Robotic Applications in Lung Cancer Diagnosis and Treatment: Market Overview and Innovative Product Landscape
Editor’s Note: This article is reprinted fromSiyu MedTech Observer (WeChat Official Account: suribot), Author: Liu Jixuan. Reposted with permission from VCBeat.
Lung cancer is one of the malignant tumors with the fastest growing incidence and mortality rates, posing the greatest threat to public health and life.
According to data from the National Cancer Center of China, lung cancer accounts for over 35% of all cancer-related deaths. The incidence is higher in men than in women. Most cases occur in individuals aged over 40, with the highest prevalence observed among those aged 50–70. Lung cancer often presents no obvious symptoms in its early stages, and 75% of patients are diagnosed at an advanced stage.
With the aging population, the number of elderly patients with lung cancer is continuously increasing. Due to factors such as declined pulmonary function, reduced hepatic reserve and renal clearance capacity, diminished bone marrow hematopoietic function, and the presence of multiple age-related comorbidities, elderly cancer patients often exhibit low treatment tolerance and are prone to complex and diverse clinical conditions during therapy. Research on immunotherapy, surgical techniques, and device-related innovations for lung cancer is of great significance and represents a critical challenge that must be addressed to advance China’s future medical technology and healthcare standards.
Recently, Intuitive Surgical, the pioneer of surgical robotics, and Fosun Pharma have officially launched a strategic partnership, jointly investing $100 million to establish a joint venture in Shanghai dedicated to the research and development of innovative products for the early diagnosis and treatment of lung cancer. Meanwhile, numerous innovative enterprises are also entering this field. The emerging battlefield of robotic systems for lung cancer is poised for intense competition. Siyu Medical Device Observer has provided an overview of these developments.
Tissue biopsy is essential for the precise treatment of lung cancer. However, traditional manual tissue biopsy techniques have various limitations, leading to the emergence of robotic systems designed to assist with biopsies. Pioneers in this field include I-SYS, SimpliCT, ROBIO EX, and Medtronic’s Super Dimension Navigation system.
(1) Puncture Robot
The iSYS system from Austria’s Interventional System GmbH is a novel, compact robotic targeting system designed to assist in interventional radiology procedures. Radiologists use a handheld joystick for remote control, enabling them to operate at a safe distance from the radiation beam while utilizing real-time fluoroscopic navigation guidance.
iSYS1 enables radiologists to pre-plan needle trajectories prior to procedures. Its accuracy and precision are certified, ensuring reliable reproducibility. The user interface is highly intuitive and user-friendly, and the system is compatible with any CBCT (Cone-Beam Computed Tomography) or C-Arm platform. The system is quick and easy to use, with setup completed within three minutes.
iSYS System Diagram
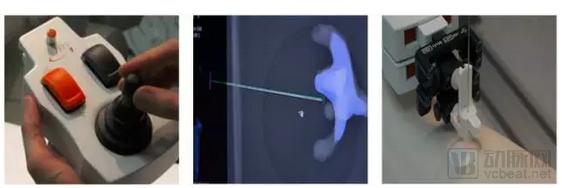
Norwegian company NeoRad’s SimpliCT system is an interventional laser navigation device for CT, PET-CT, and cone-beam CT (CBCT), used for non-vascular interventions such as biopsy, ablation, drainage, and infiltration. SimpliCT uses laser beams to significantly improve the accuracy of computed tomography (CT/CBCT)-guided puncture procedures and can reduce radiation exposure for both operators and patients.
SimpliCT is installed using the Mavig Portegra2 ceiling-mounted system, enhancing patient comfort with faster and safer procedures. SimpliCT’s laser navigation system is currently marketed and promoted in the United States, the European Union, Japan, South Korea, Taiwan, Singapore, Australia, as well as many countries in the Middle East and South America.
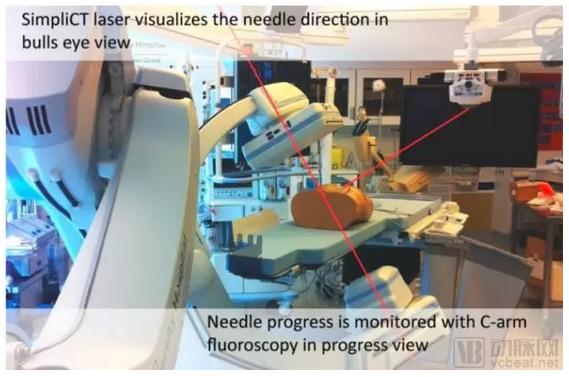
SimpliCT System Diagram
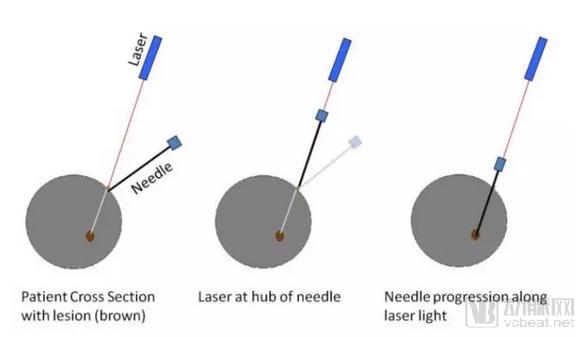
SimpliCT System Laser Positioning Diagram
Perfint Healthcare’s ROBIO EX system is a CT- and PET/CT-guided robotic positioning system designed for interventional procedures in the thorax and abdomen. It facilitates rapid and accurate tumor targeting and instrument placement, with specific applications including tissue biopsy, fine-needle aspiration cytology (FNAC), pain management, drainage, and tumor ablation.
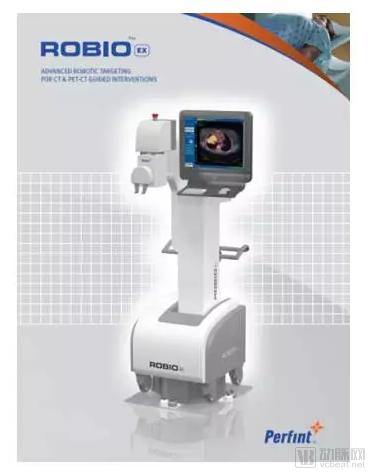
The robotic arm of ROBIO EX features 5 degrees of freedom with sub-millimeter and sub-angular precision, ensuring that surgical procedures can be performed at varying heights and positions.
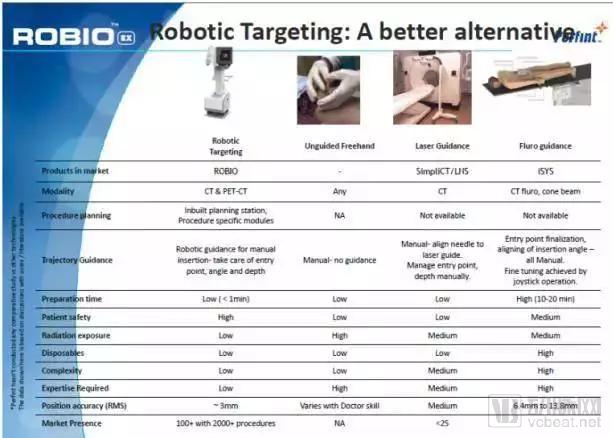
Comparison of Several Puncture Robots
Bronchoscopy plays a pivotal role in the early diagnosis of lung cancer. Conventional bronchoscopy is primarily suitable for diagnosing central-type lung cancer, whereas autofluorescence bronchoscopy, which integrates cell spontaneous fluorescence and computerized image analysis, offers certain advantages in detecting early mucosal and submucosal lesions. For mediastinal or peripheral lung cancer, endobronchial ultrasonography (EBUS), which has emerged in recent years, demonstrates excellent diagnostic efficacy. Depending on the type of ultrasound probe, EBUS is categorized into radial probe (RP) and convex probe (CP). RP-EBUS is mainly used to examine peripheral lesions (located in bronchi below the subsegmental level), while CP-EBUS is primarily employed for the examination and diagnosis of mediastinal lymph nodes. When combined with endoscopic ultrasound via the esophagus, it enables accurate needle aspiration of most mediastinal lymph nodes.
(II) Electromagnetic Navigation Bronchoscopy Robotic System
Electromagnetic Navigation Bronchoscopy (ENB) is the latest generation of bronchoscopic navigation technology. By integrating electromagnetic navigation, virtual bronchoscopy, and three-dimensional reconstruction of CT images, it enables real-time navigation and significantly improves the accuracy of biopsies. This technique is primarily indicated for peripheral lesions that cannot be definitively diagnosed using conventional bronchoscopy or percutaneous lung biopsy. Currently, its applications are gradually expanding to include assistance in surgical localization, radiotherapy planning, and ablation therapy under precise navigation for patients with peripheral lung cancer who are no longer candidates for surgery.
Medtronic’s Super Dimension Navigation System employs electromagnetic navigation bronchoscopy (ENB) technology to visualize the tracheobronchial tree, assisting physicians in guiding endoscopic tools or lung access catheters and placing markers within soft lung tissue. The system comprises a navigation system, a localization board, a patient triplet, a localization catheter, and an extended working channel for the endoscope. The Super Dimension Reach System constructs a three-dimensional (3D) image using the patient’s computed tomography (CT) scans. This 3D image is used to plan a pathway from the airways to potential suspected lesions and provides feedback as the tip of the localization catheter traverses the planned path. The system operates by having the localization board emit electromagnetic signals, which are detected by electromagnetic sensors on the localization catheter and three sensors on the patient triplet. Once the localization catheter reaches the target location, it is removed, while the extended working channel remains in place, allowing other instruments to access the site.
Medtronic superDimension Electromagnetic Navigation Bronchoscopy (ENB)
Since the 1990s, with advancements in thoracoscopic equipment and high-definition imaging technologies, minimally invasive thoracoscopic surgery for lung cancer has become one of the most widely used surgical approaches in clinical practice. Due to advantages such as a low incidence of postoperative complications, shorter hospital stays, and faster recovery, it has replaced most open thoracotomies. Surgical incisions have gradually evolved from the initial four-port approach to three-port, two-port, single-port, and subxiphoid single-port thoracoscopic procedures. Surgical techniques have progressed from traditional lobectomy to more precise anatomical lobectomy and sublobar resections (segmentectomy and wedge resection), as well as totally thoracoscopic sleeve lobectomy and double-sleeve lobectomy involving both bronchial and vascular reconstruction.
Robot-assisted surgery has emerged as the advanced representative of minimally invasive lung cancer surgery under total thoracoscopy. Minimally invasive surgery offers significant advantages in lung cancer treatment, including minimal trauma, reduced blood loss, faster recovery, shorter hospital stays, and lower postoperative complication and mortality rates, gradually becoming the preferred surgical approach for lung cancer. Minimally invasive surgery encompasses two distinct techniques: Video-Assisted Thoracoscopic Surgery (VATS) and the da Vinci Robotic Surgical System.
(I) Video-Assisted Thoracoscopic Surgery (VATS)
Video-assisted thoracoscopic surgery (VATS) was first used in the early 20th century for the treatment of pulmonary tuberculosis, at which time thoracoscopic techniques were not yet applicable to lobectomy for lung cancer. With advancements in optics and instrumentation, thoracoscopic technology has been gradually applied to the treatment of lung cancer, leading to the emergence of single-port VATS. The primary instruments for VATS include the thoracoscope, miniature camera, light source, video monitor, electrocautery knife, ultrasonic scalpel, linear stapler, long electrocoagulation hook, and ENDO-GIA cutting stapler, among others, along with conventional thoracic surgical instruments. A 5-mm, 30-degree thoracoscope is commonly used to facilitate better visualization of the spatial relationships among intrathoracic organs and tissues. Articulating, rotatable-head staplers are frequently employed, as they allow for more convenient manipulation under thoracoscopy by directly targeting the tissue, thereby reducing operative time.
Currently, the diameter of the operating handles of thoracoscopic surgical instruments may interfere with faster and better surgical maneuvers in single-port procedures. With technological advancements, thinner operating instruments may be designed in the future. At the 2015 ASCVTS meeting, researchers introduced a 5-mm vessel sealer; if such a device becomes commercially available, it will undoubtedly significantly promote the development of single-port video-assisted thoracoscopic surgery.

Video-Assisted Thoracoscopic Surgery (VATS)
(II) da Vinci Robotic Surgical System
1. Overview of the da Vinci Surgical Robot System
The da Vinci Surgical System represents the first true robotic participation in lung cancer surgery. Manufactured by Intuitive Surgical, it became the world’s first robotic surgical system approved for formal use in operating rooms after receiving FDA clearance in July 2000. The da Vinci system consists of three components: the surgeon console, the patient-side cart with robotic arms, and the vision system. The lead surgeon sits at the console, located outside the sterile field of the operating room, and uses both hands (via two master controllers) and feet (via foot pedals) to control the surgical instruments and a three-dimensional high-definition endoscope.
The Patient Cart is the operational component of a surgical robot, primarily designed to support the instrument arms and camera arm. An assistant surgeon works alongside the Patient Cart within the sterile field, responsible for exchanging instruments and the endoscope, and assisting the lead surgeon in completing the procedure. The Video Cart houses the core processor and image processing equipment of the surgical robot. The robot’s endoscope features a high-resolution three-dimensional (3D) lens that provides more than 10x magnification of the surgical field, delivering clear, three-dimensional HD images of the patient’s body cavity to the lead surgeon. This enables the lead surgeon to better judge operating distances and identify anatomical structures compared with conventional laparoscopic surgery, thereby enhancing surgical precision.

da Vinci Surgical System
The da Vinci Surgical System innovatively applies the concept of seamless human-machine integration, significantly enhancing the overall standard of minimally invasive surgery, and has been widely adopted in fields such as thoracic surgery. The use of this system for thoracic surgical procedures was approved by the U.S. Food and Drug Administration (FDA) on March 5, 2001, marking a relatively late start to its clinical application. Currently, only a few countries, including the United States, Italy, and Japan, permit the use of the da Vinci Surgical System for general thoracic surgeries. In China, the system was first introduced in 2006 by the Chinese People's Liberation Army General Hospital in Beijing, where it was primarily applied to cardiac surgeries by Professor Gao Changqing.
The da Vinci robotic system has now evolved to the sixth-generation SP (Single Port) system. Its most distinctive feature is the use of a single robotic arm, which can accommodate three multi-jointed instruments and one 3D HD camera, enabling visual control within narrow surgical spaces. Furthermore, improvements have been made in areas such as streamlined setup, multiple control modes, and dynamic information display. Through a specialized cannula, one camera arm and two crossable, articulating instrument arms are introduced into the body cavity to perform surgery, thereby allowing all procedures for lung cancer surgery to be completed through just a small incision in the chest wall.
In China, the da Vinci robotic surgical system is utilized in general thoracic surgery to perform procedures including: resection of anterior and posterior mediastinal tumors (both cystic and solid), total thymectomy with anterior mediastinal fat clearance, repair of diaphragmatic hiatus hernia, Heller myotomy, enucleation of intramural esophageal cysts with esophageal mucosal suture repair, radical esophagectomy for esophageal cancer, bullectomy, segmentectomy, wedge resection of pulmonary lesions or lobectomy for lung cancer, and lymph node dissection.

da Vinci Surgical Robot System
The da Vinci robotic surgical system offers advantages over traditional thoracoscopic surgery primarily in the following aspects.
(1) Greater surgical precision. The robotic system is equipped with a high-resolution 3D endoscope that provides 10–15x magnification, and its robotic arms measure only 5 or 8 millimeters in diameter—more dexterous than human fingers—thereby achieving a qualitative leap in surgical accuracy.
(2) Patients experience less trauma and faster recovery. During the procedure, the robotic arms create smaller incisions on the patient's body surface, resulting in less blood loss, reduced intraoperative tissue trauma and inflammatory response, decreased postoperative pain, shortened hospital stays, and improved quality of life.
(3) Greater flexibility and convenience for surgeons. The da Vinci Surgical System expands the surgeon’s field of view; its instrument wrists enable dexterous articulation within the patient’s body, allowing manipulation from multiple angles. It also reduces hand tremor and surgeon fatigue, thereby enhancing focus during procedures. These represent significant advancements not available with conventional thoracoscopy.
2. Market Overview of the da Vinci System
As of September 30, 2013, a total of 2,871 da Vinci Surgical Systems had been sold worldwide, including 2,042 in the United States, 455 in Europe, 261 in Asia, and 113 in other regions. In Asia, the breakdown was as follows: South Korea (39 units), Japan (138 units), India (23 units), Mainland China (17 units), Hong Kong (8 units), Taiwan (18 units), Singapore (8 units), Malaysia (3 units), Thailand (6 units), the Philippines (1 unit), and Indonesia (1 unit).
Since the introduction of the da Vinci Surgical System by the Chinese People's Liberation Army (PLA) General Hospital in 2006, mainland China had acquired a total of 17 units by the end of June 2013. Among these, the PLA General Hospital in Beijing held four units. The following institutions each possessed one unit: Beijing Ditan Hospital, the PLA Second Artillery General Hospital in Beijing, Ruijin Hospital affiliated with Shanghai Jiao Tong University School of Medicine, Shanghai Chest Hospital affiliated with Shanghai Jiao Tong University, Huadong Hospital affiliated with Fudan University, Zhongshan Hospital affiliated with Fudan University, Nanjing General Hospital of the Nanjing Military Command, Southwest Hospital affiliated with the Third Military Medical University, the General Hospital of the Shenyang Military Command, Shanghai Changhai Hospital, Peking Union Medical College Hospital, the General Hospital of the Jinan Military Command, and Xijing Hospital affiliated with the Fourth Military Medical University. The General Hospital of the Shenyang Military Command was currently the only institution in Northeast China equipped with the da Vinci Surgical System.
In 2012, approximately 450,000 surgical procedures were performed worldwide using the da Vinci Surgical System, representing an increase of over 25% compared to 2011. In China, a total of 6,535 da Vinci robotic surgeries were conducted from 2006 to December 2013, with 2,984 procedures performed between January and December 2013 alone. This demonstrates the remarkably rapid development and adoption of the da Vinci robotic system.
3. Status of Da Vinci Thoracic Surgery in China
Due to the high technical difficulty of performing da Vinci robot-assisted lobectomy and lymph node dissection for lung cancer, proficiency in conventional open thoracotomy lobectomy as well as skilled application of complete video-assisted thoracoscopic surgery (VATS) lobectomy is required. Consequently, the implementation of this surgical approach presents significant challenges. According to incomplete data, only a few hospitals in China are currently capable of performing da Vinci robot-assisted lobectomy and lymph node dissection for lung cancer, including the Chinese PLA General Hospital, the General Hospital of Shenyang Military Command, Shanghai Chest Hospital affiliated with Shanghai Jiao Tong University, the General Hospital of Nanjing Military Command, and Southwest Hospital affiliated with the Third Military Medical University.
From 2006 to the end of December 2013, a total of 607 general thoracic surgical procedures were performed using the da Vinci Surgical System in China, accounting for 9% of all da Vinci surgeries across various specialties. The number of procedures by hospital was as follows: General Hospital of Shenyang Military Command, 260 cases; General Hospital of Nanjing Military Command, 191 cases; Shanghai Chest Hospital affiliated with Shanghai Jiao Tong University, 70 cases; General Hospital of the Second Artillery Corps of the Chinese People's Liberation Army in Beijing, 49 cases; Chinese PLA General Hospital in Beijing, 11 cases; Zhongshan Hospital affiliated with Fudan University and Southwest Hospital affiliated with the Third Military Medical University, 9 cases each; General Hospital of Jinan Military Command, 6 cases; Huadong Hospital affiliated with Fudan University and Shanghai Changhai Hospital, 1 case each.
Over the past three decades, continuous updates to radiotherapy equipment and related auxiliary devices have driven rapid advancements in radiation therapy techniques. Clinical radiation therapy has evolved from initial two-dimensional irradiation to current three-dimensional conformal radiation therapy (3DCRT) and intensity-modulated radiation therapy (IMRT), as well as derived technologies such as image-guided radiation therapy (IGRT) and adaptive radiation therapy (ART). These innovations in radiotherapy have, to some extent, altered the role of radiation therapy in the comprehensive treatment of lung cancer.
In the late 1990s, stereotactic ablative radiotherapy (SABR) for thoracic tumors gradually began to be applied in clinical research, with 5-year survival rates exceeding 50%. For patients with stage I non-small cell lung cancer (NSCLC) who are medically fit for surgery but refuse it, SABR can achieve therapeutic outcomes comparable to surgery if the radiation biological effective dose (BED) exceeds 100 Gy. A 2015 pooled analysis of two studies comparing SABR with lobectomy (STARS and ROSEL), published in *Lancet Oncology*, included a total of 58 patients; the 3-year survival rates were 79% in the surgical group and 95% in the SABR group. Currently, SABR is primarily used for the treatment of peripheral lung cancers and small-volume lung cancers (maximum tumor diameter < 5 cm).
Varian Medical Systems, Inc. is currently a global supplier of integrated hardware and software for radiotherapy equipment, as well as key hardware and software for X-ray diagnostic devices. Committed to providing equipment and related software for radiation therapy, radiosurgery, proton therapy, and brachytherapy for cancer and other diseases, Varian is a leading global provider of diagnostic and therapeutic solutions for cancer and other major diseases. To date, Varian has installed more than 7,000 radiotherapy systems worldwide, accounting for nearly 70% of the global market share. Varian’s TrueBeam™ linear accelerator and the Calypso® “GPS for Cancer” tumor localization system are the stereotactic ablative radiotherapy systems with the highest market share globally.

China’s research and development of robotics for lung cancer is still in its early stages. Given the rapid advancement of artificial intelligence in the country, robotic applications related to lung cancer are primarily focused on image interpretation and diagnosis.
iFlytek Co., Ltd. and Anhui Provincial Hospital have jointly developed an imaging recognition robot through their collaborative Medical Artificial Intelligence Laboratory. This robot can analyze lung CT scans to detect inflammation or cancer. Currently, it is being used in clinical trials, with a recognition accuracy rate exceeding 95%.

iFlytek Lung Cancer Imaging Diagnosis and Film Reading Robot
True Health (Beijing) Medical Technology Co., Ltd. was jointly initiated by multiple institutions, including Beihang University, Tsinghua University, and the Chinese Academy of Sciences. Focusing on the diagnosis and treatment of lung cancer in China, the company leverages artificial intelligence to achieve precise early diagnosis and precision surgery for lung cancer. It has developed an automated diagnostic and surgical robotic system for pulmonary nodules, which integrates robotic navigation and control technologies with big data-based automatic segmentation and 3D reconstruction. This system assists physicians in automatically diagnosing pulmonary nodules and navigating precisely to the preoperatively planned surgical site. The prototype has already been manufactured, achieving a positioning accuracy of 1 mm, and preparations for clinical trials are imminent.
Suzhou Anshu Medical Co., Ltd. is a specialized high-tech company that independently develops intelligent robotic systems for ablation surgery assistance. It is the first company in China to provide precise puncture ablation technology, successfully breaking through the bottlenecks of traditional tumor ablation procedures and offering surgical treatment possibilities for patients with advanced-stage lung cancer. The company is currently the first in China to successfully develop a tumor ablation robotic system, which holds significant future market potential and has completed the prototype development phase.
Driven by advancements in robotics and the growing demand for minimally invasive procedures among cancer patients, the robotics market for lung cancer care boasts broad development prospects. Whether in surgical robots for lung cancer, robotic systems for early diagnosis, or robotic stereodynamic ablative radiotherapy, China still lags behind major developed countries in Europe and the United States. Time is needed to cultivate domestic companies with independent intellectual property rights and full-industry-chain capabilities in lung cancer robotics. Nevertheless, this sector remains a blue ocean. Domestic innovative companies that have identified these opportunities are rapidly catching up, and in certain areas, they are already on par with top-tier global medical device manufacturers.