CAR-T Cell Immunotherapy (Part II): Global Market Exceeds $60 Billion – Opportunities for Chinese Companies to Overtake Global Leaders
Independently produced by Probe Capital. Welcome to join the discussion~ Please add WeChat ID: S-caffeine
III. Analysis of the Policy Environment for CAR-T
(I) Policy Analysis
To address the R&D trends in CAR-T therapy, China has formulated corresponding regulatory and review policies.
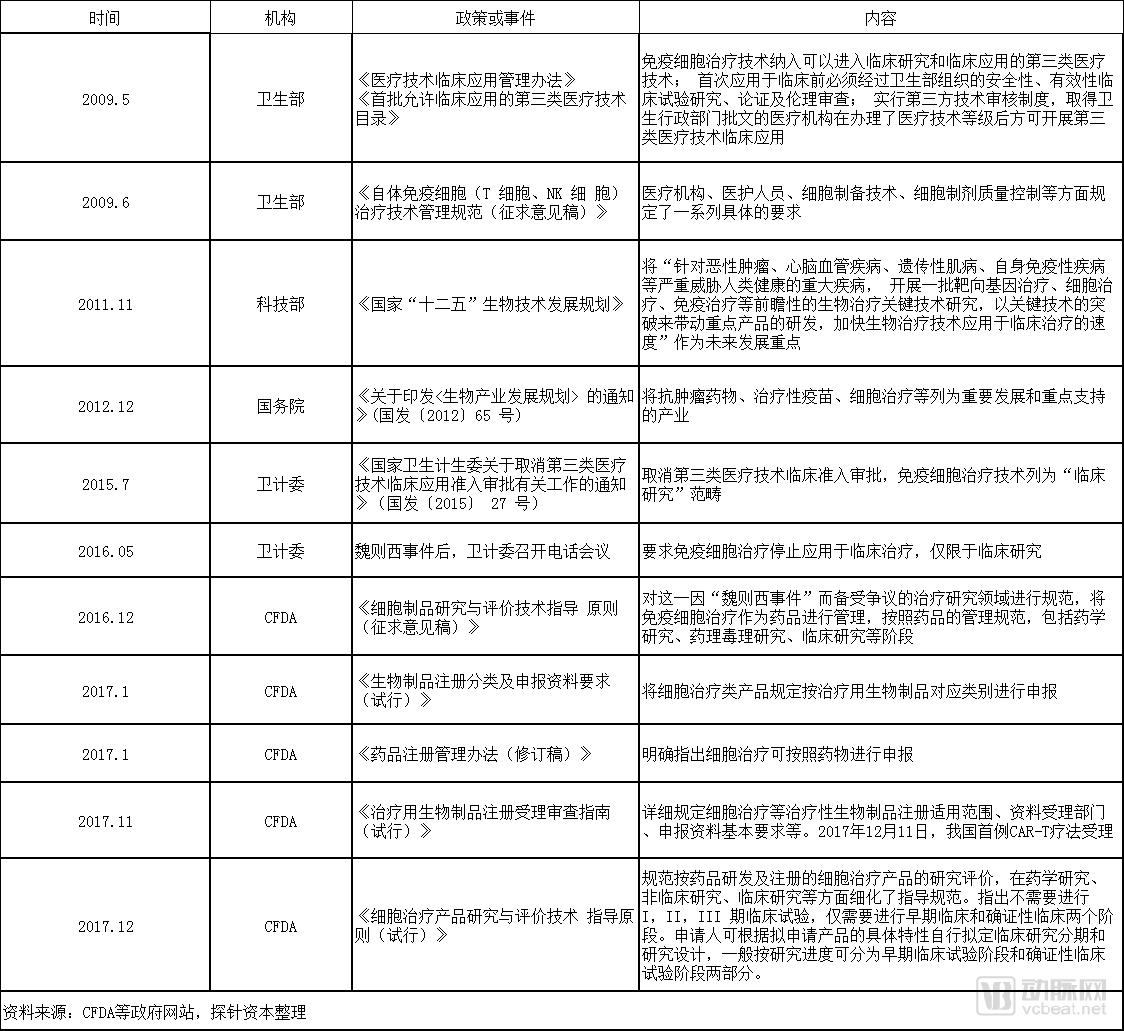
In November 2017, under the guidance of the “Guidelines for Acceptance and Review of Registration Applications for Therapeutic Biological Products (Trial),” the Center for Drug Evaluation (CDE) began accepting applications for clinical trials of domestic CAR-T therapeutic products. On December 11 of the same year, Nanjing Legend Biotech’s CAR-T project, the LCAR-B38M cell preparation, submitted a clinical trial application as a Class 1 new drug, becoming the first domestically submitted clinical trial application for a CAR-T project following its regulation as a drug. Subsequently, CAR-T projects from several other companies also received acceptance for their Investigational New Drug (IND) applications.
On December 22, 2017, the “Technical Guidelines for the Research and Evaluation of Cell Therapy Products (Trial)” was officially promulgated. The Guidelines point out that the design of clinical trials for cell therapies differs from that of traditional clinical trials. Applicants may independently formulate clinical study phases and study designs based on the specific characteristics of the product under application. Generally, these can be divided into early-stage clinical trial phases and confirmatory clinical trial phases according to research progress, which will significantly reduce the time required for clinical trials. Meanwhile, unnecessary animal studies may be conditionally waived if human trial data are already available; non-registration clinical trial data may be accepted to varying degrees depending on actual circumstances. These measures will accelerate the market launch of cell therapy products in China.
(1) Market Size
3.2.1 U.S. CAR-T Market Forecast: Total Market Size Approximately $38 Billion, with Hematologic Malignancies Accounting for Approximately $10 Billion
Currently, the most mature applications of CAR-T therapy remain in the field of hematologic malignancies, particularly in the treatment of B-cell leukemias and non-Hodgkin lymphoma.
On August 30, 2017, Novartis’s CAR-T product Kymriah (tisagenlecleucel, CTL019) became the first gene therapy approved by the FDA, as well as the first CAR-T therapy approved globally. It is indicated for the treatment of relapsed/refractory acute lymphoblastic leukemia in children and young adults (aged 2–25 years), with a price tag of $475,000.
In addition, in April 2017, Kymriah received Breakthrough Therapy Designation from the FDA for the treatment of relapsed or refractory (r/r) diffuse large B-cell lymphoma (DLBCL). On May 1, 2018 (U.S. time), Kymriah was approved for a second indication: the treatment of adult patients with relapsed or refractory large B-cell lymphoma who had previously undergone two or more lines of systemic therapy.
On October 18, 2017, Gilead’s (Kite) Yescarta (axi-cel, KTE-C19) became the second approved CAR-T therapy for the treatment of adult patients with specific types of diffuse large B-cell lymphoma (DLBCL), and it was also the first gene therapy approved for the treatment of non-Hodgkin lymphoma (NHL), priced at $373,000.
However, in myeloid leukemias—including AML and CML—multiple myeloma, Hodgkin lymphoma, and solid tumors such as colorectal cancer, lung cancer, and liver cancer, research and development are still in relatively early stages, holding immense potential for future applications.
According to Cancer Statistics 2018, the number of new cancer cases in the United States will reach 1.73535 million in 2018. The annual number of new cases includes 5,960 for ALL, 20,940 for CLL, 74,680 for NHL, 19,520 for AML, 8,430 for CML, 8,500 for HL, 30,770 for myeloma, 23,880 for brain or other nervous system tumors, 164,690 for prostate cancer, and 234,030 for lung and bronchus cancer.
Given that Kymriah is priced at $475,000 and Yescarta at $373,000, and taking into account the costs associated with research and development, manufacturing, quality control, and logistics for CAR-T therapies, as well as the size of the eligible patient population, we assume that the average price per single infusion for newly launched CAR-T products will be $350,000, based on existing pricing and efficacy data.
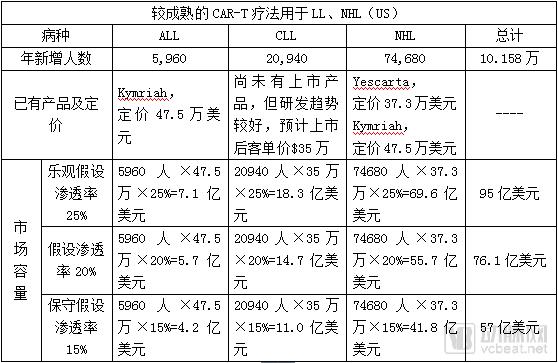
The total U.S. market size for other CAR-T therapies still in the R&D stage, applied to other cancer indications, is (with a conservative assumption of only 5% penetration rate due to the technologies being in the R&D and clinical trial phase):
(1.73535 million - 101,580) × $350,000 × 5% = $28.6 billion
Therefore, the total addressable market for CAR-T therapy in the United States is estimated at $38.1 billion under an optimistic scenario, $36.2 billion under a baseline scenario, and $34.3 billion under a conservative scenario.
3.2.2 Global CAR-T Market Forecast: Total Market Size Exceeds $60 Billion
In April 2018, a research report by Southwest Securities stated, “Since the global sales of the top 20 anti-tumor drugs are 1.75 times their U.S. sales, we believe that the global market for hematologic malignancies is 1.75 times the size of the U.S. market.”

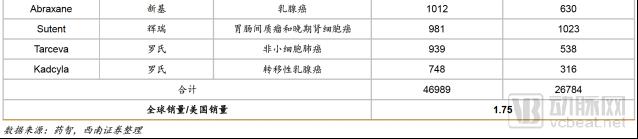
If the global CAR-T market is also 1.75 times the size of the U.S. CAR-T market, the global CAR-T market capacity could reach $66.675 billion in an optimistic scenario; $63.35 billion in a general development scenario; and $60 billion in a conservative scenario.
3.2.3 China CAR-T Market Forecast: Total Market Size of Approximately RMB 80 Billion, with Hematologic Malignancies Accounting for Approximately RMB 15 Billion
Currently, no CAR-T products have received marketing approval in China. Although Novartis’ Kymriah and Kite’s Yescarta have been approved for market launch by the FDA, they must still obtain approval from the CFDA after submitting a New Drug Application (NDA) to enter the Chinese market. On December 5, 2017, Fosun Pharma and Kite Pharma established a joint venture in China, Fosun Kite, thereby securing the commercialization rights for Yescarta in China as well as priority licensing rights for subsequent products. This May, the product received a “Notice of Acceptance” from the CFDA, but it has not yet obtained marketing approval.
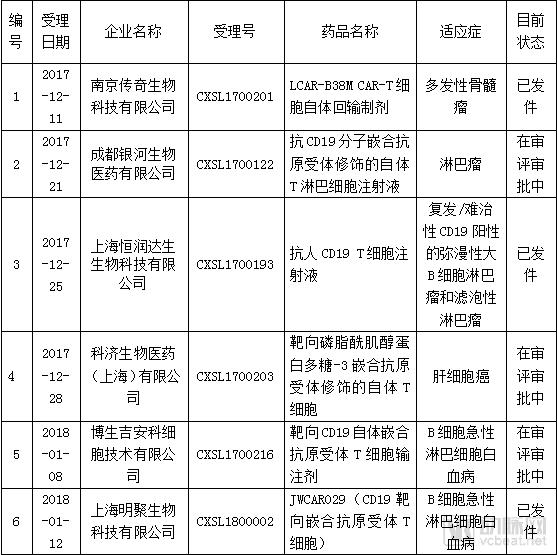
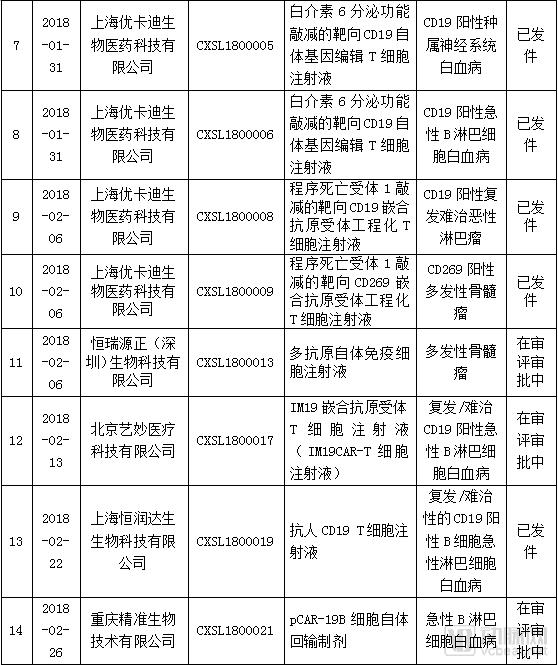
Regarding domestically produced CAR-T therapies, as of July 25, 2018, the Center for Drug Evaluation (CDE) had accepted a total of 24 Investigational New Drug (IND) applications for CAR-T products. Among these, 8 applications had been processed, and none had progressed to New Drug Application (NDA) submission. Specifically, 18 projects targeted leukemia or lymphoma, 5 targeted multiple myeloma, and 1 targeted hepatocellular carcinoma.
According to the data from "Cancer Statistics in China, 2015," the number of new cancer cases in China will reach 4.292 million in 2015. Among them, there were 75,300 leukemia patients, 88,200 lymphoma patients, 376,300 colorectal cancer patients, 446,100 liver cancer patients, and 733,300 lung cancer patients.
Assuming an annual 3% increase in new cancer cases in China, the number of newly diagnosed cancer patients is projected to reach 4.69 million in 2018, including 82,300 leukemia patients and 96,300 lymphoma patients. Additionally, with an incidence rate of approximately 1 per 100,000 for multiple myeloma in China, the estimated number of multiple myeloma patients is around 14,000.
Considering the R&D, manufacturing, quality control, and logistics costs of domestically produced CAR-T therapies, as well as the number of eligible patients, and taking into account factors such as the pricing of existing CAR-T products and China’s current basic economic level, it is assumed that the average unit price per single infusion for domestically launched CAR-T products will be RMB 300,000.
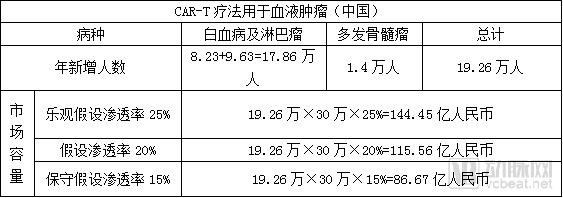
The market size in China for other CAR-T therapies currently in the R&D stage, applied to other cancer indications, is estimated as follows (due to the technologies still being in the R&D and clinical trial phases, a conservative assumption of a 5% penetration rate is applied):
(4.69 million - 192,600) × RMB 300,000 × 5% = RMB 67.461 billion
Therefore, the market size of CAR-T in China is estimated at RMB 81.9 billion under an optimistic scenario, RMB 79.0 billion under a baseline scenario, and RMB 76.1 billion under a conservative scenario.
(II) Competitive Landscape
Internationally, the three giants—Novartis, Kite, and JUNO—are at the forefront of research and development, continuously achieving breakthrough progress.
Currently, Novartis’s CAR-T product Kymriah and Kite’s Yescarta have been launched in the United States, targeting leukemia and non-Hodgkin lymphoma, respectively, and both are covered by U.S. health insurance programs.
China has not yet approved cell therapy products for market launch as drugs, but there are numerous approvals for clinical use.
Regarding the submission status of anti-tumor drugs, as of July 25, 2018, the Center for Drug Evaluation (CDE) had accepted a total of 24 Investigational New Drug (IND) applications for CAR-T products. Among these, 23 projects targeted hematologic malignancies, with indications including leukemia, non-Hodgkin lymphoma, and multiple myeloma. One project targeted solid tumors, specifically liver cancer.
Among the projects currently filing for IND, eight have had their submissions issued, originating from companies such as Legend Biotech, JW Therapeutics, Shanghai Hengrun Dasheng, and Shanghai Ucar-T.

(4) Analysis of Classic Overseas Corporate Cases and Products
3.4.1 Novartis
Novartis, founded in 1996 and headquartered in Basel, Switzerland, is an international pharmaceutical and biotechnology company whose core businesses span multiple fields, including innovative patented medicines, eye care, generic drugs, consumer health, and vaccines and diagnostics.
In August 2012, Novartis entered into a collaboration agreement with the University of Pennsylvania, obtaining authorization to develop CAR-T cell therapies based on the university’s research findings. Novartis invested $20 million to establish a laboratory and formed an independent gene and cell therapy team to commence CAR-T research and development. In 2014, Novartis formally submitted an Investigational New Drug (IND) application to the U.S. Food and Drug Administration (FDA), and clinical trials began in April 2015. By August 2016, as Novartis’s CAR-T cell therapy technology matured, the company fully accelerated the development of CTL019 for the treatment of relapsed or refractory (r/r) B-cell acute lymphoblastic leukemia (ALL) in children and young adults. In March 2017, the FDA accepted the Biologics License Application (BLA) for CTL019 for the r/r B-ALL indication and granted it Priority Review, shortening the review period to six months. On August 30, 2017, CTL019 received FDA marketing approval, becoming the world’s first approved CAR-T cell therapy product, marketed under the name Kymriah.
Latest official website data indicate that Kymriah achieved an objective response rate (ORR) of 83% within three months in CAR-T clinical treatment for relapsed/refractory B-cell acute lymphoblastic leukemia (r/r B-ALL) (N=52). In pivotal clinical trials, the three-month response rate was 82%, the six-month overall survival rate was 89%, and the twelve-month overall survival rate was 79%, demonstrating the significant efficacy of CAR-T cell therapy. Among patients, 49% experienced grade 3 or higher cytokine release syndrome (CRS), and 18% experienced grade 3 or higher neurological events (with specific symptoms including headache, coma, anxiety, seizures, etc.); however, no cases of cerebral edema were reported.
To secure FDA approval for Kymriah’s second indication (r/r DLBCL), Novartis and the University of Pennsylvania jointly presented new data from the pivotal global Phase II JULIET clinical trial at the American Society of Hematology (ASH) annual meeting on December 10, 2017. The study evaluated the efficacy of Kymriah (CTL019) in patients with relapsed or refractory diffuse large B-cell lymphoma (r/r DLBCL). The data showed that among 81 patients followed for three months or longer, the overall response rate (ORR) was 53%, with a complete response (CR) rate of 40% and a partial response (PR) rate of 14%. At six months post-infusion, the ORR was 37%, with a CR rate of 30% and a PR rate of 7%.
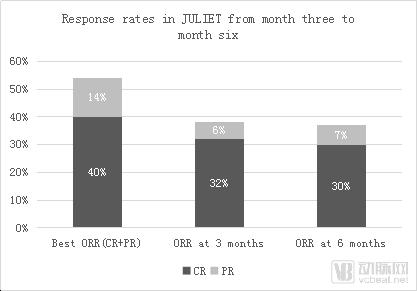
Data Source: Novartis Official Website; Compiled by Probe Capital
Regarding adverse events, 58% of patients experienced cytokine release syndrome (CRS), with 23% experiencing Grade 3/4 CRS (15% Grade 3, 8% Grade 4). Neurological events occurred in 21% of patients, with 12% experiencing Grade 3/4 severity. Additionally, Grade 3/4 cytopenias lasting more than 28 days, Grade 3/4 infections, and Grade 3/4 febrile neutropenia were observed in 27%, 20%, and 13% of patients, respectively. Three patients died within 30 days post-infusion due to progressive underlying disease; however, no cases of cerebral edema or treatment-related deaths were reported.
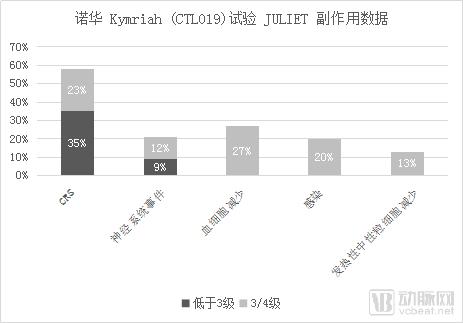
Source: Novartis official website; compiled by Probes Capital
On January 17, 2018, Novartis announced that the U.S. FDA had granted Priority Review for its Biologics License Application (BLA) seeking approval of Kymriah for the treatment of adult patients with diffuse large B-cell lymphoma (DLBCL). Concurrently, the European Medicines Agency (EMA) granted Accelerated Assessment designation to Novartis’s Marketing Authorization Application (MAA) for Kymriah in the treatment of relapsed or refractory B-cell precursor acute lymphoblastic leukemia (r/r B-ALL) and relapsed or refractory DLBCL (r/r DLBCL). On May 1, 2018 (U.S. time), the U.S. FDA approved Kymriah (tisagenlecleucel, CTL019), a CAR-T cell therapy, for its second indication: the treatment of adult patients with relapsed or refractory large B-cell lymphoma who have received two or more prior lines of systemic therapy.
Kymriah is priced at $475,000. On April 1, 2018, the U.S. Centers for Medicare & Medicaid Services (CMS) announced that it would reimburse hospitals $500,000 for Novartis’s CAR-T therapy Kymriah, covering part of the costs for disabled individuals, patients with end-stage renal disease, and special patients aged 65 and older who are enrolled in Medicare Part B. These patients are responsible for approximately 20% of the treatment costs out-of-pocket. According to disclosures on Novartis’s official website, Kymriah generated $12 million in sales revenue in the first quarter of 2018.
3.4.2 Kite Pharma (acquired by Gilead; established Fosun Kite in partnership with Fosun Pharma)
Kite Pharma, founded in 2009, was acquired by Gilead Sciences for $11.9 billion on August 28, 2017. Headquartered in Santa Monica, California, Kite Pharma is dedicated to the development of novel oncology immunotherapy products and stands as one of the world’s leading enterprises in T-cell therapy research and development. It is the only pharmaceutical company globally licensed by the U.S. National Institutes of Health (NIH) and has established extensive collaborative relationships with both the National Cancer Institute (NCI) and the NIH.
In January 2015, Amgen made an upfront payment of $60 million to collaborate with Kite Pharma on the development of novel cancer immunotherapies, aiming to advance the research, development, and commercialization of CAR-T cell immunotherapy. In December 2015, Kite presented Phase I clinical data for its CAR-T therapy KTE-C19-101 (ZUMA-1) in patients with refractory malignant non-Hodgkin lymphoma (NHL) at the American Society of Hematology (ASH) Annual Meeting. Meanwhile, the U.S. Food and Drug Administration (FDA) granted Breakthrough Therapy Designation to Kite’s KTE-C19 for the treatment of NHL during its Phase II clinical trials.
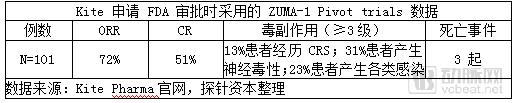
In September 2016, Kite Pharma announced interim data from the Phase II clinical trial of KTE-C19 (ZUMA-1). The results showed that among patients with diffuse large B-cell lymphoma (DLBCL; n=51), the overall response rate (ORR) was 76% and the complete response rate (CRR) was 47%; among patients with transformed follicular lymphoma (TFL; n=11), the ORR was 91% and the CRR was 73%. The efficacy outcomes met expectations.
However, in May 2017, the death of a patient due to cerebral edema in the KTE-C19 trial had a certain negative impact on the Biologics License Application (BLA). In December 2016, Kite announced that it would submit a marketing application to the U.S. Food and Drug Administration (FDA) based on the latest pivotal data from the ZUMA-1 trial. On October 18, 2017, Kite Pharma’s product KTE-C19 received FDA approval for market launch. The FDA approved the product for the treatment of adult patients with specific types of diffuse large B-cell lymphoma (DLBCL) who are refractory or relapsed after at least two prior lines of therapy. This made it the second CAR-T cell immunotherapy product globally, following Novartis’ CTL-019.
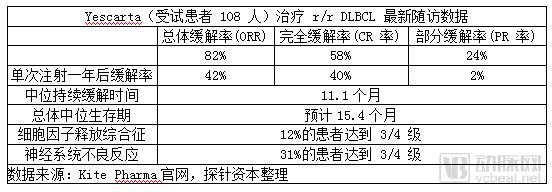
To assess the tolerability of Yescarta-induced remission, Kite conducted a minimum one-year follow-up of patients with refractory aggressive non-Hodgkin lymphoma (n=108) enrolled in the ZUMA-1 study; subsequent follow-up confirmed significant efficacy. Among patients with advanced diffuse large B-cell lymphoma (DLBCL) who would typically survive only six months with conventional therapy, more than half remained alive one year after receiving Yescarta, with a median overall survival estimated at 15.4 months.
Currently, the product is priced at $373,000. The Centers for Medicare & Medicaid Services (CMS) reimburses hospitals providing Yescarta therapy $395,380 for patients enrolled in Medicare Part B (Supplementary Medical Insurance), with a minimum patient co-payment of $79,076. Additionally, patients are required to pay a $1,340 deductible as the threshold for reimbursement.
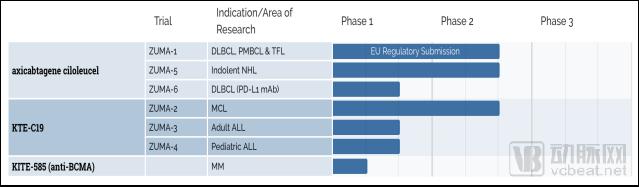
As of July 2018, Kite had seven CAR-T therapies in development, three of which involved KEC-C19. Additionally, the company initiated research into BCMA-targeted CAR-T cell therapies for multiple myeloma (MM).
Data Source: Kite Pharma Official Website
To expand its CAR-T products internationally and enter the Asian market, Kite announced on January 9, 2017, a collaboration with Daiichi Sankyo of Japan to introduce the KTE-C19 product for research, development, and commercialization in Japan, with an upfront payment plus milestone payments totaling over USD 200 million. On January 10, 2017, Fosun Pharma announced that Kite had established a joint venture, Fosun Kite Biotechnology, with Shanghai Fosun Pharmaceutical Industry (a wholly-owned subsidiary of Fosun Pharma), dedicated to exploring the Chinese market.
3.4.3 Juno (acquired by Celgene; established Shanghai WuXi Juno in partnership with WuXi AppTec)
Juno, founded in 2013 and headquartered in Seattle, Washington, USA, is a small biopharmaceutical company established through a collaboration between the Fred Hutchinson Cancer Center, Memorial Sloan Kettering Cancer Center, and Seattle Children’s Research Institute. The company primarily focuses on the development of CAR-T and TCR-T cell therapies and was formerly one of the “big three” in cell therapy (prior to the discontinuation of JCAR015). In January 2018, Juno was acquired by Celgene for $9 billion.
Juno’s fastest-advancing and most mature CAR-T product, JCAR015, was twice placed on clinical hold by the FDA after multiple patient deaths due to neurotoxicity and cerebral edema occurred during treatment. In March 2017, Juno officially announced the termination of the Phase II clinical trial of JCAR015, causing its CAR-T development program to fall behind those of its competitors, Novartis and Kite.
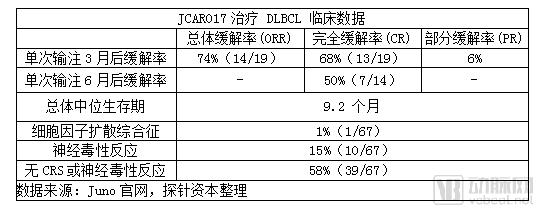
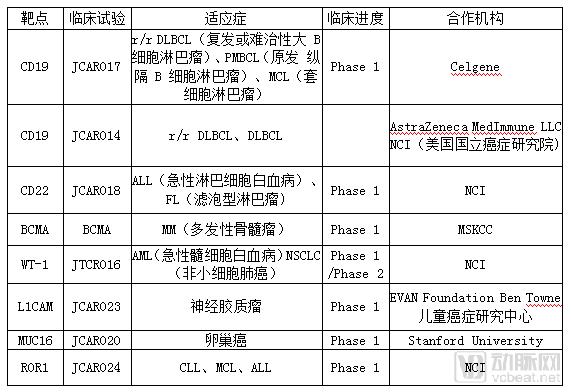
However, Juno’s other product, JCAR017, demonstrated superior safety and cure rates compared to Novartis in the treatment of relapsed or refractory B-cell non-Hodgkin lymphoma (NHL). The drug has received Breakthrough Therapy designation from the U.S. FDA for the treatment of relapsed/refractory (r/r) aggressive large B-cell NHL, and has also been granted PRIME status by the European Medicines Agency (EMA) for the treatment of diffuse large B-cell lymphoma (DLBCL). On December 9, 2017, Juno presented interim results from its clinical trial of the CAR-T therapy JCAR017 for relapsed/refractory CD19+ non-Hodgkin lymphoma at the American Society of Hematology (ASH) Annual Meeting. Among the 19 patients in the core cohort who received the high dose (DL2 = 100 million cells), the overall response rate at three months was 74% (14 patients), with a complete response rate of 68% (13 patients); the complete response rate at six months was 50% (7 patients).
Regarding adverse effects, among the 67 patients in the core cohort, 1% (1 patient) experienced severe cytokine release syndrome (CRS), 15% (10 patients) developed severe neurotoxicity, and 58% (39 patients) had no CRS or neurotoxicity.
In addition, Juno has JTCR016, a therapy targeting WT-1, which has initiated Phase I/II clinical trials for three indications: acute myeloid leukemia, non-small cell lung cancer, and mesothelioma.
In April 2016, WuXi AppTec and Juno Therapeutics jointly established Shanghai WuXi Juno Biopharmaceutical Co., Ltd. to accelerate the research, development, and industrialization of CAR-T products. The company is primarily responsible for researching and conducting cell immunotherapy within China. On March 8, 2018, WuXi Juno announced the completion of a $90 million Series A financing round led by Temasek, Sequoia Capital China, and Yuanming Capital. On June 27, 2018, WuXi Juno announced that its CAR-T product, JWCAR029, had successfully filed an Investigational New Drug (IND) application with the China Food and Drug Administration (CFDA) and entered the clinical trial phase.
3.4.4 Bluebird (co-developed with Celgene)
Bluebird, founded in 1992 and headquartered in Cambridge, Massachusetts, USA, is a clinical-stage biotechnology company dedicated to developing revolutionary gene therapies for the treatment of severe genetic and rare diseases.
In March 2013, Bluebird and Celgene entered into a strategic collaboration to jointly develop CAR-T therapies, with the signed agreement including milestone payments totaling $225 million. In June 2015, the two parties amended their collaboration agreement to prioritize the development of BCMA-targeting candidates, focusing specifically on research into bb2121, a CAR-T cell therapy targeting B-cell maturation antigen (BCMA), with associated costs amounting to $25 million. In March 2018, Celgene and bluebird reached a co-development agreement to jointly develop and commercialize the bb2121 therapy, with R&D costs and revenues in the United States shared on a 50:50 basis. Celgene would independently handle manufacturing and commercialization of bb2121 in markets outside the United States, while Bluebird would receive milestone payments and sales royalties.
In December 2017, Celgene and Bluebird jointly presented the Phase I clinical results of the CRB-401 trial at the ASH Annual Meeting, with a median follow-up time of 40 weeks (overall range: 6.6–69). The trial evaluated the safety and efficacy of the CAR-T cell therapy bb2121 in 21 patients with advanced relapsed or refractory multiple myeloma. The data showed:
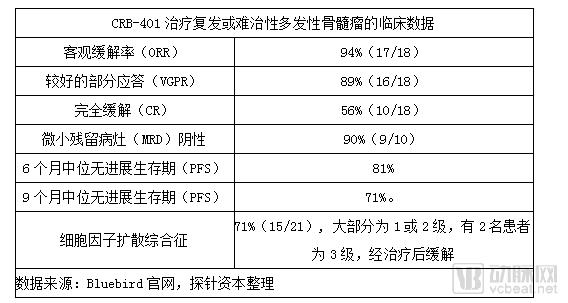
bb2121 therapy is currently undergoing pivotal Phase II clinical trials, while the second-generation anti-BCMA CAR-T therapy bb2127 has entered Phase I clinical trials. Leveraging outstanding efficacy and safety data from Phase I trials, Bluebird’s bb2121 received Breakthrough Therapy Designation from the FDA and Priority Medicines (PRIME) designation from the EMA in November 2017, with its first FDA filing expected in 2019.

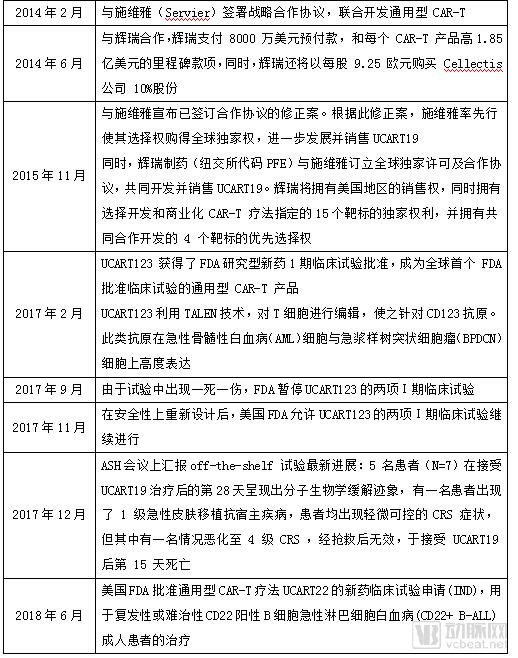
3.4.5 Cellectis (co-developed with Servier and Pfizer)
Founded in Paris, France, in 1999, Cellectis has emerged as a technologically transformative company with the potential to surpass the three major players in the CAR-T field through its development of allogeneic universal CAR-T cells. It boasts UCART123, the first universal CAR-T product globally to receive FDA approval for clinical trials.
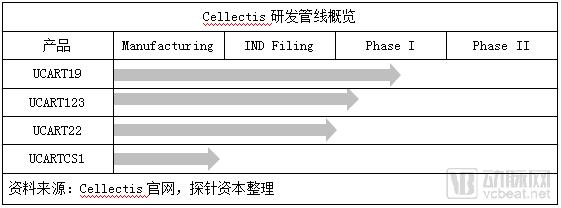
Cellectis’s engineered universal T cells offer advantages such as being allogeneic, cryopreserved, and “off-the-shelf,” enabling use in multiple patients and representing a new direction for CAR-T therapy. By leveraging its proprietary TALEN technology to knock out the αβ T-cell receptor (TCR) and the CD52 gene in CAR-T cells, Cellectis has taken a historic step toward resolving histocompatibility issues. Currently, Cellectis has four products in development, among which UCART19, targeting CD19, and UCART123, targeting CD123, have both entered Phase I clinical trials; both products are indicated for the treatment of hematologic malignancies.
Cellectis’s Development of Universal CAR-T Therapy: A Turbulent Journey
3.4.6 Bellicum
Bellicum Pharmaceuticals (NASDAQ: BLCM), founded in 2004 and headquartered in Houston, United States, is a biopharmaceutical company dedicated to the discovery and development of innovative cellular immunotherapies for various cancers. Its therapeutic areas include hematologic malignancies, solid tumors, and rare inherited blood disorders.
One of Bellicum’s core technologies is the molecular switch rimiducid. By introducing a signaling domain combined with a specially designed CID (chemically induced dimerization) system, this technology adds a molecular switch to CAR-T therapy. The small molecule rimiducid controls the activation and deactivation of signaling pathways, thereby enhancing the controllability of cell therapy. This approach addresses challenges such as significant inter-individual variability, difficulties in dose management, and the risk of severe adverse effects, enabling quality control over therapeutic outcomes.
Mechanism of Action of the Rimiducid Molecular Switch
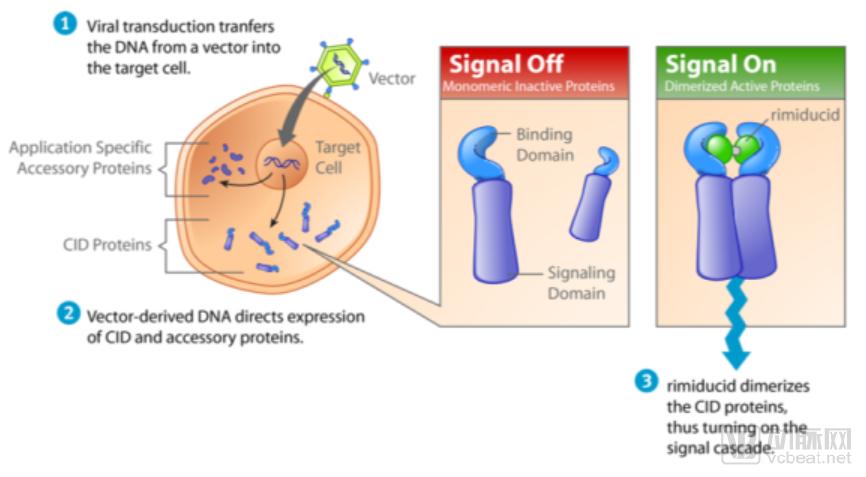
Image source:Bellicum Official Website, Compiled by Probes Capital
Leveraging its CID platform in combination with CAR-T technology, the company has developed the suicide switch CIDeCAR, the activity switch GoCAR-T, the suicide switch CaspaCIDe for bone marrow transplantation and TCR-T therapy, and DeCIDe for DCs.
The primary function of the activatable switch GoCAR-T is to induce T cell activation and proliferation. The investigational product in development is BPX-601. In vitro study data demonstrate that GoCAR-T products targeting prostate stem cell antigen (PSCA) significantly promote T cell proliferation and cytokine release.
The BPX-601 therapy, based on the company’s GoCAR-T technology, is currently in Phase I clinical trials. This Phase I clinical trial, named “BP-012” (ClinicalTrials.gov Identifier: NCT02744287), is an open-label, non-randomized dose-escalation study conducted at Baylor College of Medicine. The primary objective is to evaluate the safety and efficacy of BPX-601 in combination with rimiducid in 30 patients with unresectable pancreatic cancer.
Comparison between Traditional CAR-T Technology and GoCAR-T Technology
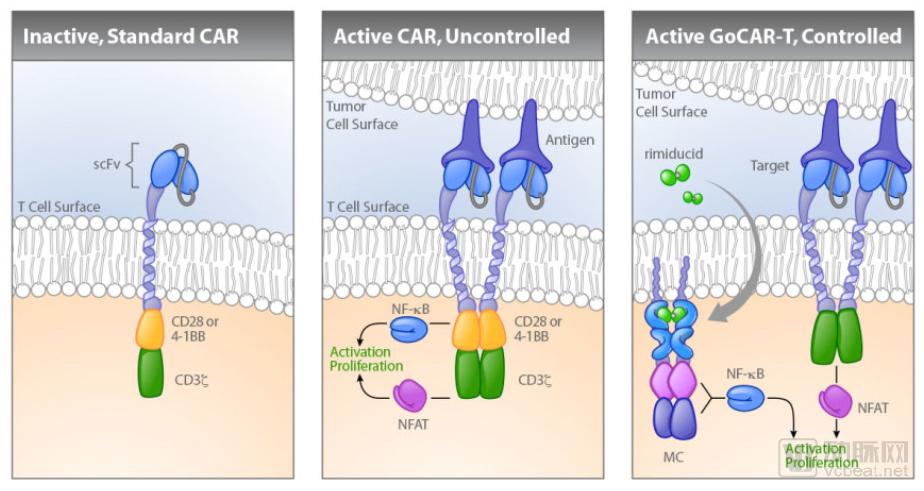
Image source: Bellicum official website; compiled by Probe Capital
Suicide Switch CaspaCIDe Technology: The primary function is to induce T-cell apoptosis, with related products including BPX-501 and BPX-701. BPX-501 is currently Bellicum’s most advanced cell therapy drug. Although three cases of brain injury occurred during the January 2018 clinical trial of BPX-501, leading the FDA to halt the trial, the BP-004 clinical trial of this product in Europe continues.
On March 13, Bellicum announced interim data from its investigational candidate therapy BPX-501 for the treatment of pediatric acute myeloid leukemia (AML) and primary immunodeficiencies (PIDs), demonstrating high response rates and high survival rates. The data indicate that BPX-501 T cells have the potential to achieve durable anti-leukemic effects in AML patients.
In this study, 38 pediatric patients with acute myeloid leukemia (AML) who received BPX-501 treatment after haploidentical hematopoietic stem cell transplantation (haplo-HSCT) achieved complete remission. After a median follow-up of one year, the relapse-free survival rate and overall survival rate were 91.5% and 97.3%, respectively. In contrast, the one-year survival rate for pediatric AML patients undergoing stem cell transplantation reported in the literature ranges from 60% to 80%.
Bellicum's R&D Pipeline
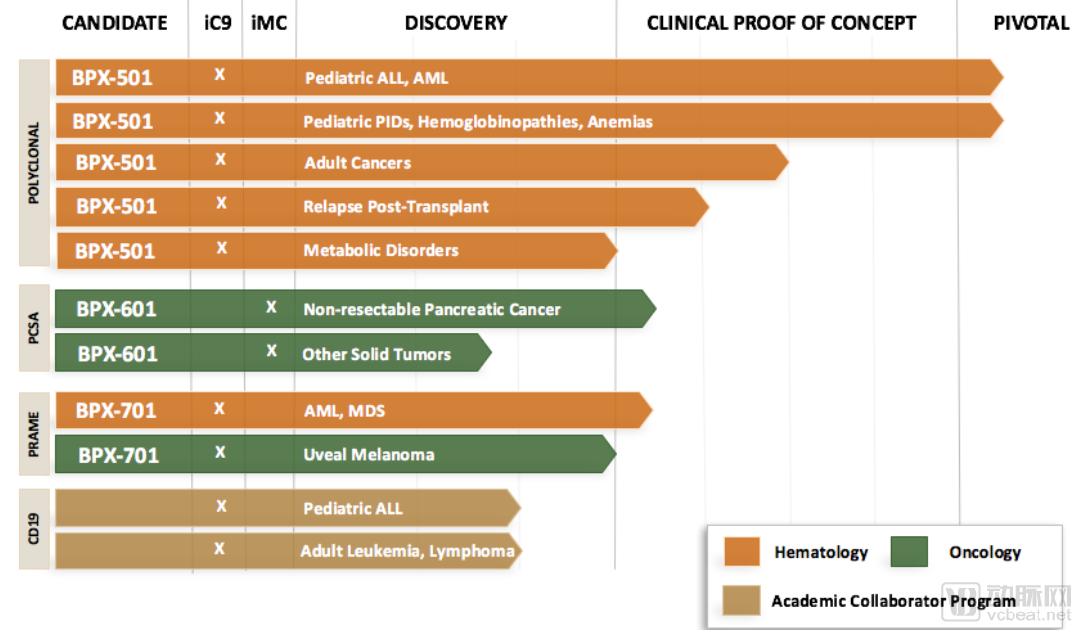
Image source: Bellicum official website; compiled by Probe Capital