Professor Zhou Zhongxin's Team Showcases DKutting® Directional Scoring Balloon for Improved AVF Patency

DK Medtech
Vascular Interventional Balloon Product Developer

With the vigorous development of China's peripheral vascular intervention market, common balloons tend to cause complications such as excessive vascular injury, flow-limiting dissections, and hematomas when addressing the increasing number of highly resistant stenotic lesions. In contrast, pressure-focusing balloons utilize cutting/notching components positioned between the inner wall of the blood vessel and the outer diameter of the balloon during expansion. These components enhance localized pressure, enabling efficient directional expansion, thereby reducing vascular elastic recoil and representing a new direction in the evolution of vascular intervention balloons.
DK Medtech's Self-Developed DKutting® Directional Scoring Balloon, featuring an exclusive patented design (CN201810478242.X), utilizes nickel-titanium coiled scoring elements. It offers numerous advantages such as excellent trackability, uniform expansion, high burst pressure, and directional cutting. The upgraded product provides "top-tier expansion" treatment outcomes for vascular stenosis lesions. This marks a significant breakthrough for local enterprises in innovating and surpassing top imported products.
DK Medtech Special Release[Professor Zhongxin Zhou's Team: Directional Notched Balloon Facilitates AVF Patency] Case Presentation, demonstrating the meticulous operation of each case and the clinical application of advanced equipment and instruments. From the formulation of treatment strategies for different cases, standardized intraoperative procedures and technical applications, complication prevention, to perioperative management, etc., the aim is to promote the standardization of diagnosis and treatment for vascular stenosis and occlusive diseases, enhance technical exchange and experience sharing among doctors, with the hope of providing new ideas and methods for future diagnosis and treatment, benefiting more clinical patients.
Patient Information
Basic Information:Underwent hemodialysis for 3 years, and established an arteriovenous fistula in the left forearm in early 2022.
Chief Complaint:Severe stenosis of the arteriovenous fistula in the left upper limb found 1 day ago (admitted on 2025-9-3).
History of Present Illness:Due to arteriovenous fistula stenosis, the patient requires a fistuloplasty (PTA) every six months at the local hospital. The most recent PTA was performed in May this year, but postoperative improvement in fistula blood flow was suboptimal. One day prior, the patient noticed weak thrill in the left forearm arteriovenous fistula with only faint vascular pulsation, which could not meet dialysis requirements. The patient came to our hospital for further treatment.
Past Medical History:Generally in poor health, with a history of diabetes for over 30 years, currently undergoing regular treatment with NovoRapid 30 insulin injections (26u before each meal), but with suboptimal blood glucose control. History of hypertension for over 30 years, with the highest recorded blood pressure exceeding 200 mmHg; no regular use of antihypertensive medications or blood pressure monitoring. Surgical history: underwent left forearm arteriovenous fistula surgery at a local hospital in 2022.
Physical Examination:The thrill of the arteriovenous fistula in the left forearm is weak, with only faint vascular pulsation palpable.
Admission Diagnosis:Stenosis of Arteriovenous Fistula:Color Doppler ultrasound indicates extremely severe stenosis of the cephalic vein in the left forearm (Type Ib stenosis of arteriovenous fistula), with underdeveloped cephalic vein in the upper arm (diameter approximately 3mm). The fistula blood flow mainly returns through the median cubital vein and basilic vein. The vascular condition of the contralateral right forearm is poor, with multiple plaques in the radial artery and luminal stenosis; the maximum diameter is about 1.6mm, and the diameter of the cephalic vein after arm constriction is approximately 2mm. The vessels in the right forearm do not meet the conditions for fistula creation.
Previous interventional treatment
Time | Main Treatment Process |
Early 2022 | A temporary dialysis catheter was inserted into the right neck to start hemodialysis, followed by an autologous arteriovenous fistula surgery on the left forearm. After the fistula matured, the temporary dialysis catheter was removed, and regular hemodialysis has been ongoing since then. |
December 2023 | Stenosis of Arteriovenous Fistula in Left Forearm, PTA Performed |
June 2024 | Stenosis of Arteriovenous Fistula in Left Forearm, Treated with PTA |
December 2024 | Stenosis of Arteriovenous Fistula in Left Forearm, PTA Performed |
May 2025 | Left forearm arteriovenous fistula stenosis underwent PTA. Postoperative improvement of fistula blood flow was not ideal. One day ago, the patient noticed weak thrill in the left forearm arteriovenous fistula, with only faint vascular pulsation detectable, insufficient for dialysis. |
Preoperative Analysis
Preoperative Analysis:Preoperative physical examination and color Doppler ultrasound evaluation suggest elastic recoil of the venous anastomosis leading to stenosis. Based on theoretical knowledge, this is likely due to severe intimal hyperplasia.
Surgical Objective:
Main Objectives:Dilate the venous anastomosis to restore normal venous pressure and meet the requirements for dialysis;
Secondary Objective:Prolong AVF service life, fewer complications, fewer interventions.
Surgical Strategy/Plan:Balloon dilation under DSA guidance.
Equipment Preparation:
DKutting®Directional Scoring Balloon
DK Medtech Peripheral Balloon 5*40mm
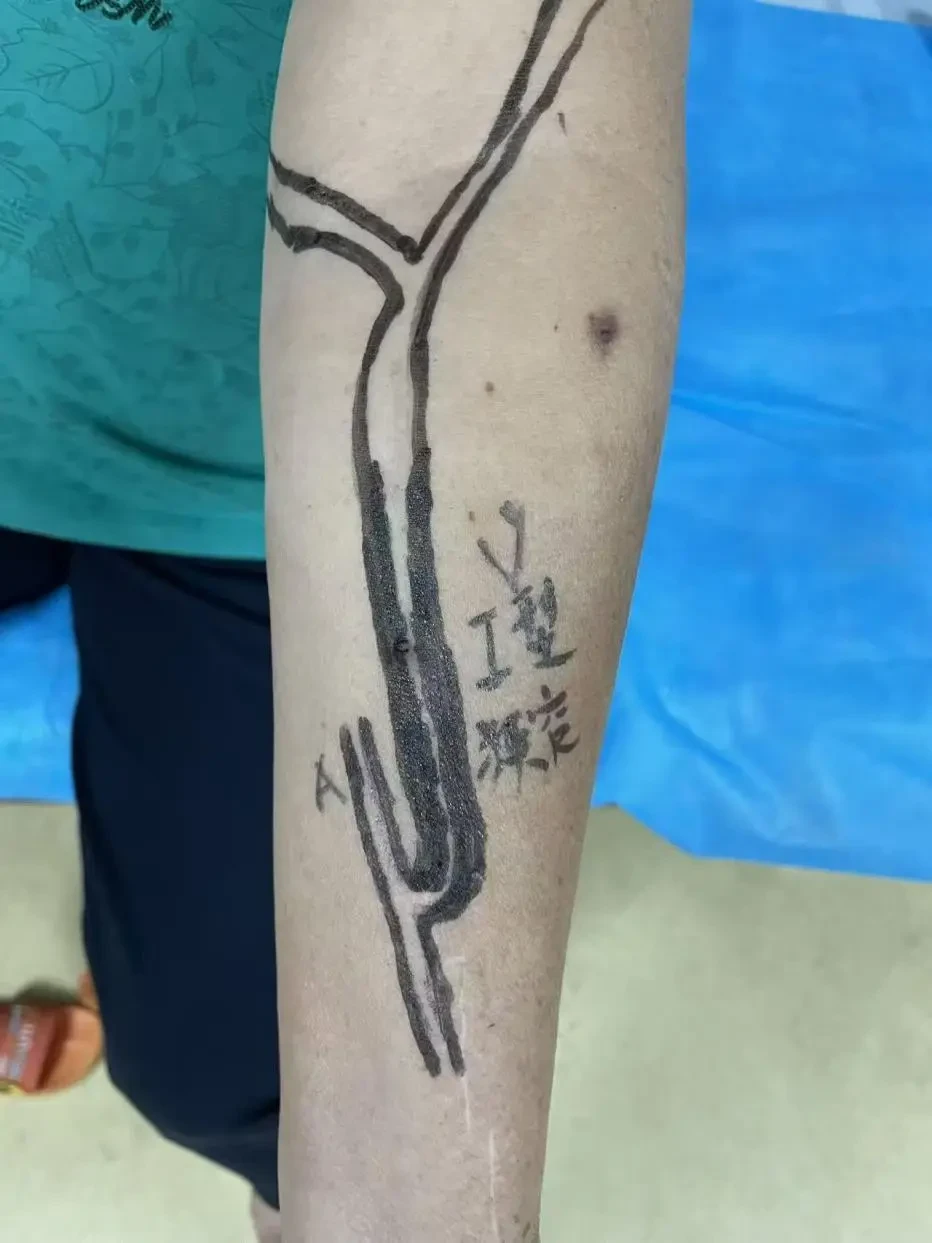
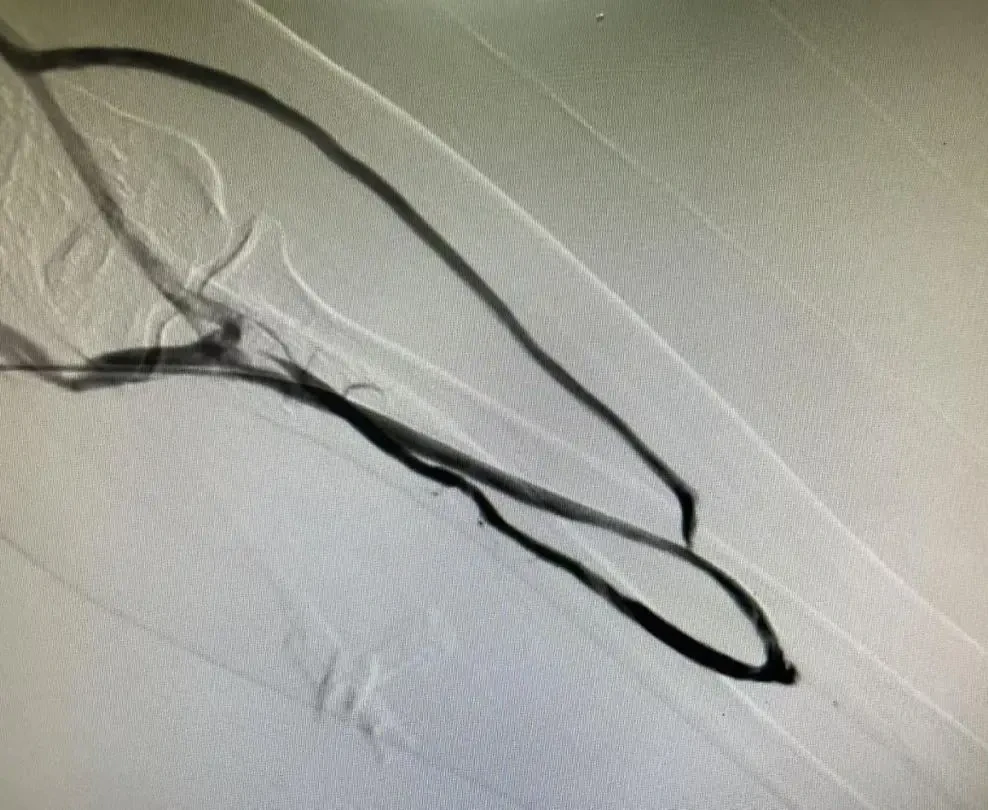
Preoperative Imaging
Surgical Procedure
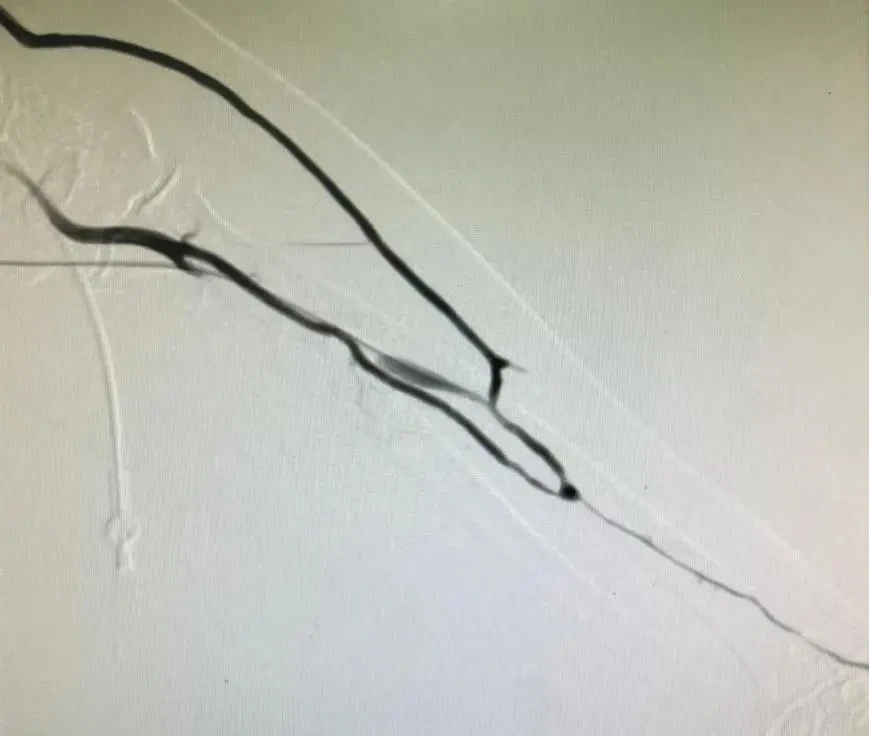
Through the cephalic vein of the forearm, the anastomosis of the internal fistula enters the brachial artery of the upper arm. Angiography through the catheter shows severe stenosis at the anastomosis and the cephalic vein proximal to the anastomosis. First, introduce4mmx40mm DK Medtech Directional Scoring Balloon(DKT35-4040A) Dilate the anastomosis and the stenotic segment of the cephalic vein. After dilation, repeat angiography shows improved blood flow in the cephalic vein compared to before, but local lumen narrowing is still observed.

A 5*40mm standard balloon was then introduced to dilate the stenotic segment of the cephalic vein again until the stenosis was completely resolved.
Follow-up angiography showed a significant increase in the blood flow velocity of the arteriovenous fistula, with the lumen of the previously narrowed segment widened compared to before. Palpation revealed a marked thrill in the forearm fistula.
Follow-up
Discharge Status:
Postoperative thrill of the patient's arteriovenous fistula significantly increased, and dialysis through the left forearm arteriovenous fistula was successfully performed immediately after the surgery.
Follow-up by telephone on December 16, 2025, after discharge: Currently undergoing regular dialysis through an autologous arteriovenous fistula with good blood flow during dialysis.
Case Summary
Case Characteristics:Severe stenosis of the reflux cephalic vein in the left forearm (Type Ib arteriovenous fistula stenosis).
Preoperative Assessment Key Points:The patient has been using AVF for over 3 years, with recurrent stenosis occurring in the past six months. The cephalic vein in the upper arm is underdeveloped (diameter approximately 3mm), and the main blood flow of the fistula returns via the median cubital vein and basilic vein. The contralateral arm shows poor condition of the arteriovenous vessels in the right forearm, with multiple plaques in the radial artery and luminal stenosis; the maximum diameter is about 1.6mm, and the diameter of the cephalic vein after cuffing is approximately 2mm.
Surgical Strategy/Technical Key Points:The patient is a long-term diabetic with poor vascular condition, so a balloon with higher expansion efficiency is needed to achieve safe and effective dilation. A 4mm directional scoring balloon will be used first, followed by a 5mm regular peripheral balloon.
Device Features/Usage Tips:Achieved using a directional scoring balloonDirectional intimal tearing ensures better lumen gain while reducing elastic recoil.
Effectiveness Evaluation:Postoperative Enhancement of Internal Fistula Thrill and Successful Dialysis via Left Forearm Arteriovenous Fistula

Expert Introduction


Professor Zhongxin Zhou
Director of Interventional Vascular Surgery
Director of the Department of Interventional Vascular Surgery, First Affiliated Hospital of Guangzhou University of Chinese Medicine, Medical Doctor, Chief Physician, Master's Supervisor;Chairman of the Peripheral Vascular Disease Committee of the Guangdong Provincial Traditional Chinese Medicine Association;Chairman of the Vascular Access Special Committee of the Guangdong Grassroots Medical Association;Vice Chairman of the Vascular Surgery Committee of the Guangdong Provincial Clinical Medical Association;Vice Chairman of the Vascular Surgery Branch of the Guangdong Health Association;Standing Committee Member of the Vascular Surgery Branch of the Guangdong Medical Association.

Professor Wang Xun
Surgeon of This Case
Associate Chief Physician, Department of Interventional Vascular Surgery, First Affiliated Hospital of Guangzhou University of Chinese Medicine; Medical Doctor;Youth Committee Member of the Interventional Medicine Branch of the Guangdong Medical Association;The Second Standing Committee Member of the Interventional Professional Committee of Guangdong Medical Education Association;Standing Committee Member of the First and Second Sessions of the China Pediatric Intervention Alliance;Youth Committee Member of the Interventional Specialty Committee of Guangzhou Medical Association;Member of the First Committee of the Precision Intervention Branch of the Guangdong Provincial Society for Precision Medicine Application;Member of the Second Interventional Medicine Professional Committee of Guangdong Provincial Hospital Association.

Xiao Weiliang Professor
The Surgeon of This Case
Attending Physician at the First Affiliated Hospital of Guangzhou University of Chinese Medicine.
Participate in the clinical teaching of interventional radiology and integrated traditional Chinese and Western medicine surgery, specializing in interventional and vascular surgeries such as thoracoabdominal aortic aneurysms, aortic dissections, lower extremity arterial sclerosis occlusion, deep vein thrombosis of the lower extremities, varicose veins of the lower extremities, and liver cancer.

Department Introduction


The predecessor of the Interventional Vascular Surgery Department at the First Affiliated Hospital of Guangzhou University of Chinese Medicine, the Interventional Suite, was established in 1995. An interventional outpatient service was introduced in 2017, and in August 2023, the department expanded to become the Interventional Vascular Surgery Department, with 43 beds. It has developed into a relatively comprehensive clinical department integrating medical treatment, research, and teaching, focusing on minimally invasive vascular surgery and tumor intervention. Over the past 30 years, the department has carried out numerous minimally invasive interventional and vascular surgical diagnostic and therapeutic procedures across various parts of the body, with an annual average of over 2,000 surgeries.
The department currently has more than twenty healthcare professionals and technical personnel, equipped with internationally advanced diagnostic and treatment technologies as well as extensive clinical experience. Among the physician team, there are 2 chief physicians, 1 deputy chief physician, 3 attending physicians, 2 resident physicians, and several graduate students in training. In the past three years, this specialty has led and undertaken 1 provincial-level research project, 3 research projects from the Guangdong Provincial Administration of Traditional Chinese Medicine, and relevant academic achievements have been widely applied and promoted in clinical practice.
Zhou Zhongxin, Director, Professor, Chief Physician, and Master's Supervisor, is a leading figure in the field. He specializes in hybrid surgery for aortic aneurysms/aortic dissections, interventional treatment of tumors, varicose veins of the lower extremities, carotid artery diseases, and critical complications related to vascular access in uremic patients.
Copyright Statement: This platform aims to help healthcare professionals better understand the latest developments in relevant disease areas. The information published on this platform does not imply agreement with its descriptions or viewpoints; it is solely for providing more information. If there are any copyright issues, we kindly request the rights holders to contact us, and we will address them as soon as possible. The information is intended for healthcare professionals to stay informed and should not replace professional medical guidance in any way, nor should it be considered as medical advice. If such information is used for purposes other than staying informed, this platform and the author assume no responsibility.Contact Email for Cooperation:vascular@edoctor.work。
