Another Tumor on the Brink of Cure? Strong Clinical Data for Tecvayli plus Darzalex in Relapsed/Refractory Multiple Myeloma

Johnson & Johnson
Medical Device R&D and Manufacturer

© Amino Observation - Innovative Drug Team Original Production
Author | Shawei Sha
In the long journey of fighting cancer, "cure" has always been the ultimate goal pursued by both doctors and patients. However, in most cancer types, long-term survival has become the alternative measure of "cancer cure" due to recurrence, drug resistance, and the ceiling of treatment efficacy.
However, with the advent of targeted therapy, immunotherapy, and cell therapy, some tumors have begun to approach the boundary of being cured. For hematological tumors such as Hodgkin's lymphoma and leukemia, progression-free survival periods of 5 years or even 10 years have been observed.
A recent clinical study in relapsed/refractory multiple myeloma (RRMM) has brought the goal of a cure even closer: On December 29, at the ASH conference, Johnson & Johnson presented the phase 3 clinical results of the BCMA/CD3 bispecific antibody TECVAYLI combined with the CD38 monoclonal antibody DARZALEX as a second-line treatment for RRMM patients. Compared to standard treatment, the combination therapy group achieved a 36-month PFS rate of 83.4%, with a hazard ratio (HR) of 0.17.
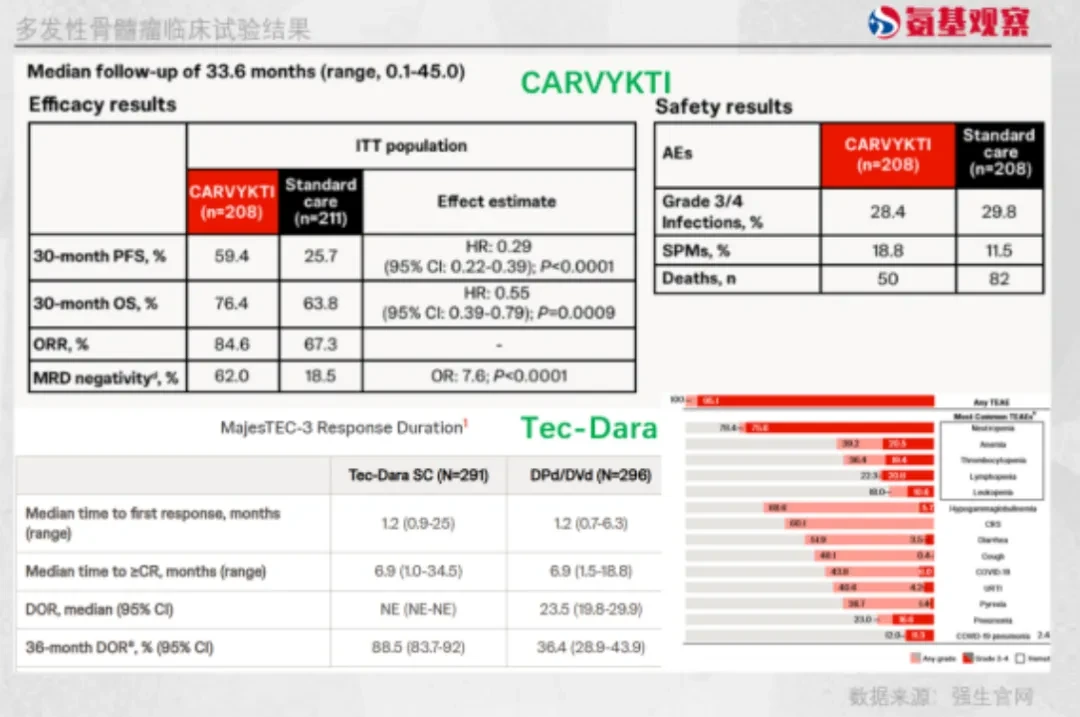
In a long-term follow-up prior to this, the CAR-T therapy CARVYKTI, developed by Legend Biotech/Johnson & Johnson for RRMM, achieved ≥5 years of progression-free survival in 33% of patients.
For blood tumors long considered "highly recurrent and difficult to cure," multiple drugs have demonstrated lasting and stable survival benefits. Tecvayli+Darzalex, in particular, has shown significant survival benefits, further raising the efficacy ceiling for RRMM treatment. Does this mean the "cure" era for multiple myeloma has arrived?
/ 01 /
"One Step Closer to the Ultimate Cure"
Data from the American Cancer Society (ACS) shows that by 2025, nearly 70% of cancer patients in the United States will survive five years or more after diagnosis, with 49% surviving 10 years or more and 22% surviving 20 years or more.
However, multiple myeloma (MM), the second most common blood cancer globally, has a 5-year survival rate of less than 60%, due to drug resistance and recurrence.
The emergence of CAR-T therapy has brought new hope to patients with RRMM. Currently, two approved CAR-T therapies, Abecma and Carvykti, both target BCMA, with Carvykti showing superiority in ORR and OS compared to the former. Although CAR-T is effective for some RRMM patients, relapse remains inevitable, and the single-target BCMA is susceptible to antigen escape.
To address this challenge, Johnson & Johnson has proposed a strategy to upgrade innovative treatment models: achieving mechanism complementarity through the combined application of Tecvayli and Darzalex.
Tecvayli, as a BCMA/CD3 bispecific antibody, targets the BCMA antigen on the surface of MM cells at one end and binds to the CD3 molecule on the surface of T cells at the other end, rapidly activating T cells to kill tumor cells; whereas the CD38 monoclonal antibody Darzalex not only directly kills CD38-positive MM cells but also eliminates immunosuppressive cells, improving the tumor microenvironment.
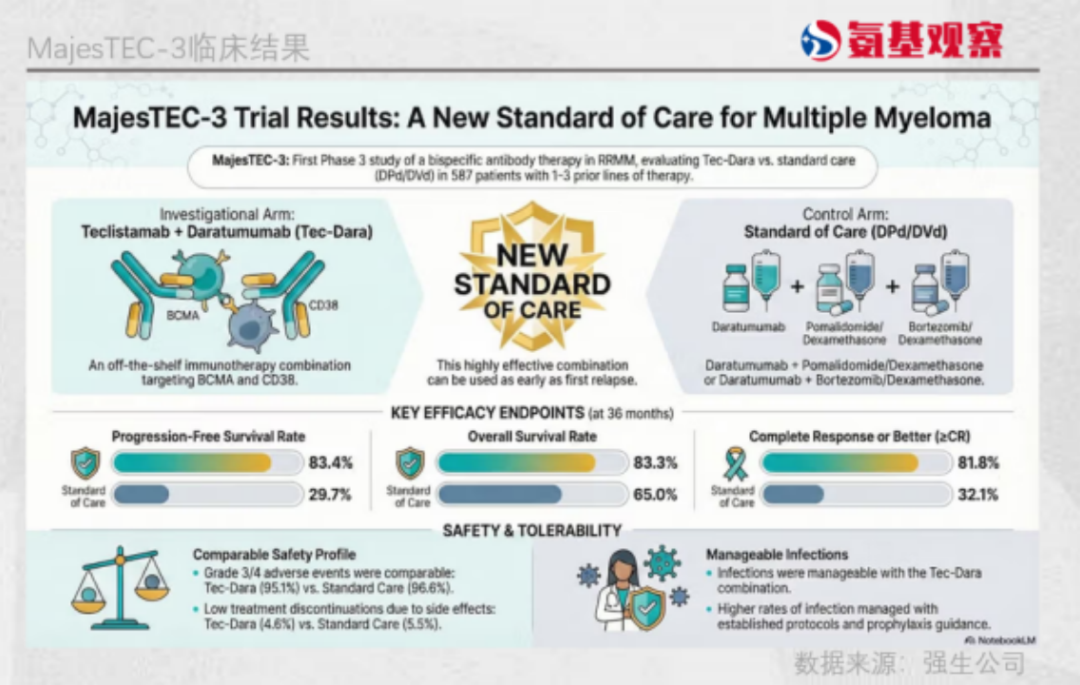
Latest Clinical Outcomes Validate the Success of This Strategy: The Tecvayli+Darzalex Combination Demonstrates Greater Advantages in Survival Metrics. Compared with Carvykti Treatment CARTITUDE-4 Study Data: In terms of survival benefits, the 36-month OS rate for the Tecvayli+Darzalex group was 83.3%, surpassing Carvykti's 76.4%; the durability of progression-free survival showed an even more pronounced advantage, with the combination group achieving a 36-month PFS of 83.4%, while Carvykti’s 30-month PFS was 59.4%.
Currently, the Tecvayli+Darzalex combination therapy group has been granted Breakthrough Therapy Designation by the U.S. FDA, and Johnson & Johnson has submitted an application for market approval.
It should be noted that both drugs have accumulated sufficient clinical validation in the treatment of MM. Tecvayli was approved by the FDA in 2022 for fourth-line treatment of MM and is even approved for third-line treatment in Europe, with its single-agent efficacy having been confirmed in heavily pretreated, relapsed MM patients. Darzalex has been approved for 11 indications across multiple treatment stages, ranging from first-line to later lines, in MM.
Sen Zhuang, M.D., of the Johnson & Johnson Innovative Medicine Oncology Clinical Center, stated: "With this data, we are entering a new era in the treatment of multiple myeloma. By combining other transformative therapies from our leading portfolio, we can provide optimal outcomes for patients at any stage of the disease, bringing us one step closer to our ultimate goal of a cure."
At the same time, although Carvykti and the combination therapy are in competition, Mark Wildgust, Vice President of Global Medical Affairs at Johnson & Johnson, said at a briefing before the ASH conference: "Both provide the same chance of a cure." He also added: "Carvykti requires only one treatment to complete the course, while Tecvayli-Darzalex is more suitable for patients who are unwilling or unable to travel to a CAR-T treatment center, as it will be available in a community setting. In the United States, Carvykti is available at only 128 sites, whereas there are over 5,000 medical centers using Darzalex."
Obviously, a new round of competition has unfolded around market penetration, but in any case, the trend toward more accessible treatments for RRMM is already emerging.
/ 02 /
Another "Cured" Hematoma
The breakthrough brought by Tecvayli+Darzalex represents another step forward in the overall trend towards a "cure" for hematological tumors.
Previously, Hodgkin's lymphoma has achieved a long-term remission rate of 80-90% through classical chemotherapy regimens and immunotherapy. Even for advanced-stage patients, more than half can achieve long-term survival, making it the tumor with the highest "cure rate" among hematological malignancies.
Ph+ acute lymphoblastic leukemia (ALL) is a typical example of a once fatal disease evolving into a curable cancer. Before 2000, the long-term survival rate of Ph+ ALL was less than 10%. The introduction of the first-generation TKI, imatinib, enabled 60% of relapsed patients to achieve complete remission. In the latest D-ALBA study, patients who achieved complete molecular remission (CMR) with the "immunotherapy + targeted therapy" combination of ponatinib and blinatumomab reached a 4-year disease-free survival rate of 100%.
Although the long-term survival outcomes of Tecvayli+Darzalex in RRMM are not as favorable as those for the aforementioned indications, this is undoubtedly a groundbreaking advancement in RRMM, a tumor characterized by high long-term recurrence rates and strong drug resistance.
From targeted therapy and CAR-T to Tecvayli + Darzalex, the advancements in treatment strategies and mechanisms for RRMM have become a hallmark of the current era of cancer cures.
Compared with hematologic tumors, solid tumors are associated with high heterogeneity and the influence of a complex tumor microenvironment, which prevents cell therapies from demonstrating their clearance capabilities in solid tumors. However, targeted drugs such as EGFR and ALK inhibitors have achieved precise interventions for solid tumors.
Pfizer's third-generation ALK inhibitor, lorlatinib, achieved a 5-year progression-free survival rate in 60% of participants with previously untreated ALK-positive advanced NSCLC; the long-term survival curve for some patients has even approached that of a chronic disease trajectory. Additionally, for early-stage EGFR-mutated NSCLC, first-line treatment with osimertinib enabled some patients to achieve more than 5 years of progression-free survival.
The emergence of immunotherapy has further brought new hope to some solid tumors, such as melanoma. In a clinical trial (CheckMate 067 III) of nivolumab combined with ipilimumab for the treatment of advanced melanoma, sustained survival benefits were observed in the follow-up results, with a median OS reaching 71.9 months.
Although the cure of solid tumors mostly occurs in the early localized stage, surgery, chemotherapy, targeted drugs, immunotherapy, and combination strategies are also driving solid tumors towards a "cure."
"Within five years, cancer will be removed from the list of fatal diseases." This was the optimistic promise made to U.S. President William Howard Taft by laboratory staff during his 1910 visit to the Roswell Park Comprehensive Cancer Center. More than a century has passed, and while cancer has not been completely conquered, the era of cures has arrived.
/ 03 /
The Advent of the Era of Tumor Cure
From "Cancerophobia" to "Scientific Cancer Fighting", tumors are shifting towards a form that can be controlled over the long term, and even achieve functional cure in certain populations. The advent of the "Cure Era" for cancer is not the result of a single drug or a particular clinical breakthrough, but rather the outcome of technological maturity and synchronized upgrades in industry understanding.
Technological leaps serve as the underlying driving force. The completion of the Human Genome Sequencing in 2003 marked a significant turning point in the logic of cancer treatment. Gene sequencing has facilitated early detection and biomarker stratification, transforming cancer from a homogeneous disease into a more nuanced condition; personalized medicine has further expanded treatment options for cancer, including surgery, radiotherapy, immunotherapy, targeted therapy, and gene editing, significantly improving patient survival rates and quality of life.
When "cure" becomes possible, the design logic of pharmaceutical companies' clinical pipelines shifts from "unmet needs" to "a comprehensive layout with the goal of cure."
A typical example is Johnson & Johnson's investment and layout in the MM field: previously approved drugs include Darzalex, Carvykti, and Tecvayli, with subsequent advancements such as KLN-1010 (in vivo CAR-T) and JNJ-5322, a BCMA/GPRC5D/CD3 trispecific antibody, aiming to achieve comprehensive cure for MM.
Of course, Johnson & Johnson's pipeline layout is not entirely based on the development of innovative drugs with cutting-edge mechanisms; it also includes drug upgrades that are based on expert consensus and can be quickly realized. This is why Johnson & Johnson was the first to upgrade the Tecvayli+Darzalex combination and rapidly advance it to the market stage.
It needs to be clear that "cure" does not mean an absolute "never relapse," but rather a long-term health condition that is assessable and acceptable.
From "prolonging survival" in the era of chemotherapy to "precision strikes" in targeted therapy, then to "spontaneous attacks" in immunotherapy, and the "regenerative mechanism" introduced by cell therapy, all are bringing humanity closer to curing cancer.
Looking forward to more and more cancers welcoming the era of cure under the advancement of scientific innovation.
PS: Welcome to scan the QR code below to add the WeChat ID of Anji Jun for communication.
