Immunocore Announces Orphan Drug Designation for IMCgp100 and Collaboration with AstraZeneca on Combination Therapy for Metastatic Melanoma
For a long time, cancer, as an incurable disease, has posed a major challenge to human health. Traditional immunotherapies, such as surgical tumor resection, radiation therapy, chemotherapy, or other combination therapies, lack effective targeting of specific antigen-antibody interactions.

Image from Immunocore
Immunocore focuses on the development of TCR-based targeted therapies, with its lead product, IMCgp100, receiving orphan drug designation from the FDA in 2016.
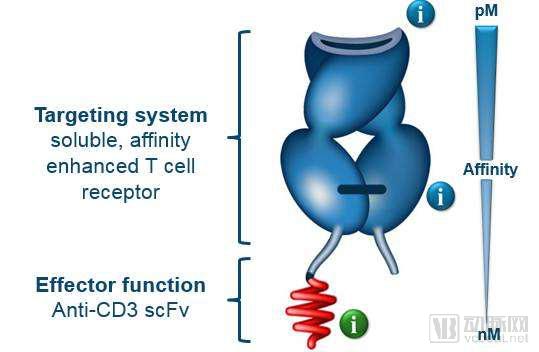
Immunocore’s core technology, known as ImmTAC, is a novel bispecific biologic composed of an engineered T cell receptor (TCR) and an anti-CD3 single-chain variable fragment (scFv). This molecule exhibits high tumor-targeting specificity.
TCRs can recognize intracellular antigens that are processed and presented on the cell surface as peptide-HLA complexes (pHLA). The affinity of TCRs is approximately nine-fold higher than that of conventional antigen-antibody interactions. The CD3 scFv binds to T cells, with ImmTAC serving as a bridge between the two. Upon binding, T cells can specifically eliminate target antigens.
ImmTAC Molecules
The unique and potent mechanism of ImmTAC molecules enables them to address various types of solid tumors.
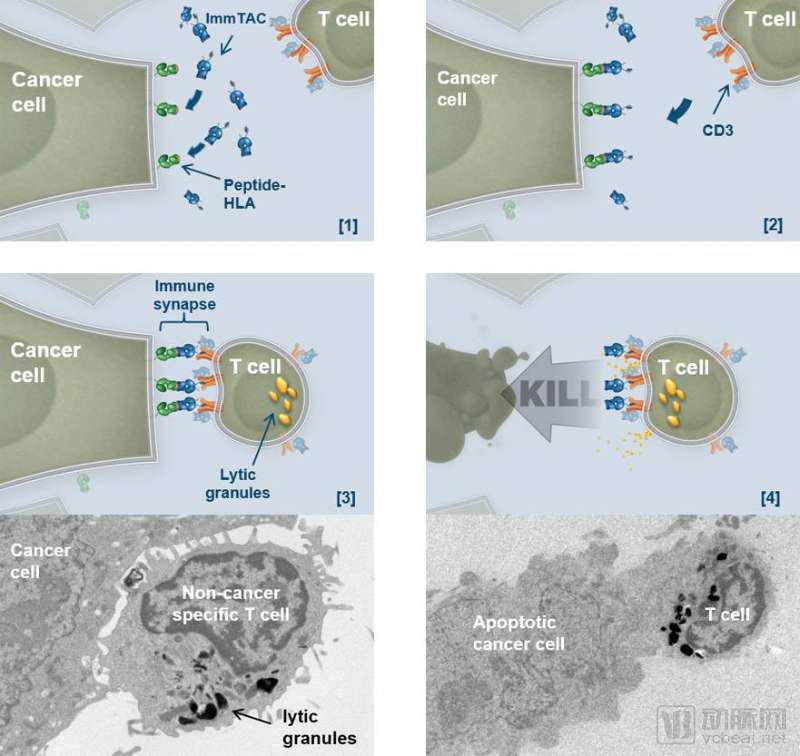
Schematic Diagram of ImmTAC-Mediated Tumor Cell Killing
Moreover, ImmTAC molecules are relatively low-cost, can be mass-produced in bacterial systems, and have a shelf life of up to several years.
Currently, Immunocore’s lead product, imcgp100, features an engineered T-cell receptor that targets the gp100 peptide antigen presented by HLA-A2 on the surface of melanoma cells, exhibiting extremely high affinity. This product has currently entered Phase IIa clinical trials.
In contrast, other types of bispecific antibodies have shown suboptimal clinical performance to date, largely due to their high pricing and short half-lives.
Amgen’s platform is called the BiTE platform, and Blincyto, based on this platform, was approved for market launch in 2012. This drug is primarily used to treat acute lymphoblastic leukemia (ALL). The bispecific antibody developed using this technology can bind to T cells and tumor cells via CD3 and CD19, respectively. It recruits and activates T cells through CD3, thereby killing tumor cells.
However, data from Phase II clinical trials showed that only 43% of patients achieved partial or complete remission after two cycles of Blincyto treatment.
Roche’s CrossMab technology achieves its objective through the exchange of Fab arm domains in bispecific IgG antibodies, while correct heavy-chain pairing can be accomplished using the KiH and electrostatic steering technologies.
This platform can construct bispecific antibodies in various formats, but it has significant drawbacks, including the generation of multiple by-products, which hinders industrial-scale manufacturing. Its product, CEA-TCB, exhibits low efficacy as a monotherapy, with a disease response rate of only 6%; however, when combined with tecentriq, the disease response rate improves to 18%.
ImmTAC technology is primarily used for the treatment of solid tumors, either as monotherapy or in combination with other agents. Beyond oncology, ImmTAC holds promise for future applications in the treatment of infectious diseases and autoimmune disorders.
Immunocore has announced the initiation of a Phase Ib/II clinical study in collaboration with MedImmune, an AstraZeneca company, to evaluate the safety and efficacy of IMCgp100 in combination with durvalumab and tremelimumab for the treatment of metastatic cutaneous melanoma.
It is reported that this open-label, four-arm controlled trial will evaluate the efficacy of IMCgp100 plus durvalumab, IMCgp100 plus tremelimumab, and the combination of all three immunotherapies.
Leveraging its ImmTACs technology, Immunocore has established extensive collaborations with Roche, GlaxoSmithKline, and Eli Lilly.
Dr. Lundberg, President of Lilly Research Laboratories, commented, “The primary goal and challenge of cancer immunotherapy drugs is to direct the immune system to recognize and destroy cancer. I believe Immunocore’s ImmTAC platform has the potential to achieve this.”
Immunocore, which spun off from Germany’s Medigene AG in 2008, has secured a total of $360 million in investment to date, most recently raising $40 million in Series B financing from the Bill & Melinda Gates Foundation.
Bent Jakobsen, the company’s founder, currently serves as Chief Scientific Officer and a member of the Executive Board. He is also one of the founders of Adaptimmune. Previously, Jakobsen served as Chief Scientific Officer at Avidex, where he led the development of T-cell receptor-based therapeutics, and he is an expert in the field of T-cell receptor immunology.
Nicholas Cross served as Executive Director of Avidex from 2000 to 2006, and subsequently as Chairman of Immunocore from 2008 to 2013. He is a serial entrepreneur and investor, holding a Bachelor of Arts degree from the University of Oxford and an MBA from London Business School.
Ian Laing is a founding shareholder of Immunocore. Over the past 25 years, he has primarily invested in life sciences and technology companies. He holds a master’s degree from the University of Oxford and an MBA from London Business School.
George Robinson has served as a Non-Executive Director of Immunocore since 2008. He co-founded the investment management firm Sloane Robinson LLP in 1993 and is a member of the Investment Committee of the University of Oxford Endowment Fund.
Competitor: Adaptimmune
Immunocore currently has a budgeted revenue of $22.7 million and has raised $360 million in financing. Its sister unicorn company, Adaptimmune, currently has a budgeted revenue of $43.2 million and has raised $149 million in financing.
As Immunocore’s biggest competitor in the TCR technology field, Adaptimmune’s experts bring 15 years of research experience in immuno-oncology and T-cell receptors. Its proprietary SPEAR T-cell platform enables the engineering of T cells to target and destroy a wide range of tumors.
The company’s four independently developed classes of anticancer drugs have entered the clinical trial stage for the treatment of various tumors, including non-small cell lung cancer, melanoma, bladder cancer, and head and neck tumors. In addition, NY-ESO TCR, jointly developed by Adaptimmune and GSK, has also entered clinical trials.
Meanwhile, Immunocore’s current pipeline indicates that most of its drug candidates are in the preclinical research stage.
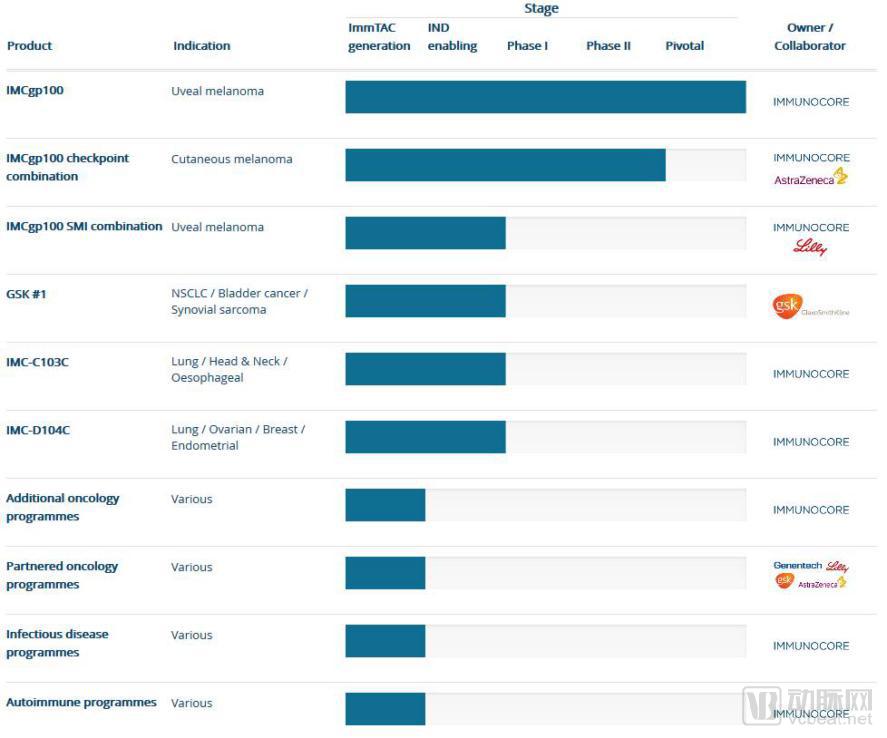
Immunocore's R&D Pipeline
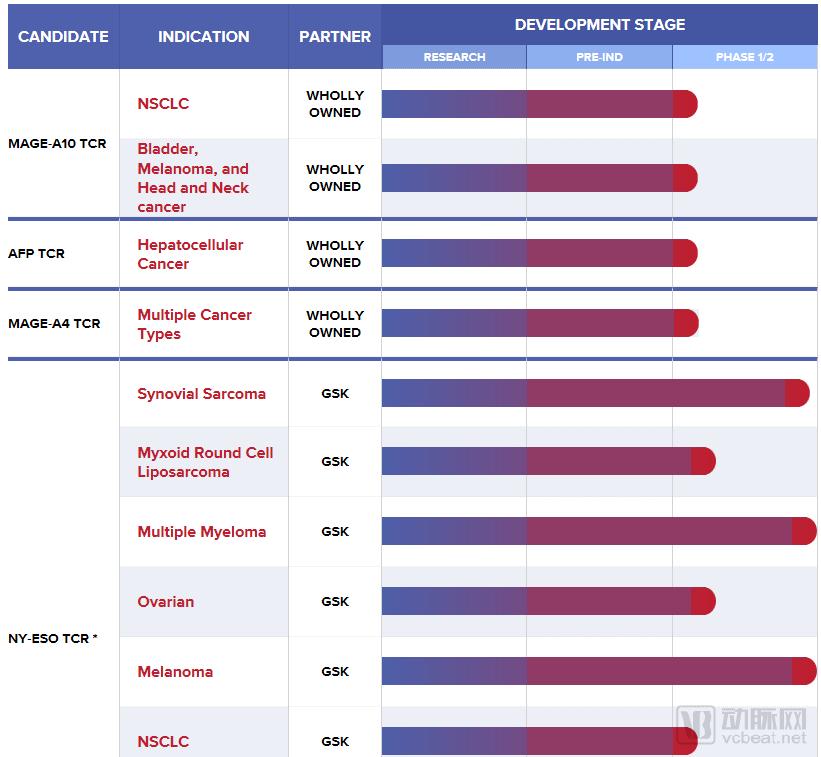
Adaptimmune's R&D Pipeline
Compared with Adaptimmune, ImmunoCore has a slower pace in clinical research and stronger product specificity; whereas most of Adaptimmune’s products can be used for the treatment of various tumors, with a broader range of indications.
Competitor: Medigene
Medigene aims to create breakthrough therapies to improve the lives of cancer patients, with a budgeted revenue of $13.6 million. Its core technologies primarily fall into three categories: TCR-Ts, DCs, and TABS.
TCR-T therapy involves the specific modification of T cells isolated from the human body, which are then reinfused to generate CD4+ and CD8+ T cells for the targeted elimination of various tumor cells.
The DCS platform is a vaccine produced by the company that stimulates the human immune system to eliminate tumor cells. Currently, this vaccine demonstrates excellent therapeutic efficacy in patients with minimal residual disease, such as those with a small number of remaining tumor cells after surgical resection, radiation therapy, or chemotherapy. At present, the vaccine is primarily used for the treatment of acute myeloid leukemia.
TABS therapy is designed to target pathogenic T cells, capable of identifying and distinguishing between normal and pathogenic T cells, ultimately eliminating the latter. This therapy is primarily used for autoimmune diseases.
Currently, Medigene has five main drug candidates, but only its DCs antibody has entered Phase II clinical trials. Compared with Immunocore, Medigene’s various clinical studies are progressing more slowly, as the company focuses more on the development of personalized T-cell immunotherapies.
In 2013, Science magazine ranked cancer immunotherapy as the top breakthrough among its Top 10 Scientific Breakthroughs. Immunocore, with its core technology ImmTAC, is a leader in cancer immunotherapy.
Other immunotherapies, such as PD-1 inhibitors, PD-L1 inhibitors, CAR-T cell therapy, and biological therapies, have attracted widespread attention in the field of cancer treatment; however, the current outlook for anticancer therapy remains less than optimistic. Following the “Wei Zexi incident,” DC-CIK therapy came under public scrutiny and intense media focus.
The National Health and Family Planning Commission has clearly stipulated that such products shall be regulated as pharmaceuticals, and may only be promoted on a large scale after their safety and efficacy have been confirmed through scientific, standardized, and rigorous clinical trials, and formal approval has been obtained from the relevant authorities.
Among current tumor immunotherapies, CAR-T stands out. Yu Lei, founder of a leading company in this field, pointed out that existing clinical cancer treatments—such as surgery, radiotherapy, chemotherapy, targeted drugs, and monoclonal antibodies—are unable to achieve a cure for tumors.
Unlike humoral immune approaches such as CAR-T and antibody drugs, this therapy equips the body’s innate cellular immune system with a powerful new cytotoxic weapon, offering the potential to completely eradicate tumor cells and cure malignant cancers, thus representing a revolutionary treatment modality.
In China, the Chinese PLA General Hospital is leading in clinical trials. Current Phase I data for three CAR-T therapies—CAR-T CD19 for acute lymphoblastic leukemia, CAR-T CD20 for diffuse large B-cell lymphoma, and CAR-T CD30 for Hodgkin’s lymphoma—indicate that this targeted tumor immunotherapy is relatively safe, feasible, and effective.
In 2017, the CD19+CD22 dual-target CAR-T technology, developed by Hebei Senlang Biotechnology Co., Ltd., successfully treated a leukemia patient at the Second Hospital of Hebei Medical University. This marked the first successful clinical case in China using CD19+CD22 dual-target CAR-T therapy.
Overall, cancer immunotherapy will evolve toward personalized medicine, with combination therapies employed to enhance efficacy. Since these therapies achieve autoimmunity through the modification of patients’ own T cells, their cytotoxicity and neurotoxicity cannot be overlooked. Furthermore, investigating potential long-term sequelae or risks of other diseases in patients undergoing cancer immunotherapy represents a future direction for the field.