AI Is Reshaping Clinical Trials and Apple Is Unifying Data to Reinvent the Process: Insights from CB Insights
Technology has brought boundless wealth to the pharmaceutical industry, fueling its unprecedented prosperity.
Testing new drugs is a slow, expensive, and labor-intensive process. Artificial intelligence has the potential to reshape every stage of the clinical trial process—from matching eligible patients to trials, to monitoring adherence and data collection.
In the United States, more than 1.7 million people were newly diagnosed with cancer in 2018. Meanwhile, over 10,000 clinical trials each need to recruit thousands of new patients to test experimental cancer drugs that could potentially save lives. However, fewer than 5% of cancer patients ultimately participate in these trials.
There are multiple reasons why it is difficult to match suitable patients for clinical trials. For terminal illnesses such as cancer, patients are eligible to participate in drug trials only after existing treatments have failed. Most importantly, not all patients diagnosed with terminal illnesses qualify for clinical trials; indeed, determining their eligibility itself is a formidable task.
For those eligible to participate in clinical trials, enrollment entails substantial costs and time commitments, while existing data collection methods further complicate this process.
Current clinical trial processes not only impose hardships on patients but also represent an inefficient workflow for other stakeholders, such as pharmaceutical companies and contract research organizations (CROs). Drug trials take nearly a decade on average and cost up to billions of dollars. Many trials fail due to enrollment issues. These factors underscore the need to transform the $65 billion clinical trial market.
Artificial intelligence is currently being hailed as a panacea, with immense potential to streamline cumbersome clinical trial processes. Examples range from Internet of Things (IoT)-enabled remote monitoring and machine learning for processing electronic health record (EHR) data, to AI-driven cybersecurity for data protection.
CB Insights, a renowned U.S. data services firm, recently analyzed the prospects and limitations of artificial intelligence in clinical trials. VCBeat (WeChat ID: vcbeat) has compiled and translated this analysis.
This article mainly covers the following content:
1. Why do pharmaceutical companies need to accelerate the drug development process?
Current Status of Clinical Trials
2. How is AI Transforming the Clinical Trial Process?
Matching Patients and Trials in Patient Recruitment
Simplified Registration Process
In terms of data collection and dependency
3. How Apple Is Preparing to Restructure Clinical Trials
4. Why AI Alone Cannot Be a Panacea
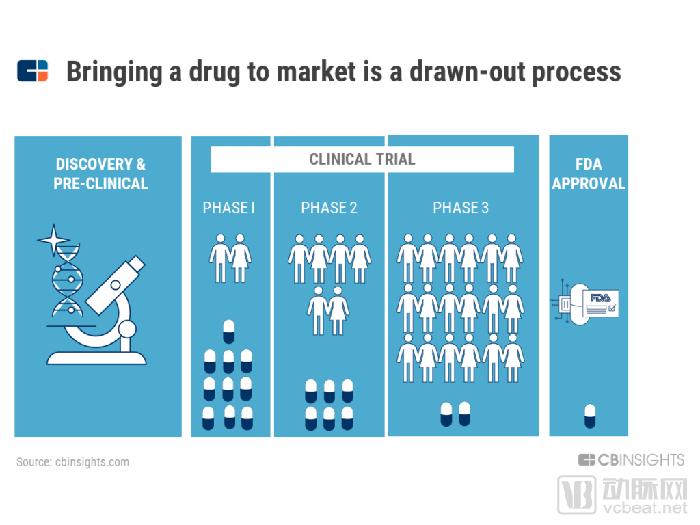
The launch of a new drug is a long and arduous process.
Although there is no central repository for drug development-related expenditures and timelines, studies estimate that it takes an average of 7.5 years to test new drugs on patients, with costs ranging from $161 million to $2 billion per drug.
As is well known, clinical trials are conducted in multiple phases, with costs escalating throughout the process. Phase III trials require larger patient populations and are significantly more expensive and complex than Phase I trials. Despite substantial investments of time and money, ultimately only one in ten new drugs that enter Phase I clinical trials receives FDA approval for market launch.
There are many reasons for the failure of clinical trials, including insufficient participant recruitment, patient dropout during the trial, unexpected and serious side effects, and improper data collection methods, all of which can lead to the premature termination of new drug development.
Certainly, the later a clinical trial fails, the higher the cost borne by both the sponsor and the patients. Sometimes, the blow from a failed clinical trial can be fatal to a pharmaceutical company.
For example, Novartis of Switzerland attributed its 15% year-on-year decline in net income for the first quarter of 2017 to the failure of a Phase III drug candidate for the treatment of heart failure. In another instance, in the United States, the CEO of Tenax Therapeutics resigned two months after the company’s lead drug candidate failed in Phase III clinical trials. The company is reportedly considering a merger or sale.
For small biopharmaceutical companies and start-ups entering this field, the cost of failure is more significant. The risk of failure is absolute, especially when pharmaceutical companies bet on only one drug.
The high costs associated with drug development are ultimately passed on to consumers. The healthcare services purchased by consumers not only cover the costs of successfully developed drugs but also bear the burden of failed clinical trials. This is why drug prices are so high.
Beyond the economic costs, the human cost of failed or ineffective trials is borne by patients.
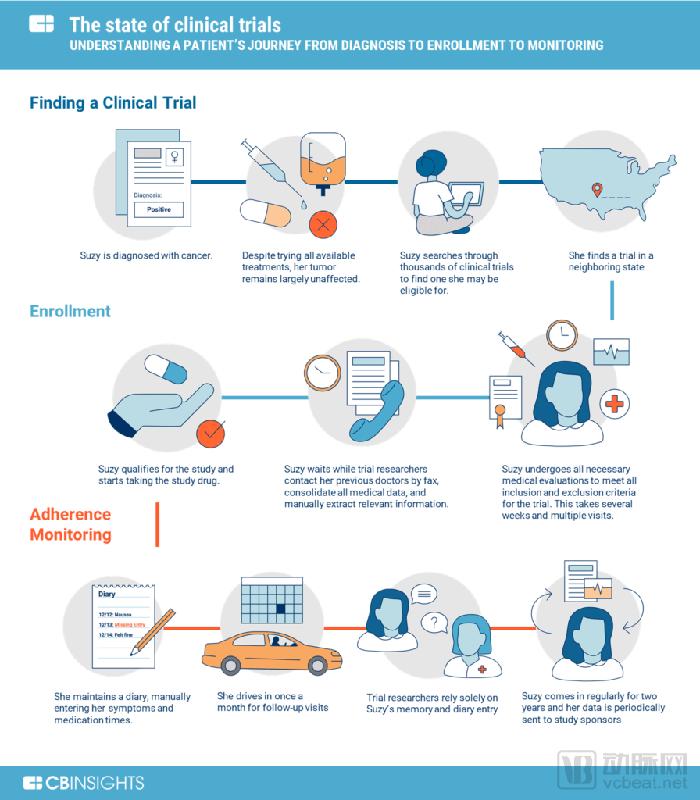
For most patients, discovering clinical trials is a process of trial and error, but registration and participation bring new challenges.
Many clinical studies still rely on primitive and outdated methods to collect and verify data, such as sending patients’ medical records via fax, manually counting remaining pills in bottles, and relying on patient diaries to assess medication adherence. Clearly, this process needs to be reengineered.
How AI Will Transform Clinical Trials
It can be said that AI has the potential to transform every aspect of clinical trials, from trial registration to patient adherence management.
Transforming the current clinical trial process by matching suitable patients with the appropriate clinical trials can save significant time for both patients and pharmaceutical companies.
According to a report by Cognizant on recruitment forecasts, approximately 80% of clinical trials fail to enroll suitable patients within the designated timeframe, and about one-third of Phase III clinical studies are terminated due to difficulties in patient recruitment.
Currently, more than 18,000 clinical trials are recruiting patients in the United States, with approximately 1,000 of them focused solely on breast cancer. Citing a statement from the White House in May 2018, VBInsight noted, “In fact, only 3% of cancer patients participate in clinical trials.”
If physicians are aware of ongoing trials, patients may occasionally receive trial recommendations from them. Otherwise, patients must independently seek relevant information from the government-run ClinicalTrials.gov database. ClinicalTrials.gov is a comprehensive federal database that collects information on both past and ongoing clinical trials.
If AI is available, the ideal approach would be to use artificial intelligence software to extract relevant information from patients’ medical records, compare it with ongoing clinical trials, and recommend matched studies.
In fact, extracting information from medical records—including electronic health records (EHRs) and laboratory images—is one of the most popular applications of artificial intelligence in the healthcare sector. However, the practical implementation of this technology must confront several challenges, such as unstructured medical data and disparate data sources that lack interoperability.
Challenges of EHR Interoperability
Despite the federal government spending more than $28 billion over the past decade to promote digital electronic health records (EHRs), there is no centralized repository or standard format for patients’ medical data. In fact, it is difficult for patients to aggregate all their medical information from every healthcare institution they have visited.
The HIPAA Act is a law that protects patients' medical data and privacy. It allows the sharing of patient data with personally identifiable information such as names and Social Security Numbers (SSNs), generally based on patients signing informed consent forms. This enables artificial intelligence startups to analyze these medical data within minutes and recommend eligible patients, a process that would take several months under current procedures.
However, issues of interoperability (compatibility) persist, making it difficult to seamlessly share health information across institutions or between different software systems.
Different hospitals treating the same patient may use different EHR software to enter data. In clinical trials, researchers still send fax requests for specific patient records to different hospitals, which subsequently transmit or email the information as images (including images of handwritten notes or PDF files).
This poses a challenge to artificial intelligence technology. A study by researchers at the Massachusetts Institute of Technology, Harvard University, Johns Hopkins University, and New York University states: “Standard natural language processing tasks, such as sentiment analysis and word sense disambiguation, are difficult in clinical annotations because clinical data often contain spelling errors, abbreviations, and extensive copy-and-paste content.”
Health AI company Flatiron Health further explained this in a patent application: “Structured data can also become unstructured due to the method of transmission. For example, spreadsheets faxed or converted into read-only documents (such as PDFs) lose much of their structure.”
This outdated manual system makes it difficult for clinical trial researchers to collect the accurate data needed to determine patient eligibility.
Last year, Mendel, a California-based startup, attempted to address this challenge by leveraging AI to integrate cancer patients’ medical histories. Patients can submit their medical records on Mendel’s platform, or alternatively, authorize Mendel to collect all their medical records from physicians on their behalf.
Mendel is developing machine learning algorithms to extract information from digital records and match patients with the clinical trials best suited to their needs. The startup charges patients on a subscription basis, with an introductory price of $99 for processing all medical record data during the first three months.
However, Mendel has not announced any further expansion plans since then, nor has it raised additional funding. Furthermore, the option to upload medical records on its website is no longer available.
Other companies, such as Antidote.me, are using machine learning to simplify the terminology in the “inclusion/exclusion” criteria listed on the ClinicalTrials.gov website.
In the B2B sector, startups are leveraging deep learning and natural language processing to automate clinical trial matching by collaborating directly with healthcare institutions. For example, Deep 6 AI partners with Cedars-Sinai Medical Center and TD2, an oncology CRO company.
Acquisition as a Strategy to Address Interoperability
Flatiron Health acquired Altos Solutions, an EMR company focused on oncology, in 2014, addressing interoperability issues.
At the time, Flatiron was selling its cloud analytics platform to healthcare and life sciences companies. Altos’s EMR system was also used by Florida Cancer Specialists, an oncology practice. The deal enabled Flatiron to directly access patients’ raw data, rather than relying solely on third-party emails.
To date, more than 2,500 clinicians have used Flatiron’s OncoEMR, with reports indicating that over 2 million active patient records are available for research.
Furthermore, Roche acquired Flatiron for $1.9 billion in February 2018, making it one of the largest mergers and acquisitions in the field of artificial intelligence. This, combined with Roche’s recent acquisitions of Foundation Medicine and Viewics as part of its broader digital initiatives, underscores Roche’s intention to reposition itself as a data-centric, machine learning-driven pharmaceutical company.
Challenges in Clinical Trial Registration
Identifying a suitable clinical trial does not mark the end of the enrollment process. Instead, patients must visit the trial sites to confirm their eligibility and undergo an initial telephone screening with researchers from the clinical study team. Patients must also meet the inclusion and exclusion criteria listed for the trial, as each participant must satisfy the eligibility requirements for a specific study. These criteria are often replete with medical terminology.
For example, in an FDA-approved clinical trial for breast cancer, patients must undergo evaluations, such as laboratory and imaging tests, to ensure they meet all inclusion and exclusion criteria.
Depending on their availability and proximity to the trial site, some patients can complete these procedures in less than a week. However, for those juggling work, parenting responsibilities, or long commutes, the process may require multiple trips.
As part of the eligibility verification process, on-site investigators collect patients’ medical records from other physicians’ offices. As previously noted, these faxed or emailed copies add a layer of complexity when using artificial intelligence to extract information.
If eligible, patients sign an informed consent form agreeing to the terms of the clinical trial. This includes acknowledging potential side effects, willingness to provide biological samples containing genetic information, and covering costs not included in the research budget.
Some AI-powered solutions that extract information from patient medical records can help streamline the enrollment process by automatically verifying certain inclusion and exclusion criteria.
A more effective solution is to leverage patient-generated data. Given the vast volume of data generated in real time, AI and patient-generated data are inextricably linked. Apple is currently exploring applications in this area.
Apple is gradually building a clinical research ecosystem centered around the iPhone and Apple Watch. By continuously monitoring patients in the comfort of their homes, the company can generate vast amounts of health data that were previously inaccessible.
Apple has been collaborating with healthcare institutions and medical researchers to efficiently identify patient cohorts suitable for their studies. This aspect will be discussed in detail below.
After the patient confirms participation in the clinical trial. Upon returning home, the patient will take the medication for the first treatment cycle (e.g., a 30-day supply bottle with dosage instructions) and a patient diary to be completed daily. Many clinical studies still use paper diaries rather than electronic systems.
Patients taking the investigational drug should pay attention to other medications being taken concurrently, as well as any adverse reactions (including headache, stomach pain, and muscle pain).
This reveals that the recording of clinical trial data relies on unverifiable sources, such as patient recall and paper records, leading to inefficiencies.
Reliance on Patient Memory: When patients come for regular check-ups, researchers examine their medication bottles to ensure no pills remain and review patient diaries for any gaps or inconsistencies. If information is missing from diary entries, researchers rely on the patients’ memory of events. This makes the process susceptible to human error.
Outdated Record-Keeping Systems: Paper-based documents are prone to information loss, representing an obsolete and unreliable method in which critical recorded data may be lost.
Risk of Patient Dropout: Frequent travel to clinical trial sites for regular check-ups imposes time and financial burdens on patients, particularly those traveling from abroad (e.g., airfare, hotel accommodations, and leave from work). This increases the risk of patient discontinuation.
Additional Costs: Although patients’ informed consent forms include out-of-pocket expenses, many patients do not understand that additional costs may arise. For example, extra MRI scans and laboratory tests performed during follow-up visits may not be covered by the clinical trial, and insurance companies will not reimburse these expenses because they are considered for “research” purposes rather than being “medically necessary.”
Failure to adhere to treatment or improper medication use may adversely affect patients’ health. For sponsors, enrolling new patients in a study increases costs and compromises the accuracy of study results.
Sponsors of clinical trials are eager to change this situation and are investing in technology to do so.
In addition to using mobile technology to remind patients to take their medications, Pfizer and Novartis are also investing in the Internet of Things (IoT) and “ingestible sensors” to track medication adherence. In the first quarter of 2017, Merck Ventures participated in Medisafe’s $14.5 million Series B financing round; Medisafe develops smart pill bottles with wireless connectivity.
AI startups have gone to great lengths to improve patient adherence by offering visual confirmation solutions. AiCure, a mobile SaaS platform headquartered in New York, uses image and facial recognition algorithms to track patient adherence. Patients record videos of themselves swallowing pills with their smartphones, and AiCure verifies that the right person has taken the correct medication. Following a series of grants from institutions such as the National Institutes of Health and the National Institute on Drug Abuse, AiCure has raised an additional $27 million in a new round of financing.
Another startup in this field, Catalia Health, which is backed by Khosla Ventures, is developing an AI-powered healthcare companion and advisor.
Catalia aims to reinforce patient behavior change by asking targeted questions, setting reminders, and tailoring conversations to each individual patient. One of the company’s objectives is to understand the reasons behind poor patient adherence. Catalia’s robotic assistant is essentially a tablet equipped with a touchscreen; however, the startup is also reported to be working on voice-activation capabilities.
It is worth noting that the ability of AI assistants to successfully transform lifestyles largely depends on patients’ willingness to interact with AI on a daily basis—a factor that can be monitored through AIoT (Artificial Intelligence of Things) technology.
An emerging trend is the integration of biosensors with artificial intelligence.
To this end, some startups are developing their own monitoring devices and sensors, then adding a layer of machine learning to interpret the data. Others are focusing solely on developing AI software and integrating it with third-party home monitoring devices.
Israeli company ContinUse Biometrics is developing its own sensing technology. The startup monitors more than 20 biological parameters—including heart rate, blood glucose levels, and blood pressure, which are some of the standard vital signs measured during drug trials—and uses artificial intelligence to detect abnormal patterns. The company raised $20 million in its Series B financing round in the first quarter of 2018.
Biofourmis is developing an artificial intelligence analytics engine that extracts data from FDA-cleared home monitoring devices and predicts patient health outcomes.
AI + IoT holds the potential for real-time, continuous monitoring of patients’ physiological and behavioral changes in clinical trials, potentially reducing the cost, frequency, and complexity of on-site monitoring.
For small startups, the biggest obstacle to simplifying clinical trials is that these technologies are relatively new and the industry adapts slowly.
However, tech giants such as Apple have seen success in attracting partners to participate in their healthcare-focused initiatives. Apple has already addressed some bottlenecks in the medical industry’s information flow by allowing researchers to use its APIs to build artificial intelligence applications.
In particular, Apple is building a clinical research ecosystem centered around its two devices: the iPhone and the Apple Watch. Data is at the core of artificial intelligence applications. Through these products, Apple can provide medical researchers with two streams of data that are currently difficult to obtain.
Apple's Big Data Stream
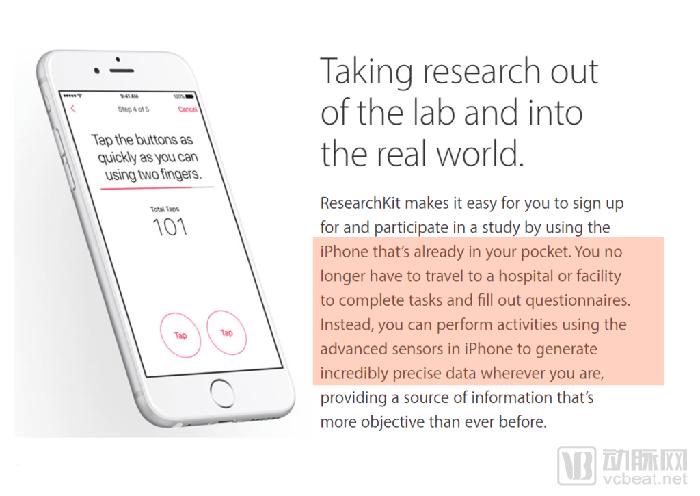
Since 2015, Apple has launched two open-source frameworks—ResearchKit and CareKit—to help recruit patients for clinical trials and remotely monitor their health status. These frameworks allow researchers and developers to create medical applications that monitor patients’ daily lives.
For example, researchers at Duke University developed an app called “Autism & Beyond,” which uses the iPhone’s front-facing camera and facial recognition algorithms to screen children for autism.
Similarly, nearly 10,000 individuals have used the mPower app, which employs exercises such as finger tapping and gait analysis to study Parkinson’s disease with users’ informed consent. Other variants of the app, such as HopkinsPD for Android users, leverage machine learning to process data collected from smartphones, thereby assessing the severity of patients’ Parkinson’s disease.
Reimagining EHR Data Sharing
In January this year, Apple announced that iPhone users can now access all their medical record information through the Health app on their iPhones. This feature, known as the “Health Records” API, is an extension of the work done by Gliimpse, an AI-driven healthcare startup acquired by Apple in 2016.
Information on the Gliimpse website indicates that its “core technology converts medical documents into data, enabling easy search and filtering of the most important graphs and dashboards.” This aligns with Apple’s Health Records feature—a user-friendly interface that allows users to find information on allergies, conditions, immunizations, lab results, medications, procedures, and vital signs.
Apple has also partnered with leading EHR vendors such as Cerner and Epic to address interoperability challenges. A potential ultimate goal of these collaborations may be bidirectional data flow, in which EHR vendors are encouraged to integrate patient-generated data into Apple’s software.
Apple stated, “More than 500 physicians and medical researchers are using Apple’s ResearchKit and CareKit software tools to conduct clinical studies involving 3 million participants, covering conditions ranging from autism and Parkinson’s disease to post-surgical home rehabilitation and physical therapy.”
In June this year, Apple launched the Health Records API for developers. Users can choose to share their data with third-party applications or medical researchers. This move has opened up new possibilities for disease management and lifestyle monitoring.
What Do These Data Mean for Clinical Research?
Apple is now at the center of a new medical data ecosystem, providing previously inaccessible health data while collecting EHR information that is difficult to integrate.
The application scenarios are endless in leveraging artificial intelligence and machine learning for early diagnosis, driving drug design decisions, recruiting suitable patients for studies, and remotely monitoring patient progress throughout the research process.
A potential competitor to Apple in this field is Google. Google’s Project Baseline aims to recruit 10,000 patients and monitor their daily lives over a five-year period, which could ultimately benefit clinical trials.
Many trials include an experimental group (patients receiving the investigational drug) and a control group (patients receiving a placebo). The purpose of the control group is to establish a baseline for comparison with the symptoms observed in the experimental group. Patients are typically unaware of which medication they are receiving.
Patient-generated data—such as that being collected by Google’s Project Baseline—can eliminate the need for control groups, provide the necessary data for controls, and ultimately alleviate difficulties in patient recruitment. However, this initiative is still in its early stages, and practical applications may not be realized for several years.
The healthcare industry is at the forefront of artificial intelligence applications, piloting uses ranging from machine-assisted diagnosis to information extraction from electronic health records.
Notably, the use of AI in drug discovery is also gaining momentum. Pharmaceutical giants such as Merck have partnered with startups like Atomwise, and GlaxoSmithKline has collaborated with companies including Insilico Medicine to apply AI to new drug research and development.
However, the application of artificial intelligence in actual clinical trials remains in its early stages.
Compared to other areas of healthcare, there are fewer startups directly targeting clients in the clinical trials sector. In many aspects of clinical trials, the implementation of AI first requires digitalization across the entire industry.
As mentioned above, many trials still rely on paper diaries for data collection. Even if some parts are stored in digital format, they remain difficult to search. Furthermore, handwritten clinical records must overcome the challenges of natural language processing when extracting information.
One of the greatest obstacles in clinical trials will be overcoming inertia and thoroughly overhauling current processes that are no longer effective.
Another challenge will be to accurately understand where artificial intelligence can provide assistance and what its current limitations are. Researchers must focus their discussions on achievable short-term goals, rather than indulging in the fantasy that AI will make all problems disappear.
For now, developing new data sources and handing the data over to patients—as Apple is doing—has proven revolutionary in clinical research. A prime example is using app-based interactions to rate the severity of Parkinson’s disease in patients.
Ultimately, the goal of applying artificial intelligence to clinical trials will be to bridge the gap between the information currently available to patients and the information they truly need, enabling them to lead healthier lives.