Professor Zhang Lihong's Team: A Case of Repeated Arteriovenous Fistula Stenosis Treated with Dissolve® AV High-Pressure Scoring Drug-Coated Balloon

DK Medtech
Vascular Interventional Balloon Product Developer

Stenosis of autologous or artificial arteriovenous fistula (AVF/AVG) is the most common complication in hemodialysis patients. Percutaneous transluminal angioplasty (PTA) has become the primary method for maintaining dialysis access. However, the blunt and irregular tearing of the intima and part of the media by traditional balloons during PTA can cause excessive damage to the endothelial vessels, leading to intense proliferation of vascular smooth muscle cells and macrophages, which rapidly results in restenosis.
In recent years, there have been continuous international explorations and clinical studies on drug-coated balloons for PTA treatment of dialysis access. DK Medtech has developed Dissolve.®AV High-Pressure Scoring Drug-Coated Balloon, integrating "scoring," "high pressure," and "drug coating" three features in one, is the world's first third-generation drug balloon:
Directional Scoring: Uniform and regular tearing of the intima to reduce damage from blunt rupture.
High Burst Pressure: For high-resistance lesions, improving technical success rate.
Paclitaxel Coating: Effectively Inhibits Excessive Proliferation of Smooth Muscle Cells.
DK Medtech Special Release[Professor Zhang Lihong's Team: Dissolve]®A Case of AV High-Pressure Scoring Drug-Coated Balloon Treatment for Recurrent Stenosis in Access Pathways, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, strengthen technical exchanges and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
Patient Information
Basic Information:Male, 45 years old.
Chief Complaint:Six years after the internal fistula surgery, with four months of poor internal fistula function.
History of Present Illness:Six years ago, the patient visited a "certain tertiary hospital" due to edema. At that time, the blood creatinine level was found to be 700 umol/L, and chronic kidney disease stage 5 was considered. The patient was given oral traditional Chinese medicine and temporary catheter hemodialysis treatment. After the condition improved, an arteriovenous fistula surgery was performed on the left upper limb. Two months after the surgery, dialysis using the fistula began, 3 times per week. Blood pressure started to rise after dialysis, requiring long-term oral antihypertensive medication. In October 2020, the patient experienced decreased fistula blood flow and stenosis of the cephalic vein after the anastomosis. The patient refused balloon dilation and underwent another fistula reconstruction surgery at the site of the stenosis. After the surgery, collateral stenosis of the fistula occurred, which was managed surgically. After May 2022, due to repeated stenosis of the AVF, PTA surgery was performed.
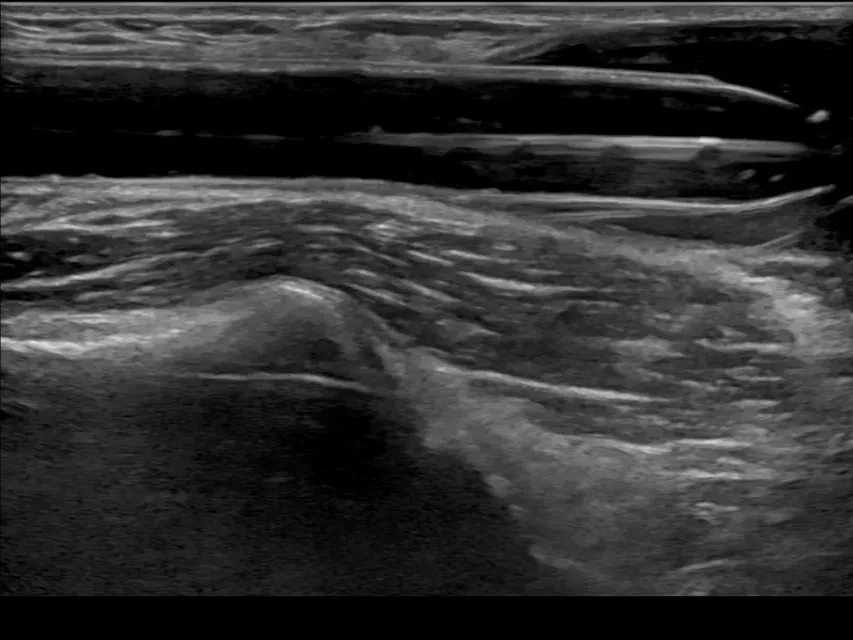
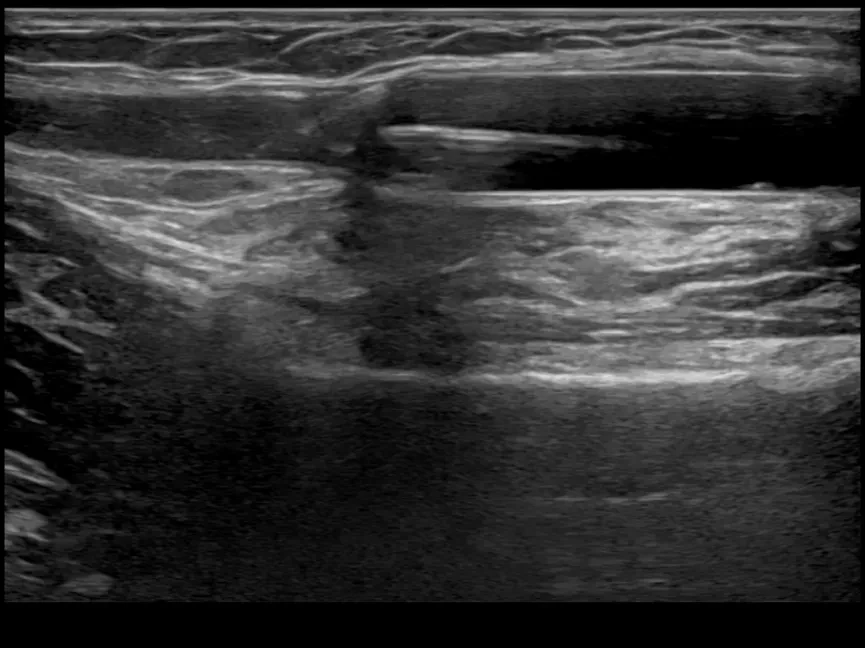
Physical Examination:Two aneurysmal dilations are visible in the forearm of the left upper limb arteriovenous fistula. The pulsation is enhanced and thrill is weakened at the aneurysmal dilation of the cephalic vein posterior to the anastomosis. The pulsation is slightly weakened but still predominant at the aneurysmal dilation of the median vein of the forearm, 4 cm below the elbow. The pulsation disappears at the proximal end of the median cubital vein near the heart, with localized enhancement of thrill.
Previous interventional treatment
Time | Main Treatment Process |
2022-05-20 | Applied MUSTANG 6x20mm (High-Pressure Balloon) to dilate the stenotic segment of the cephalic vein collateral, with balloon pressure at 24atm. |
2022-08-16 | Applied CONQUEST 7x40mm (High-Pressure Balloon) to dilate the stenotic segment of the basilic vein, with a balloon pressure of 28atm (a total of 3 dilations). |
2023-03-07 | Applied CONQUEST 8*40mm (high-pressure balloon) to dilate the stenotic segment of the basilic vein at the elbow, with a balloon pressure of 26atm (a total of 3 dilations). |
2023-06-06 | Applied MUSTANG 6*40mm (high-pressure balloon) to dilate the stenotic segment of the median cephalic vein in the forearm, with a balloon pressure of 24atm. Applied CONQUEST 8*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, balloon pressure 2atm → 22atm (gradually increased). |
2023-10-10 | Applied DK Medtech 6*40mm (high-pressure balloon) to dilate the stenotic segment of the median vein in the forearm, with a balloon pressure of 20atm. |
2024-01-02 | Applied MUSTANG 6*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, with a balloon pressure of 24atm (elastic recoil, suboptimal effect). Applied MUSTANG 6*40mm (High-Pressure Balloon) to dilate the stenotic segment of the median cephalic vein in the forearm, with a balloon pressure of 24atm (satisfactory result). Applied CONQUEST 8*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, with a balloon pressure of 26atm. |
2024-05-30 | Applied MUSTANG 6*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, with a balloon pressure of 24atm (elastic recoil, suboptimal effect). Applied MUSTANG 6*40mm (high-pressure balloon) to dilate the stenotic segment of the median cephalic vein in the forearm, with a balloon pressure of 24atm (satisfactory result). Applied CONQUEST 8*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, with a balloon pressure of 26atm. |
2024-09-10 | Applied CONQUEST 10*40mm (High-Pressure Balloon) to dilate the stenotic segment of the cephalic vein, with balloon pressure at 24atm. Applied MUSTANG 6*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, with a balloon pressure of 24atm. |
2024-12-03 | Applied CONQUEST 8*40mm (High-Pressure Balloon) to dilate the stenotic segment of the median cubital vein, with balloon pressure at 30atm. Applied MUSTANG 5*40mm (high-pressure balloon) to dilate the stenotic segment of the mid-forearm cephalic vein, with a balloon pressure of 24atm. |
2025-03-11 | Applied CONQUEST 8*40mm (high-pressure balloon) to dilate the stenotic segment of the median cubital vein, with a balloon pressure of 30atm. |
2025-07-03 | Applied CONQUEST 8*40mm (High-Pressure Balloon) to dilate the stenotic segment of the basilic vein, with a balloon pressure of 28atm. Applied CONQUEST 6*40mm (high-pressure balloon) to dilate the mid-forearm venous stenosis segment, with a balloon pressure of 28atm. |
2025/7/17 | Bleeding at the puncture site after balloon dilation and disinfection, followed by surgical debridement with skin wound excision. |
Preoperative Analysis
Preoperative Analysis:The patient has been on hemodialysis for 6 years and is currently undergoing dialysis treatment with an arteriovenous fistula in the left upper limb. The patient experiences recurrent intimal hyperplasia and stenosis of the arteriovenous fistula in the left upper limb and has undergone multiple balloon angioplasty procedures for the arteriovenous fistula in the past.
Surgical Objective:
Main Objectives:Perform dilation on the proximal and distal stenotic areas of the aneurysmal expansion of the median cubital vein near the arteriovenous fistula, to relieve the increased AVF pressure caused by the stenotic lesion.
Secondary Objectives:Inhibition of AVF Venous Intimal Hyperplasia and Prolongation of AVF Patency Rate through Notched Drug-Coated Balloons.
Surgical Procedure
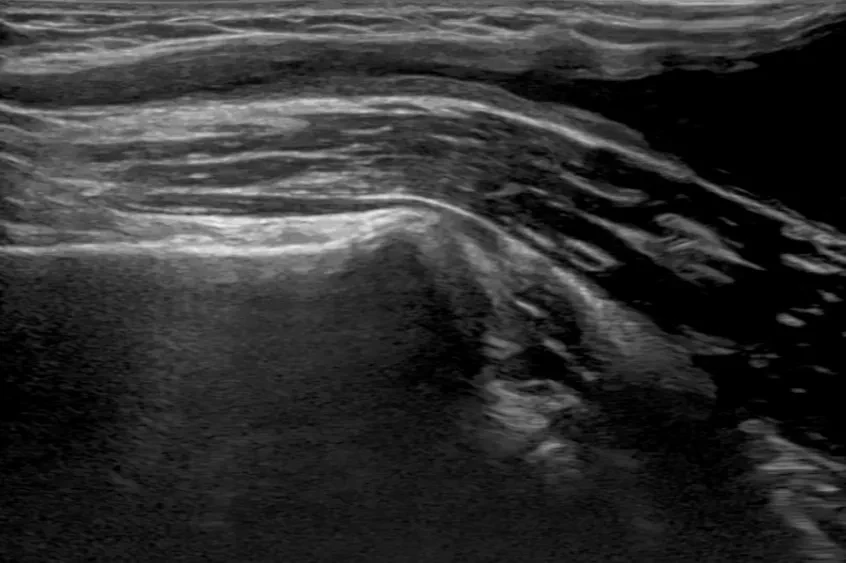

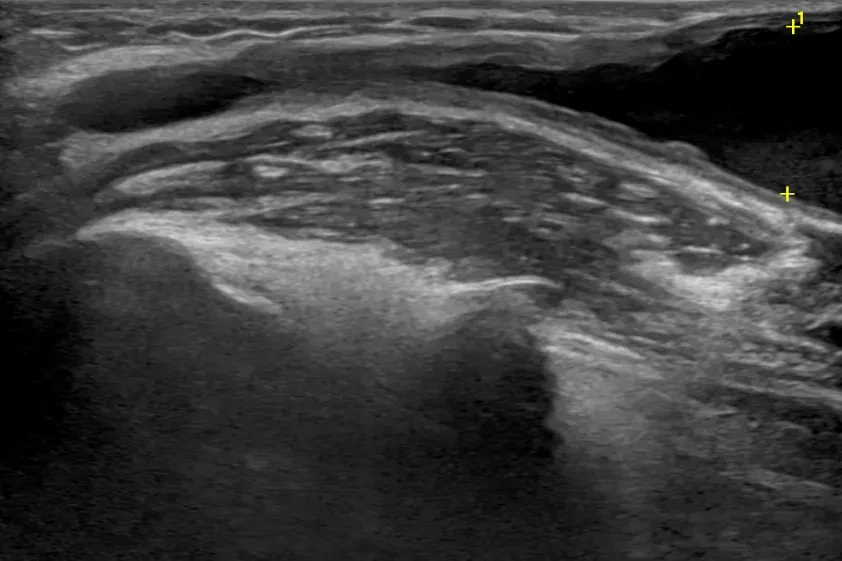
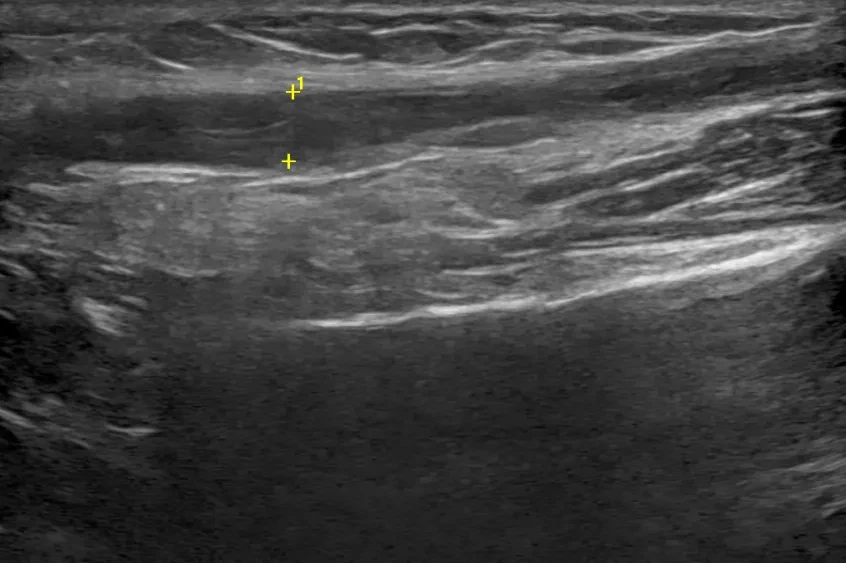
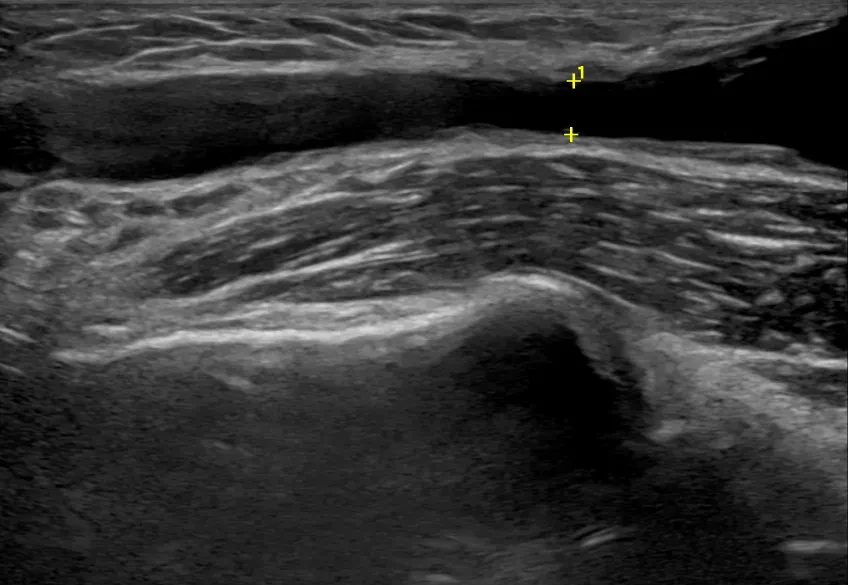
Proximal elbow median vein stenosis segment with severe intimal hyperplasia and tumor-like dilation.
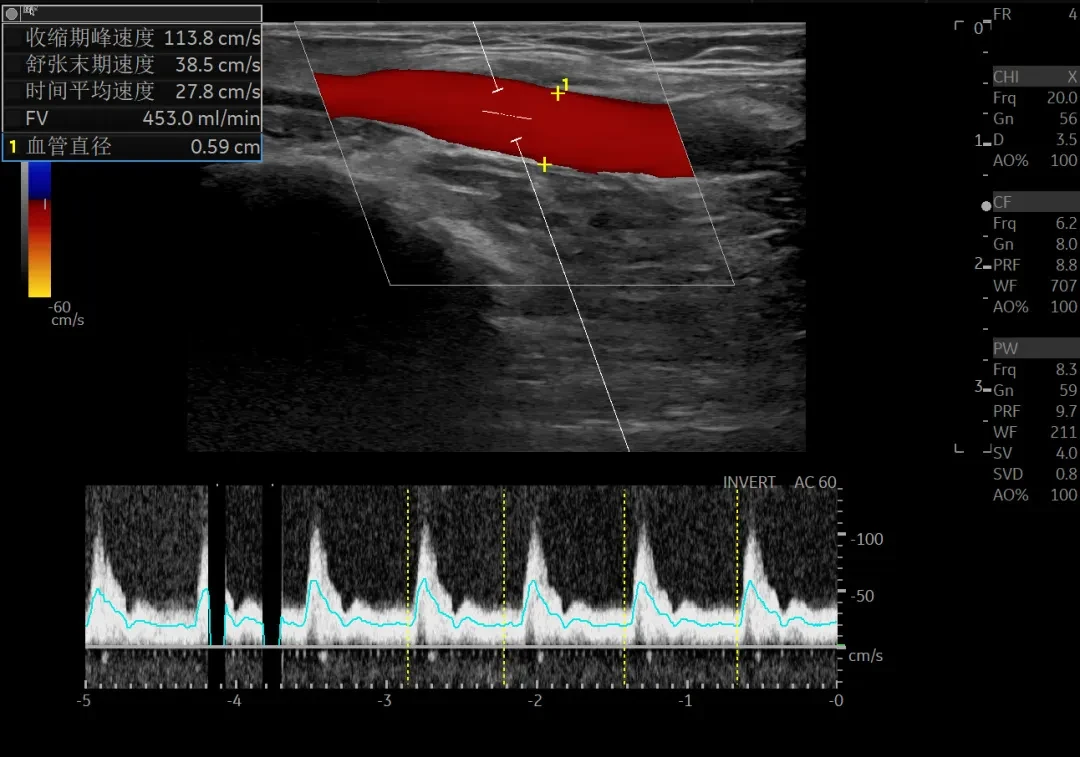
Brachial artery flow 453ml/min.
1. DK Medtech Dissolve® AV High-Pressure Scoring Drug-Coated Balloon7*60mm Aneurysm-like dilation of the proximal segment of the median cubital vein, with a stenotic segment, dilated at 20 atm for 3 minutes, no residual stenosis;
2. The high-pressure balloon Conquest 7*40mm dilated the aneurysm-like dilation at the puncture site of the distal median cubital vein, with pressure gradually increasing from 2 atmospheres to 28 atmospheres.
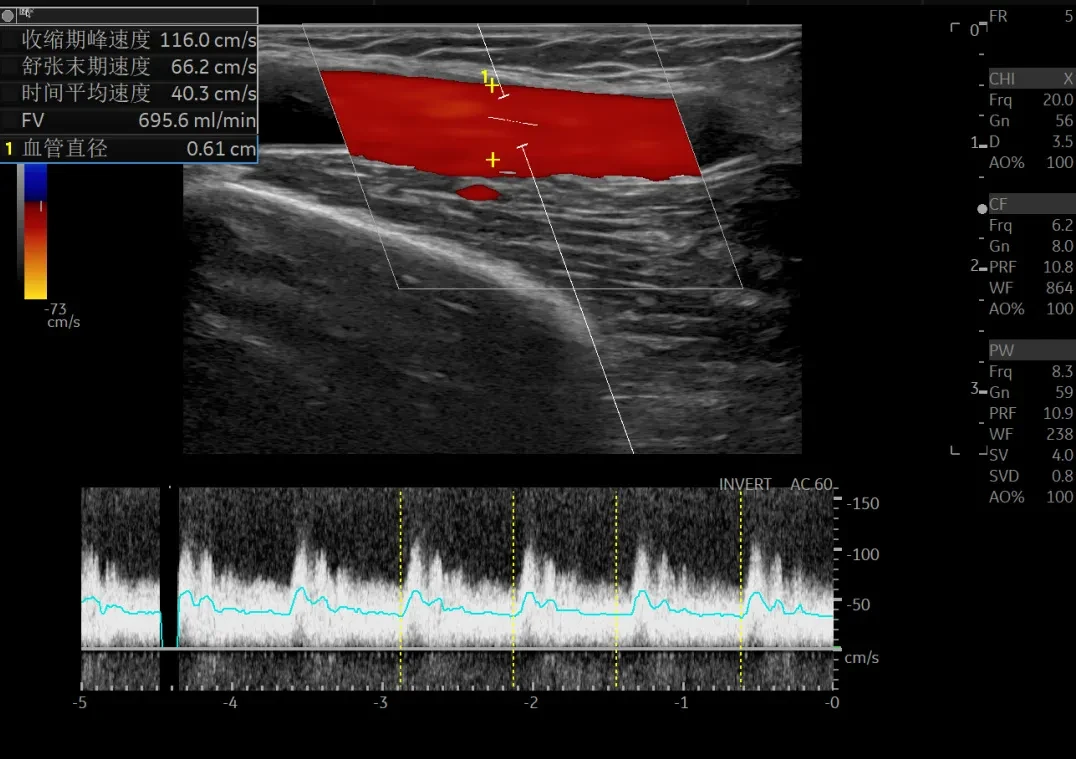
Brachial artery flow 695.6ml/min.
Follow-up
Discharge Status:Currently, the application of internal fistula hemodialysis is proceeding smoothly.
Case Summary
Case Characteristics:The patient's arteriovenous fistula repeatedly thickened, leading to stenosis, and they had undergone multiple dilation surgeries.
Preoperative Assessment Key Points:Preoperative ultrasound carefully evaluates the lesion site, degree of stenosis, nature of stenosis, and blood flow volume of the arteriovenous fistula.
Surgical Strategy/Technical Key Points:
During the operation, the patient's blood flowed retrogradely over the guidewire, entering the stenotic lesion from the vascular dilation. The guidewire was extremely difficult to pass through. Based on the direction of blood flow, the correct position was selected. After continuous random torque control of the guidewire, it successfully passed through the lesion site.
The patient has two areas of stenosis,Considering the significant intimal hyperplasia around the stenotic area of the median cubital vein at the lesion site, and given that this site has previously experienced repeated stenosis and dilation, a scoring drug-coated balloon was chosen for application at this stenotic location.
High-pressure dilation tends to cause vascular rupture; therefore, a scoring balloon is chosen to evenly incise the lesion. During the procedure, care should be taken to avoid vascular injury.
Features/Usage Tips of the Device:Select a scored balloon of appropriate size based on the patient's fistula width. Avoid excessive forceful expansion of the blood vessel, and ensure accurate positioning when using the scored balloon during the procedure.
References:Expert Consensus on Standardized Operating Procedures for Percutaneous Transluminal Angioplasty of Arteriovenous Fistulas Under Ultrasound Guidance (2024).

Introduction of Experts

Professor Zhang Lihong
Director of Nephrology
First Hospital of Hebei Medical University, Chief Physician, Associate Professor, Master's Graduate Supervisor. Director of the Second Department of Nephrology, Director of the Dialysis Access Diagnosis and Treatment Center.
Director of the Vascular Access Health and Care Committee of the Zhongguan Village Kidney Disease and Blood Purification Innovation Alliance;Vice Chairman of the Standards Committee of the Zhongguan Village Kidney Disease and Blood Purification Innovation Alliance;Professional Committee on Peripheral Vascular Diseases of the Chinese Association of Integrative Medicine;Vice Chairman of the Vascular Access Expert Committee;Member of the Professional Committee of the Chinese Hospital Association's Blood Purification Center Management Branch;Member of the Vascular Access Working Group of the Professional Committee of the Chinese Hospital Association's Blood Purification Center Management Branch;Member of the Expert Committee of the Hemodialysis Access Working Group of the Endovascular Specialty Committee of the Chinese Medical Association;Chairman of the Vascular Access and Interventional Nephrology Professional Committee of Hebei Province Vascular Health and Technology Association.

Professor Lin Ruan
Surgeon of This Case
The First Hospital of Hebei Medical University, Associate Chief Physician, Master's Graduate Supervisor, Deputy Director of the Second Department of Nephrology. Completed advanced studies in renal pathology and hemodialysis at the First Hospital of Peking University.
Deputy Chairman of the Vascular Access Health and Care Committee of the Zhongguan Village Kidney Disease and Blood Purification Innovation Alliance;Standing Committee Member of the Vascular Access and Interventional Nephrology Specialty of the Hebei Province Vascular Health and Technology Association;Member of the Hebei Province Integrated Traditional Chinese and Western Medicine Association's Nephrology Professional Committee.
Proficient in the repair of various difficult hemodialysis vascular accesses, as well as the diagnosis and treatment of primary and secondary kidney diseases.

Department Introduction


The Second Department of Nephrology at the First Hospital of Hebei Medical University is a distinctive specialty that integrates medical treatment, scientific research, and teaching.
The department specializes in blood purification and the establishment and maintenance of vascular access, conducting interventional diagnosis and treatment of vascular access with an annual surgical volume exceeding 800 cases. In the past two years, building on its original specialties, it has further developed rich clinical experience in the diagnosis and treatment of complicated and critical renal diseases and peritoneal dialysis management, successfully treating a large number of critically ill patients. It performs various complex vascular access surgeries (e.g., balloon angioplasty of arteriovenous fistulas under ultrasound/DSA guidance, recanalization of central venous occlusion, and artificial vascular arteriovenous fistula surgery), with a technical level that is leading in China.
The department undertakes the teaching tasks for undergraduate and graduate students, with four current master's degree supervisors, two graduated master’s students, and nine master’s students currently enrolled. The department emphasizes the cultivation of talent at all levels. In recent years, through actively organizing academic exchanges and vascular access ultrasound training programs, it has trained more than 100 professional backbone members for the whole of China and the province.
In the past five years, undertook five provincial and ministerial level scientific research projects, published over 60 papers, including 15 SCI papers.

Copyright Statement: This platform aims to help medical and health professionals better understand the latest developments in relevant disease areas. The information content published on this platform does not imply agreement with its descriptions or viewpoints, but is merely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. This information is intended solely for medical and health professionals to stay informed. Such information cannot replace professional medical guidance in any way and should not be regarded as diagnostic or treatment advice. If such information is used for purposes other than staying informed, this platform and its authors assume no related responsibility.Contact email for cooperation:vascular@edoctor.work。
