal stents in coronary artery disease: a meta-analysis. Eur Heart J. 2006;27(23):2784-2814. doi:10.1093/eurheartj/ehl282
[18].Byrne RA, Kastrati A, Hausleiter J. The battle against stent thrombosis--to protect and to serve. Lancet. 2012;380(9851):1365-1367. doi:10.1016/S0140-6736(12)61385-3
[19].Pfisterer M, Brunner-La Rocca HP, Buser PT, et al. Late clinical events after clopidogrel discontinuation may limit the benefit of drug-eluting stents: an observational study of drug-eluting versus bare-metal stents. J Am Coll Cardiol. 2006;48(12):2584-2591. doi:10.1016/j.jacc.2006.10.026
[20].Harrington RA, Califf RM. Late ischemic events after clopidogrel cessation following drug-eluting stenting: should we be worried?. J Am Coll Cardiol. 2006;48(12):2592-2595. doi:10.1016/j.jacc.2006.10.025
[21].Palmerini T, Benedetto U, Bacchi-Reggiani L, et al. Mortality in patients treated with extended duration dual antiplatelet therapy after drug-eluting stent implantation: a pairwise and Bayesian network meta-analysis of randomised trials. Lancet. 2015;385(9985):2371-2382. doi:10.1016/S0140-6736(15)60263-X
[22].Généreux P, Giustino G, Witzenbichler B, et al. Incidence, Predictors, and Impact of Post-Discharge Bleeding After Percutaneous Coronary Intervention. J Am Coll Cardiol. 2015;66(9):1036-1045. doi:10.1016/j.jacc.2015.06.1323
[23].Watanabe H, Domei T, Morimoto T, et al. Effect of 1-Month Dual Antiplatelet Therapy Followed by Clopidogrel vs 12-Month Dual Antiplatelet Therapy on Cardiovascular and Bleeding Events in Patients Receiving PCI: The STOPDAPT-2 Randomized Clinical Trial. JAMA. 2019;321(24):2414-2427. doi:10.1001/jama.2019.8145
[24].Valgimigli M, Frigoli E, Heg D, et al. Dual Antiplatelet Therapy after PCI in Patients at High Bleeding Risk. N Engl J Med. 2021;385(18):1643-1655. doi:10.1056/NEJMoa2108749
[25].Watanabe H, Morimoto T, Natsuaki M, et al. Comparison of Clopidogrel Monotherapy After 1 to 2 Months of Dual Antiplatelet Therapy With 12 Months of Dual Antiplatelet Therapy in Patients With Acute Coronary Syndrome: The STOPDAPT-2 ACS Randomized Clinical Trial. JAMA Cardiol. 2022;7(4):407-417. doi:10.1001/jamacardio.2021.5244
[26].Ge Z, Kan J, Gao X, et al. Ticagrelor alone versus ticagrelor plus aspirin from month 1 to month 12 after percutaneous coronary intervention in patients with acute coronary syndromes (ULTIMATE-DAPT): a randomised, placebo-controlled, double-blind clinical trial. Lancet. 2024;403(10439):1866-1878. doi:10.1016/S0140-6736(24)00473-2
[27].Gong Y, Jeong YH, Wang TD, et al. Position Statement on Antiplatelet Therapy for East Asians With Coronary Artery Disease: 2025 Update. JACC Asia. 2025;5(7):821-846. doi:10.1016/j.jacasi.2025.04.010
[28].Lansky AJ, Xu B, Baumbach A, et al. Targeted therapy with a localised abluminal groove, low-dose sirolimus-eluting, biodegradable-polymer coronary stent - five-year results of the TARGET All Comers randomised clinical trial. EuroIntervention. 2023;19(10):e844-e855. Published 2023 Dec 4. doi:10.4244/EIJ-D-23-00409
[29].https://mp.weixin.qq.com/s/hEhogfBCJS274bnu_ajq0g
[30].https://www.microport.com.cn/news/xinwendongtai/2146.html
Click belowRead the original textView Link