Are Medical AI Companies Ready for Commercialization? Insights from Physicians’ Feedback and Product Landscape
For medical artificial intelligence, 2018 was a brand-new year. By the end of the year, the commercialization of AI was gradually unfolding.
At this pivotal juncture bridging the past and the future, VCBeat has invited more than 60 physicians, scholars, and business executives specializing in medical artificial intelligence to gather in Shanghai. Together, they will discuss advancements in medical AI, review past achievements, and focus on future developments.
At this conference, seven department directors delivered keynote speeches: Liu Shiyuan, Director of the Department of Diagnostic and Interventional Radiology and Nuclear Medicine at Changzheng Hospital; Zhao Shihua, Director of the Department of Radiology at Fuwai Hospital, Chinese Academy of Medical Sciences; Wu Liangcheng, Director of the Department of Ophthalmology at Shanghai Jing’an District Central Hospital; Gong Xiangyang, Director of the Department of Radiology at Zhejiang Provincial People’s Hospital; Hu Hongjie, Director of the Department of Radiology at Sir Run Run Shaw Hospital, Zhejiang University School of Medicine; Lin Hui, Director of the Office of Internet and Artificial Intelligence at Sir Run Run Shaw Hospital, Zhejiang University School of Medicine; and Chen Jili, Director of the Department of Ophthalmology at Shanghai Shibei Hospital.
VCBeat (WeChat Official Account: vcbeat), drawing on research findings from VCBeat Institute, has synthesized expert opinions to delineate a clear profile of artificial intelligence demand through the lens of their discourse.
In 2017, VCBeat Research Institute released its inaugural report on medical artificial intelligence, which provided a detailed analysis of AI applications in the healthcare sector, business models, production costs, and talent reserves. After a year of turbulence, AI companies have shifted their focus from merely touting algorithms, specificity, and sensitivity to prioritizing product implementation. Nevertheless, while the strategic priorities of AI enterprises need not align temporally with the broader trajectory of AI development, they must still regard algorithms, data, and computing power as their core competitive advantages.
When it comes to data, take the health and medical platform service provider Jiankang Youyi as an example. The daily number of API calls made by manufacturers such as Huawei and VIVO to this enterprise exceeds 500,000. The daily usage volume of Huiyi Technology’s data platform also reaches as high as 170,000 times. Given that the data usage frequency of these health enterprises has reached such a magnitude, does it indicate that the second wave of digitalization has begun to yield initial results?
Currently, the most widely applied AI products are those for diabetic retinopathy screening. Globally, there are over 415 million people with diabetes (2017 statistics), with China ranking first at 114.4 million. Among these patients, 21.4%–27.29% develop diabetic retinopathy during their working-age years. Therefore, diabetic retinopathy screening is characterized by both a large volume and high priority. However, it is not feasible for all screening tasks to be borne solely by tertiary hospitals; instead, they should be triaged to county-level and lower-tier medical institutions or specialized ophthalmic centers such as the Health Express.
Secondly, in-hospital imaging products are favored by enterprises. Over the past two years, physicians’ workloads have increased rapidly, with the overall volume of imaging studies rising by 10%–20%. In 2017, the total number of CT scans was 260,000, and the total number of MRI scans was 83,000. Each department generates approximately 1,000 X-ray images and performs around 1,000 CT scans daily, along with nearly 300 MRI, mammography, and gastrointestinal contrast studies. These figures reflect the substantial demand from enterprises.
Compared with other imaging AI products, AI solutions for cerebrovascular and cardiovascular diseases have higher entry barriers and greater technical challenges, resulting in relatively fewer market participants. However, the diagnostic process for cardiovascular diseases is complex; interpreting two-dimensional images to reconstruct a patient’s pathological condition requires not only clinical experience but also spatial imagination.
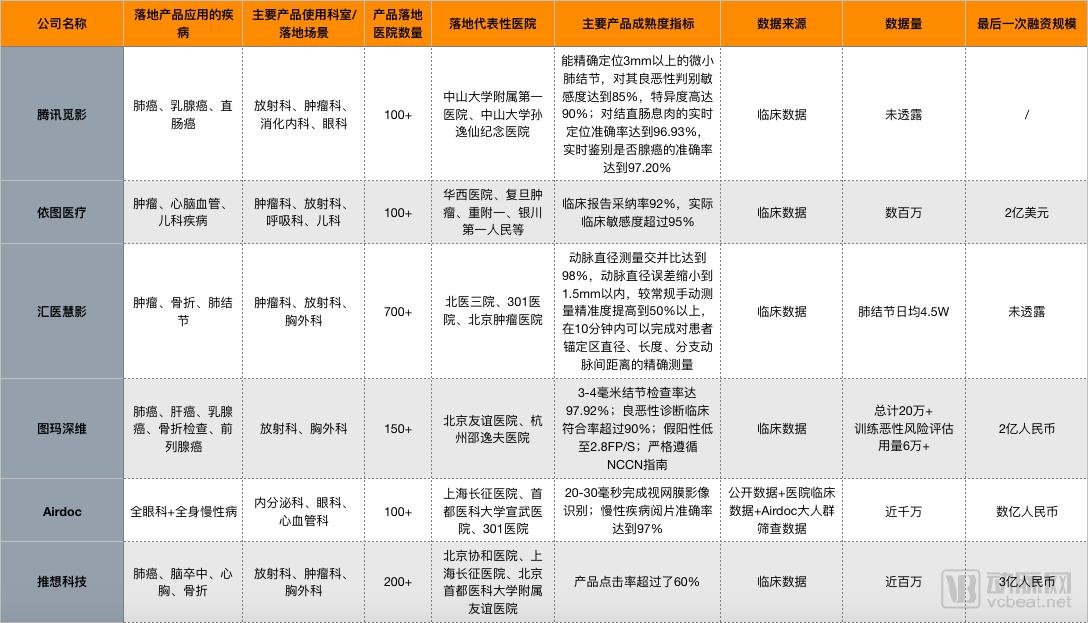
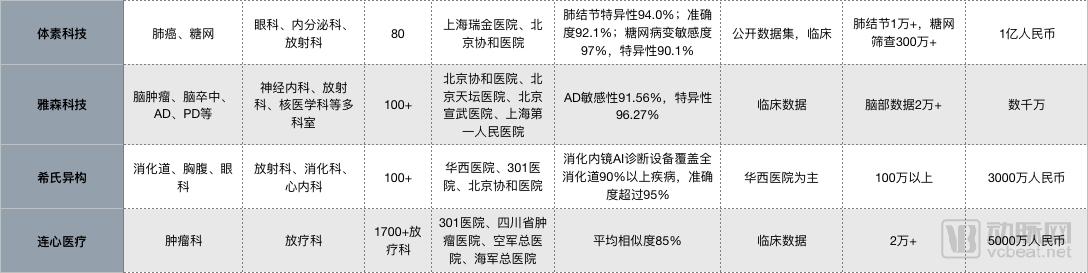
AI Product Landscape of Select Enterprises
(Data sourced from VCBeat and VCBeat Research Institute)
Liu Shiyuan, Director of the Department of Diagnostic and Interventional Radiology and Nuclear Medicine at Changzheng Hospital, provided a brief summary of the role of AI products in medical imaging. He believes that the impact of AI in medical imaging is multidimensional, primarily encompassing four key functions.
1. Lesion Detection: This is the primary quality metric for AI—AI must ensure accuracy to prevent missed diagnoses. Missed diagnoses often lead to medical disputes, and reducing the miss rate can mitigate medical risks.
2. Quantitative Analysis: Physicians’ evaluations and judgments are often subject to certain errors. If physicians can leverage artificial intelligence to perform fully or semi-automated quantitative analyses, the overall diagnostic accuracy will be improved. Meanwhile, the lesion quantification data processed and generated during the analysis, as well as the quantitative information required for treatment, hold substantial potential value.
3. Disease Diagnosis: After analyzing the available data, both machines and humans need to make judgments. For instance, the results of determining whether a tumor is benign or malignant are highly diverse, requiring the comprehensive application of various AI technologies to generate accurate diagnostic outcomes.
4. Treatment Planning: How should physicians administer treatment? How should therapeutic regimens be designed? How should clinical pathways be planned? These are critical questions that AI must thoroughly address in the future.
From a holistic perspective, existing AI imaging products span detection, quantification, diagnosis, follow-up, and prognosis, with a wide variety of specific offerings available.
In terms of detection and diagnosis, the most widespread application of AI is in the detection of pulmonary nodules. Currently, over a dozen products, including Miying, Infervision, and Huiyi Huiying, have reached maturity and have been submitted to the National Medical Products Administration (NMPA) for approval. AI applications in the nervous system have also begun to take shape. Companies such as Yasen, Nuono, and Yirui are leveraging their respective technologies to enable increasingly mature early screening and diagnosis of neurological disorders like Alzheimer’s disease and epilepsy, with corresponding products successfully implemented in hospitals. Orthopedic AI products primarily focus on fracture detection and bone age assessment; solutions from companies like Winning Health and Yitu can complete bone age tests within seconds. In the cardiovascular field, products from Shukun and Watson utilize AI to detect coronary heart disease. Regarding diabetic retinopathy, Airdoc has not only expanded its presence in hospitals but also partnered with Baodao Optical to meet users’ daily vision testing needs.
Follow-up and prognosis depend on the level of hospital informatization. Nowadays, medical informatics companies are increasingly adopting AI technologies. Researchers leverage deep learning, natural language processing (NLP), and other techniques to integrate relevant knowledge graphs, thereby providing comprehensive, intelligent, and efficient support for healthcare management and clinical decision-making.
However, regardless of the type of AI product, its purpose is to assist physicians rather than replace them.Computers are inevitably far superior to humans in memory and big data processing capabilities, but the technology required to surpass humans in comprehensive decision-making remains a distant prospect. Both domestically and internationally, enormous human and financial resources have been invested in the research of true artificial intelligence; yet, what has been achieved so far is merely the tip of the iceberg. The human neural network cannot be replicated by simple multi-layer structures, and many profound challenges remain. Without major breakthroughs in brain science, the notion that “AI will replace humans” is nothing short of a fantasy.
Just as health information systems had to navigate a tortuous path before taking root in hospitals, AI products are likewise traversing an arduous yet upward trajectory, with numerous challenges emerging one after another.
Lin Hui, Director of the Internet and Artificial Intelligence Office at Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, pointed out that interface issues are the first challenge encountered when integrating AI products into hospital systems.
“A similar phenomenon exists both domestically and internationally: when products are integrated with hospitals, the first hurdle encountered is interoperability with Hospital Information Systems (HIS). As a physician, I strongly hope that one day hospitals will migrate their systems to the cloud. This would enable us to connect numerous hospitals, promote the standardization and normalization of hospital HIS, truly integrate health data for the Chinese population, break down information silos, achieve interconnectivity between hospitals, and build a comprehensive ‘Healthy China.’”
When enterprises collaborate with hospitals, they often face risks related to data security, legal compliance, and intellectual property (IP) rights allocation. In particular, conflicts over IP rights allocation can critically constrain the enterprise party.
Therefore, when enterprises collaborate with hospitals, both parties must consider the strategic partnership agreements they sign, such as stipulating terms for data usage and selectively transmitting and receiving relevant data over the intranet based on research objectives. Data de-identification is a necessary procedure, and post-hoc data cleanup is also indispensable.
Unlike applications of computer vision in security, retail, and other fields, physicians bear responsibility for each patient. In the event of a missed or misdiagnosis, who is held accountable? A physician’s signature signifies their assumption of responsibility; but what if the physician’s signature is absent?
Secondly, taking fundus AI as an example, its training process relies on high-quality fundus image interpretation, with all relevant data sourced from the top hospitals in China. Given that images captured at primary care hospitals are of relatively lower clarity, will the technology face adaptation challenges when deployed at the grassroots level?
Finally, when AI becomes accustomed to processing typical cases, does it become confused by complex conditions involving multiple comorbidities? These are major challenges currently facing AI.
Lin Hui stated, “Before AI companies enter a specific medical niche, they must thoroughly assess the current state of healthcare services. It is widely recognized that although China’s healthcare system has made significant contributions to public health, the system itself is ailing—and seriously so. While it is common knowledge that accessing medical care is difficult and expensive, hospitals operate like bustling marketplaces, teeming with people. Doctors spend less than two minutes with each patient; can accurate diagnoses truly be made in such a brief window? In the course of diagnosis and treatment, perfunctory practices are all too common.”
“So, everyone knows that large hospitals are busy and doctors brush patients off. Why not go to primary care hospitals instead? This raises another question: Are these facilities reliable? As people place increasing importance on health, they will absolutely not entrust their lives to healthcare institutions they do not trust. Although primary healthcare service centers in major cities have seen an increase in patient volume, the vast majority of diagnosis and treatment centers remain nearly empty.”
Therefore, promoting the application of AI in primary care settings is not merely a matter of quality, but one of trust. Building patient confidence in primary care institutions and increasing the utilization rate of their equipment will require sustained effort and time.
Liu Shiyuan put forward five suggestions to all AI participants at the conference.
First, physicians need to articulate their needs, identify current pain points in clinical practice, clarify which types of products have potential demand, and guide R&D institutions in selecting research directions aligned with physicians’ priorities. From appointment scheduling and registration for examinations, to image interpretation and analysis, report generation, treatment efficacy evaluation, and follow-up, any product that can enhance physicians’ work experience and improve efficiency is highly necessary.
Second, once the model is established, physicians should serve as cultivators of AI. An AI model is akin to a newborn infant requiring nourishment. During this nurturing process, high-quality data is indispensable, and low-dimensional data is equally critical.
Third, there is currently a lack of quality control standards, and physicians should serve as both the developers and implementers of these standards. Physicians must be involved in establishing standards for data collection, image archival, and image quality. Furthermore, regulators and enterprises should also heed physicians’ input regarding disease distribution and composition issues involved in database construction.
Fourth, hospitals are the primary stakeholders in AI ethics issues, holding rights to data licensing, ownership, and privacy; accordingly, ethical standards must be developed through the joint participation of physicians, enterprises, and regulators.
Fifth, physicians and enterprises should serve as stewards and promoters of AI in medical imaging. In this process, physicians must avoid resistance, while enterprises must refrain from excessive promotion. Overhyped marketing by enterprises can mislead the public; when expectations are set too high but products fail to deliver, public confidence in AI solutions will rapidly decline, ultimately hindering industry development.
According to VCBeat, the National Institutes for Food and Drug Control (NIFDC) has received 30–40 product approval applications. Among these, products for diabetic retinopathy account for 32%, those for pulmonary nodules for 35%, X-ray-based products for 10%, endoscopy-related products for 10%, and other products for approximately 13%. Once disease-specific databases are established, regulatory approvals will be granted sequentially, accelerating commercialization. Consequently, capital investors have already begun positioning themselves in this sector.
Luo Shiming, a senior researcher at VCBeat Institute, has learned that, to date, there are no chargeable products for pulmonary nodules, whereas chargeable products have already emerged for diabetic retinopathy. The key difference between the two lies in their market entry models: the pulmonary nodule project enters hospitals under the guise of scientific research initiatives, while diabetic retinopathy screening meets the criteria of hospital fee schedules, enabling revenue sharing with hospitals. Specifically, the price per eye examination is RMB 33 in Chongqing and RMB 40 in Guangzhou. The daily screening volume can reach up to 5,000 cases, with the company’s revenue share accounting for approximately 50%.
Products for diabetic retinopathy have identified a precise entry point within existing medical catalogs, serving as an excellent case study. By the same token, artificial intelligence companies would do well to examine hospital fee schedules; those who are attentive may uncover new opportunities.
As artificial intelligence has evolved to its current stage, companies rarely discuss specificity and sensitivity anymore; instead, they focus on the level of productization. Trained on vast amounts of existing data, the accuracy and specificity of products from various enterprises have become very similar. In the general field of AI, iFlytek and Sogou have already opened their APIs to the public, allowing users to access them for a small fee, and image recognition will follow the same trend.
Once artificial intelligence reaches a certain stage of development, medical AI will become a foundational societal capability. The fundamental reason it has not yet achieved this status lies in the storage and organization of existing medical data, which constitute the critical bottleneck restricting its advancement. However, we cannot completely resolve this issue in the short term.