Professor Zhou Jianying of the First Affiliated Hospital, Zhejiang University: Telemedicine Is the Highlight of Internet Hospitals and Plays a Vital Role in Primary Respiratory Disease Prevention and Control
In China, the overall mortality rate from chronic diseases is on the rise. The four most common chronic diseases are cardiovascular and cerebrovascular diseases, chronic respiratory diseases, diabetes, and cancer. Standardized diagnosis and treatment for cardiovascular and cerebrovascular diseases and diabetes have already been widely implemented at the primary care level, whereas the development of primary care services for chronic respiratory diseases has only gradually advanced in recent years.
From November 16 to 18, 2018, the Third China Academic Forum on Prevention and Control of Respiratory Diseases in Primary Care was held in Hangzhou. Professor Zhou Jianying, Director of the Department of Respiratory and Critical Care Medicine and Director of the Center for Diagnosis and Treatment of Pulmonary Diseases at The First Affiliated Hospital, Zhejiang University School of Medicine (hereinafter referred to as “FAHZU”), National Standing Committee Member of the Respiratory Disease Branch of the Chinese Medical Association, and Deputy Leader of the Lung Cancer Group under the Respiratory Disease Branch of the Chinese Medical Association, delivered a keynote speech titled “Prevention and Control of Respiratory Diseases in Primary Care in the Internet Era.” VCBeat has compiled Professor Zhou Jianying’s keynote address.
In her keynote address, Professor Zhou Jianying presented the following views:
1. There is still a long way to go in achieving effective interoperability between primary care and tertiary hospitals for the diagnosis and treatment of chronic respiratory diseases;
2. The role of primary care physicians in the diagnosis and treatment of chronic respiratory diseases is crucial;
3. The proportion of COPD patients seeking care at primary healthcare institutions needs to be increased;
4. Telemedicine is the standout feature of internet hospitals;
5. Internet hospitals have ushered in the era of smart healthcare.
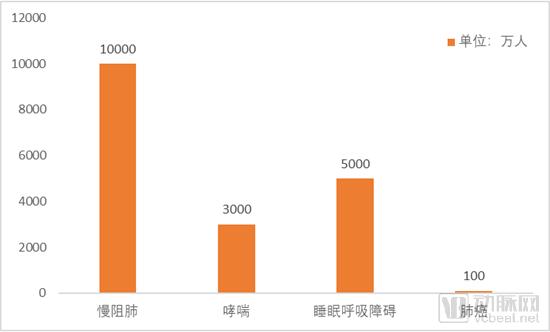
Currently, the mortality rate from chronic respiratory diseases is very high among individuals under the age of 70. Chronic respiratory diseases include chronic obstructive pulmonary disease (COPD), bronchial asthma, sleep-disordered breathing, and malignant lung tumors. Among these, the prevalence of COPD in individuals aged 40 and above exceeds 13.7%, with the number of patients reaching as high as 100 million, making it the most prevalent respiratory disease in community-based management. Globally, there are at least 300 million asthma patients, with approximately 30 million in China. There are about 50 million patients with sleep-disordered breathing in China. Lung cancer has an annual incidence of approximately 800,000 cases, ranking first among all cancers. It is projected that by 2025, the annual incidence of lung cancer in China will approach 1 million, making China the country with the highest burden of lung cancer worldwide.
Source: Chinese Journal of General Practitioners
Note: The number of lung cancer patients is estimated based on annual new cases and the 5-year survival rate.
Data show that chronic obstructive pulmonary disease (COPD) is the third leading cause of death among Chinese residents. Sleep-disordered breathing, a major underlying condition contributing to hypertension, coronary heart disease, diabetes, and stroke, has not yet received sufficient attention and should be prioritized in community-based disease management. Furthermore, lung cancer early screening programs suitable for implementation at primary healthcare facilities are of great significance for improving the five-year survival rate of lung cancer patients.
However, the implementation of diagnosis and treatment for chronic respiratory diseases at the primary care level in China is far from satisfactory, particularly with regard to chronic obstructive pulmonary disease (COPD).
On one hand, chronic obstructive pulmonary disease (COPD) has a high prevalence but a low diagnosis rate. Due to the low penetration of pulmonary function testing in the healthcare system, the COPD diagnosis rate in China is only 35.1%, with merely 6.5% of patients having undergone pulmonary function testing. On the other hand, treatment adherence among COPD patients is very low. Data show that less than one-quarter of patients receive treatment, and among those with Stage II or higher COPD, only 7.9% adhere to regular medication regimens. In a questionnaire survey involving 1,698 patients across 11 hospitals nationwide, 23.1% of patients reported self-adjusting their medications, while 28.1% stated that they did not follow medical advice regarding medication use.
Furthermore, there is a lack of systematic management for patients with chronic obstructive pulmonary disease (COPD) during the stable phase. This is specifically manifested by the low proportion of patients who transition to outpatient care for regular treatment following an acute exacerbation. An analysis based on the 2014 national medical insurance database revealed that only 30% of patients in China were transferred to outpatient clinics for regular treatment after an acute exacerbation.
The stark contrast in the average number of patient visits between primary healthcare institutions and hospitals further underscores the challenges China faces in the diagnosis and treatment of chronic respiratory diseases at the primary care level. Taking 2014 as an example, there were 917,000 primary healthcare institutions, with an average of 5,000 patient visits per institution; in contrast, there were 26,000 hospitals, with an average of 115,000 patient visits per hospital.
Professor Zhou Jianying believes that there is still a long way to go to truly achieve effective interoperability between primary care institutions and higher-level medical facilities in the diagnosis and treatment of chronic respiratory diseases.
Professor Zhou Jianying pointed out that in the management of chronic respiratory diseases, primary care physicians are usually the first point of contact and are most likely to detect patients with chronic obstructive pulmonary disease (COPD) at an early stage. Specifically, first-contact physicians should play a role in three aspects: first, smoking cessation counseling; second, pulmonary function testing; and third, diagnosis and referral. Professor Zhou emphasized that first-contact physicians play a crucial role in the management of COPD, and the proportion of COPD patients seeking care at primary healthcare institutions should be increased.
However, at the grassroots level of medical institutions, while tests such as electrocardiograms and blood pressure measurements are relatively widespread, the implementation of pulmonary function testing remains weak. Primary care practitioners face institutional barriers in fully assuming the role of first-contact physicians. As one moves further down the healthcare hierarchy, the scope of practice for physicians becomes broader. At the level of designated community medical institutions, there are no longer specialists but rather family doctors; yet, the number of family doctors conducting pulmonary function tests is limited. At township health centers, pulmonary function testing is basically not performed.
Internet-Connected Diagnosis and Treatment of Chronic Respiratory Diseases
High prevalence, low diagnosis rate, poor compliance, and uneven distribution of medical resources undoubtedly constitute bottlenecks in the diagnosis and treatment of chronic respiratory diseases.
At the policy level, in 2016, chronic respiratory diseases were included for the first time in the selection and review criteria for National Chronic Disease Demonstration Zones. In 2017, chronic respiratory diseases (specifically chronic obstructive pulmonary disease, COPD) became the third chronic condition, following hypertension and diabetes, to be incorporated into pilot programs for tiered diagnosis and treatment.
Professor Zhou Jianying believes that, with the support of the National Health and Family Planning Commission, efforts to prevent and control chronic respiratory diseases should be further extended to the grassroots level, particularly in remote areas, and that the internet can provide effective means to address bottlenecks at this level.
First, the Internet facilitates the implementation of tiered diagnosis and treatment for chronic respiratory diseases. Within this tiered system, specialists, general practitioners, and health managers are assigned distinct responsibilities. Specialists are responsible for clinical consultation, pulmonary function screening, technical training for primary care providers, patient assessment guidance, patient stratification, formulation of treatment plans, tiered patient management, and establishment and tracking of medical records. General practitioners do not undertake the responsibilities of providing technical guidance to primary care providers or managing medical record establishment and tracking. Health managers are responsible for guiding respiratory rehabilitation, providing health education for chronic obstructive pulmonary disease (COPD), and conducting follow-ups on established medical records.
By establishing an Internet-based cloud platform for tiered medical diagnosis and treatment, we achieve three-level coordination among specialists, general practitioners, and family doctors, as well as the integration of physicians, patients, and medical devices. This facilitates a complete information flow covering respiratory reports, acute exacerbation phases, and stable phases across community health centers, primary care hospitals, and tertiary hospitals.
Second, the Internet facilitates rehabilitation for chronic airway diseases. It supports primary care institutions in conducting regular follow-ups, evaluating treatment efficacy based on disease status, and timely adjusting treatment plans, thereby transforming patients’ “passive treatment” into early warning and proactive management. This enables effective self-management of home-based training and rehabilitation for patients.
Third, the Internet enables intelligent, standardized management and information sharing of medical resources for chronic respiratory diseases. It facilitates primary diagnosis at the grassroots level, two-way referrals, triage between acute and chronic conditions, and coordinated care across different tiers of the healthcare system, all based on a cloud management platform.
Professor Zhou Jianying stated that the internet plays a significant role in telemedicine, pulmonary function monitoring and follow-up, medication management and monitoring for chronic airway diseases, diagnosis and treatment of sleep-disordered breathing, lung cancer screening and follow-up, home-based remote non-invasive ventilation management, and remote guidance for pulmonary rehabilitation.
Internet hospitals offer six key advantages: convenience, interactivity, efficiency, resource sharing, continuity of care, and the ability to transcend temporal and spatial constraints. These features help ensure that medical resources are effectively aligned with the clinical needs of disease treatment, with telemedicine standing out as a major highlight of internet-based healthcare.
Zhejiang University Hospital Internet Hospital: A New Model of Diagnosis and Treatment
According to Professor Zhou Jianying, The First Affiliated Hospital of Zhejiang University School of Medicine has been leveraging the internet to connect with local hospitals and provide technical guidance since the Wenchuan Earthquake.
In February 2016, the “Zhejiang First Internet Hospital” was officially launched, becoming the first online campus of a public Grade A tertiary hospital in China. To date, The First Affiliated Hospital, Zhejiang University School of Medicine has established remote consultation partnerships with more than 80 hospitals, built a four-tier networked medical service platform covering the entire province, and empowered academic internet connectivity, referral-based hospitalization, and multi-disciplinary team (MDT) services across campuses, thereby promoting the development of medical consortia.
The first model innovation is telemedicine. When patients experience physical abnormalities, they can be connected to appropriate medical resources immediately. The First Affiliated Hospital of Zhejiang University School of Medicine’s Internet Hospital offers year-round online outpatient services, enabling clinicians to provide timely consultations and address patient inquiries as needs arise. Meanwhile, under the remote consultation model, patient data is automatically collected, saving time for healthcare professionals.
Professor Zhou Jianying believes that the First Affiliated Hospital, Zhejiang University School of Medicine’s Internet Hospital has ushered in the era of smart healthcare. Telemedicine, transcending time and space, enables optimal allocation of clinical resources and enriches the patient data available to physicians for diagnosis and treatment. Previously, doctors could only rely on test results as their primary source of information. Furthermore, internet-based medication delivery has become more convenient through centralized distribution via online platforms.
The second model innovation is the integration of multi-tiered medical institutions, fostering interaction through a cascade in which large hospitals support county-level hospitals, which in turn support township health centers. This process enables more efficient utilization of healthcare resources. Furthermore, patients can schedule hospital admissions and outpatient examinations online via the internet, thereby reducing waiting times for medical care.
The third model innovation involves establishing an internet-based health management framework, delivering personalized treatment for patients with a focus on chronic disease management, geriatric care, and nursing management. In this context, the post-discharge outpatient follow-up system is particularly critical, as it can provide timely reminders for patients to undergo regular hospital check-ups or access high-quality tertiary care services conveniently within their local communities.
According to Professor Zhou Jianying, since its launch, the First Affiliated Hospital of Zhejiang University School of Medicine (FAHZU) Internet Hospital has cumulatively provided consultations to over 37,000 patients, with the oldest being 93 years old and the youngest 4 years old, and without a single complaint. Currently, FAHZU Internet Hospital operates 13 specialized outpatient clinics and engages in remote collaboration with 206 municipal and county-level hospitals both within and outside Zhejiang Province, 322 community health service centers, and 64 pharmacies, thereby facilitating tiered diagnosis and treatment.
Professor Zhou Jianying stated that internet hospitals represent a novel exploration in healthcare, expressing confidence that they will continue to improve through sustained efforts.