Global Trends in Cancer Immunotherapy: 417 Targets and 3,394 Active Programs (Including Approved Therapies)
Editor's Note: This article is reprinted fromCPhI Online (ID: cphi_cn), Author: Weiyi. Republished by VCBeat with authorization.
On October 19, the Cancer Research Institute (CRI) once again released its survey report on “Global Trends in Cancer Immunotherapy Development,” published in the journal Nature Reviews Drug Discovery. Within one year, the number of global cancer immunotherapy projects increased by 67%, the number of targets rose by 50%, and the number of companies and institutions with clinical development programs grew by 42%, underscoring the vigorous growth of cancer immunotherapy.
In 2011, the approval of ipilimumab for the treatment of melanoma marked the beginning of a revolution in cancer immunotherapy and has gradually transformed the paradigm of cancer treatment. To date, 11 new cancer immunotherapies have been approved and have become the standard of care for various types of cancer.
The New York Cancer Institute, a non-profit organization dedicated to cancer immunotherapy research for over 65 years, conducted a comprehensive survey of the global landscape of tumor immunotherapy in 2017 (Ann. Oncol. 29, 84-89; 2017). One year later, it undertook another large-scale survey. In this report, the research team compares these two surveys and provides a longitudinal analysis of global trends in tumor immunotherapy.
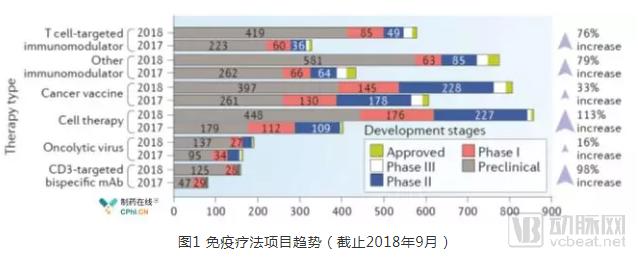
Over the past year (September 2017–September 2018), the number of global immunotherapy R&D projects increased by 67% (2,031 projects in 2017 vs. 3,394 projects in 2018). Immunotherapeutic agents can be categorized into six classes based on their distinct mechanisms of action:
• Targeted T-cell immunomodulators (e.g., monoclonal antibodies against PD-1 or CTLA-4);
• Other immunomodulators (e.g., agonists of TLR or interferon-α/β receptor 1 (IFNAR1));
• Tumor vaccines (e.g., Bacillus Calmette-Guérin (BCG) vaccine);
• Cell therapies (e.g., chimeric antigen receptor (CAR) or T-cell receptor (TCR) T-cell therapies);
• Oncolytic viruses (e.g., T-Vec);
• CD3-targeted bispecific antibodies (e.g., blinatumomab).
Among the six major categories of immunotherapy, cell therapy has demonstrated the fastest R&D growth rate at 113%, whereas oncolytic viruses saw a modest increase of only 16%. Meanwhile, cell therapy has surpassed cancer vaccines to become the largest segment in tumor immunotherapy, with 864 projects under development, accounting for 25% of all oncology immunotherapy projects. Furthermore, preclinical drug candidates increased by 97% (from 1,067 to 2,071), and drugs in clinical stages grew by 34% (from 964 to 1,287), indicating a continuous rise in both basic and preclinical innovative research.
There are currently 417 targets in global oncology immunotherapy projects. Over the past year, the number of immunotherapy targets increased by 50% (see attached table). Interestingly, in 2017, half of the R&D projects were concentrated on the top 23 targets, whereas in 2018, half of the R&D projects were focused on the top 48 hot targets (see attached table). Typically, once a drug targeting a specific target is approved, the number of corresponding R&D projects tends to decrease (Figure 2). For example, although the number of cell therapies increased by 113% in 2018, CD19-targeted cell therapies increased by only 37%.
In contrast, the number of investigational drugs targeting neoantigens (targets identified through bioinformatic analysis of individual patients’ tumors) increased by 133% within one year. The rise in the number of tumor immunotherapy targets may lead to the approval of more immunotherapies in the future. Notably, the actual number of drugs targeting non-specific tumor-associated antigens (TAAs) has decreased, indicating that the field is moving toward greater precision (Figure 3).
Figure 2. Top 15 Targets for Immunotherapy
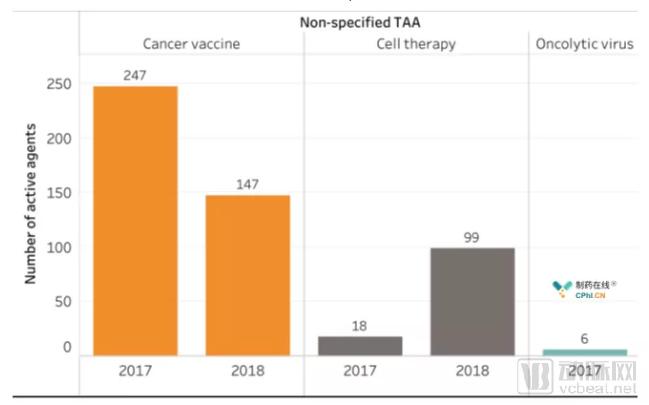
Figure 3. Trends in Non-Specific Tumor-Associated Antigen Items
In September 2017, 964 oncology immunotherapy drugs from 461 organizations (including pharmaceutical companies and institutions) had entered clinical stages (including those that had completed clinical trials). One year later, 655 organizations were conducting clinical development of 1,287 drugs. This indicates that while the number of drugs in clinical stages increased by 34%, the number of enterprises and institutions engaged in clinical drug development rose by 42% (Figure 4). A comparison of the top 15 organizations by number of clinical projects revealed an addition of 36 new drugs within one year, representing a 20% increase. More importantly, Big Pharma continued to dominate the landscape of clinical projects, occupying the top eight positions by project count. Four research institutions ranked among the top 15 in clinical projects, three of which were Chinese entities: the Shenzhen Institute of Immune Gene Therapy, the 301 Hospital (Chinese PLA General Hospital), and the First Affiliated Hospital of Army Medical University (formerly Third Military Medical University). The strong performance of Chinese institutions benefited from the vigorous development of cell therapy in China [Translator’s Note].
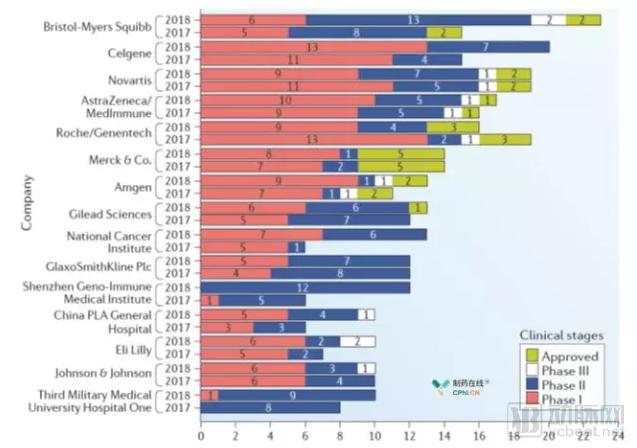
Figure 4 Top 15 Immunotherapy Companies and Institutions
Through new survey analysis, the number of global oncology immunotherapy projects increased by 67%, the number of targets increased by 50%, and the number of companies and institutions engaged in clinical drug development rose by 42% within one year. This substantial growth underscores our strong enthusiasm and confidence in the development of oncology immunotherapy drugs.
The research team considers this optimistic outlook to be justified. First, since the previous survey in 2017, a total of 10 projects have received FDA approval within one year, including two CAR-T therapies, eight PD-1 and PD-L1 antibody drugs, and one CD3-targeted bispecific antibody.
Secondly, since 2011, new immunotherapies have not only become the standard of care for 15 types of cancer but also the first-line treatment for melanoma, lung cancer, and renal cell carcinoma, establishing immunotherapy as one of the pillars of cancer treatment.
Third, immunotherapies, such as anti-PD-1 and anti-PD-L1 agents, are also rapidly entering major markets beyond the United States, Europe, and Japan; for example, China has recently approved nivolumab and pembrolizumab.
Finally, extensive clinical studies have demonstrated that immunotherapy provides durable survival benefits for patients, offering the hope of a cure for certain cancer types. However, caution is warranted when translating promising advances in cancer immunology into effective cancer immunotherapies. The recent failures or terminations of multiple Phase III trials evaluating indoleamine 2,3-dioxygenase 1 (IDO1) inhibitors serve as a reminder that drug development is a highly risky endeavor.
Looking ahead, scientific evidence should guide the development of oncology immunotherapy drugs. For instance, all eligible cancer trials should employ biomarkers to screen for patients most likely to benefit from appropriate novel cancer immunotherapies. Furthermore, relevant research should be maximally integrated into all clinical trials so that we can learn from both successful and failed trials. This will enable each clinical trial and every patient volunteer to make a greater contribution to our pursuit of cancer treatments.