International Experiences and Insights in Building a DRG Payment System: A Comprehensive Review
On December 20, 2018, the National Healthcare Security Administration (NHSA) officially issued the “Notice on Declaring National Pilot Programs for Diagnosis-Related Groups (DRG)-Based Payment” (hereinafter referred to as the “Notice”). The Notice stated that, in order to implement the requirement set forth in Document No. 55—namely, “the state shall select certain regions to carry out pilot programs for DRG-based payment and explore the establishment of a DRG payment system”—the NHSA is developing DRG standards tailored to China’s healthcare service system and healthcare security management capabilities, and has launched DRG-based payment pilots in selected cities. Healthcare security administrative departments at all levels are required to attach great importance to this initiative, actively participate in the DRG-based payment pilot programs, accelerate the improvement of refined healthcare security management, and gradually apply DRGs to actual payment practices while expanding their scope of application.
Against this backdrop, VCBeat (WeChat Official Account: vcbeat) has invited Dr. Liu Zhichen, a senior expert in Diagnosis-Related Groups (DRGs) and a postdoctoral fellow in Public Administration at Fudan University, to conduct an in-depth exploration of the DRG payment system through a long-term column series. This article marks the inaugural installment of his personal column.

Dr. Liu Zhichen
The mechanism of healthcare payment system reform lies in altering the behaviors of both providers and patients through direct or indirect incentives generated by different payment methods. Different payment methods may lead to varying medical practices, thereby raising the issue of selecting appropriate payment systems from the perspectives of “ensuring service provision” and “controlling healthcare costs.”
I. Connotation and Characteristics of the DRG Payment System
The Diagnosis-Related Groups Prospective Payment System (DRG-PPS) is a reimbursement model widely adopted in many countries abroad. It establishes payment standards for each DRG category through scientific actuarial calculations and provides prospective payments to healthcare institutions accordingly. By standardizing cases through DRGs, it achieves uniform payment standards for cases within the same group. Therefore, DRG is essentially a bundled fixed-payment system based on disease groups.
Compared with other payment methods, DRG-based payment adopts pre-established DRG payment standards, shifting the profit-making approach of healthcare providers (hospitals) from increasing service volume to controlling costs. Medical institutions and physicians can achieve surplus and generate revenue only by reasonably controlling costs and improving service efficiency. Pharmaceuticals, medical consumables, and diagnostic tests have transformed from revenue sources into cost items, necessitating rational resource utilization for efficient operations. This mechanism guides hospitals to reduce average length of stay and curb inducement-driven medical consumption among patients, thereby controlling the unreasonable growth of medical expenses.
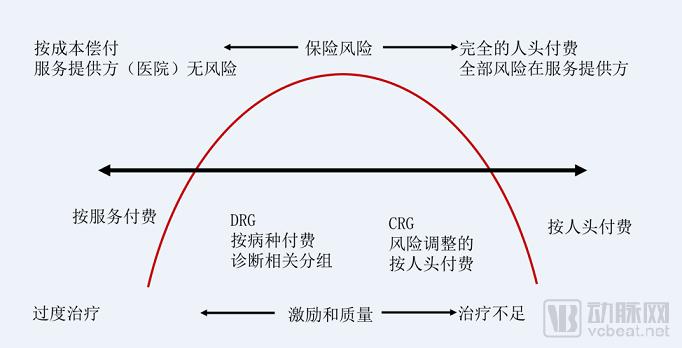
Figure 1 Differences between DRG and Other Payment Methods
II. Core Elements of the Global DRG Payment System: Lessons from International Experience
Currently, countries and regions implementing the Diagnosis-Related Group (DRG) payment system are distributed worldwide. The primary expected objectives for introducing DRGs in various countries are: 1) to enhance the transparency of medical services, facilitating monitoring of hospital expenditures by hospitals and health insurance regulatory authorities, and identifying high-efficiency services; 2) to incentivize high-efficiency, low-cost medical service practices and encourage the efficient utilization of resources. Specific manifestations include improved work efficiency, staff motivation, and transparency in service processes; reduced waiting times and length of stay; increased patient choice; assurance of medical quality; and encouragement of competition among hospitals.
The reform of the DRG payment system is not merely a matter of institutional design; it also encompasses related supporting supervision, organizational safeguards, legal protections, and technical support, constituting a comprehensive, systematic engineering effort. Differences in systems across various countries and regions have led to the diversity of DRG versions. By synthesizing the characteristics of DRG payment systems in various countries, the core elements of the global DRG payment system can be summarized as shown in Figure 2:
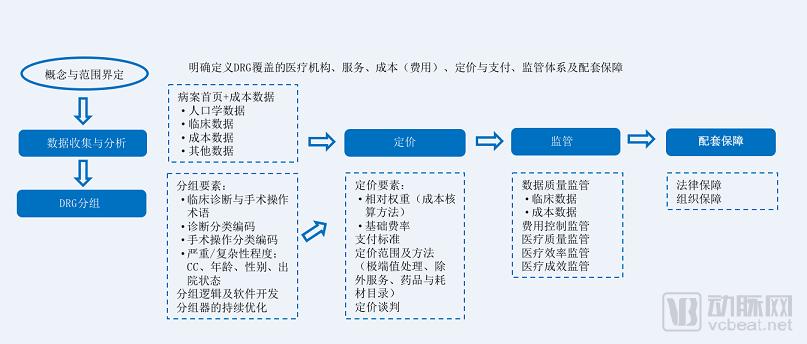 Figure 2 Core Elements of the Global DRG Payment System
Figure 2 Core Elements of the Global DRG Payment System
Since the United States’ Medicare program adopted the 470-group HCFA-DRG system, encompassing 23 Major Diagnostic Categories (MDCs), for insurance reimbursement in 1983, DRGs have been progressively introduced in Europe, Australia, and some Asian countries. Currently, nearly 40 countries worldwide utilize DRGs. When implementing DRG-based payment systems, different countries localize their DRG versions to align with national circumstances and disease spectrum characteristics. Therefore, defining the scope of DRG applicability (such as whether psychiatric disorders are included, how length of stay is defined, and whether day surgeries are covered), as well as the range of healthcare institutions and disease groups eligible for DRG-based payment, constitutes the primary prerequisite for constructing a DRG payment system.
From a global perspective, the development of DRG systems, along with accurate case grouping and weight determination, relies on two types of foundational data: first, clinical information contained in medical record face sheets, including diagnosis codes and procedure codes; second, cost information derived from medical records. Based on the clinical information, each case is assigned to a specific DRG group. Using DRG cost data, the homogeneity within different DRG groups is assessed; if homogeneity is insufficient, consideration should be given to splitting them into separate groups.
Therefore, the collection and analysis of data from medical record front sheets and cost data are crucial for accurate DRG grouping and weight determination. Taking Denmark as an example, the Dk-DRG system primarily consists of “DRG grouping logic plus cost accounting,” a framework that reflects both the clinical realities in Denmark and the cost structure of Danish hospitals.
1. Medical Record Front Page Data
The key challenges in the data quality of the medical record face sheet include the formulation and maintenance mechanisms for diagnosis and procedure coding rules, their compatibility with grouper systems, and issues regarding coding accuracy. Although grouping logics vary across countries, the overall framework is fundamentally similar. Diagnosis-Related Groups (DRGs) are assigned based on data from the medical record face sheet, including the principal diagnosis, secondary diagnoses, and surgical procedures.
The completeness and accuracy of data on the medical record face sheet, as well as the rigor of the intrinsic quality of original medical record data, will directly affect the quality of DRG grouping and the effectiveness of its application, and also serve as the basis for assigning patients to DRG payment groups. Standardized and uniform disease diagnosis and coding can not only improve the accuracy of DRG grouping but also ensure the effective operation of the DRG payment system, thereby avoiding unnecessary losses of health insurance funds due to coding errors.
2. Cost Data
High-quality and accurate cost accounting data form the basis for calculating precise DRG relative weights, and the accuracy of these weights significantly affects the effectiveness and fairness of the DRG payment system. If relative weight values are set too high, it is difficult to incentivize hospitals to improve efficiency through enhanced treatment methods. Conversely, if relative weight values are set too low, hospitals may compromise medical quality to reduce healthcare costs.
In light of the aforementioned reasons, countries have successively begun to regularly collect hospital cost accounting data after implementing DRG, in order to calculate and continuously update DRG weights.
3. Mandatory Cost Accounting System
Barbara O. Wynn & Molly Scott (2008) argue that different cost accounting methods—namely, top-down allocation (United Kingdom), bottom-up allocation (Germany), and cost-to-charge ratio (United States), which are currently the most commonly used methods internationally—exert varying impacts on the calculation of DRG relative weights.
Therefore, when introducing the DRG payment system, countries have initiated the construction of national-level cost accounting systems. Typically, countries select a cost accounting methodology based on their actual medical cost data infrastructure and data quality, while also weighing the input-output ratio of different approaches.
Furthermore, the calculation of DRG relative weights requires defining the scope of cost reimbursement under the DRG system; differences in this scope will inevitably lead to variations in DRG relative weights.
4. Data Preparation and Data Quality Oversight
Typically, to ensure the accuracy of data collection and analysis and the consistency of standards, countries initiate preparatory work 3–5 years before launching a Diagnosis-Related Group (DRG) payment system. This preparation includes formulating rules for medical record front sheets, medical terminology, diagnosis and procedure coding, and cost accounting, as well as establishing data collection and analysis frameworks. Under the condition of unified foundational data rules, clinical and cost data within the scope of DRG payment are collected and analyzed to build a database. These data are then organized and cleaned to ensure data quality. (In implementing DRG payment systems, countries typically establish specialized departments responsible for data collection, processing, supervision, and audit.) Final analyses are conducted to ensure adequate sample sizes and appropriate basic characteristics of the grouping data.
A key lesson from Germany’s DRG payment system reform is the importance of building a robust data infrastructure. The availability, timeliness, and accuracy of foundational data—such as cost, clinical, and medical record information—are among the decisive factors determining the success of the reform. Establishing a strong data foundation requires time and sustained effort.
Furthermore, the continuous evolution and updating of the DRG system itself require substantial data accumulation to better achieve ongoing improvements in disease classification, evaluation and monitoring of severity, as well as the summarization and validation of patterns within highly variable data.
Based on the collected data and analytical results, a grouping logic tailored to national conditions and characteristics is established, and a corresponding grouper is developed to assign each patient to a Diagnosis-Related Group (DRG). The grouping criteria primarily include information on disease diagnosis types, surgical and therapeutic procedures, individual patient characteristics, and the severity of the disease or complexity of treatment. These factors are reflected by variables such as age, gender, comorbidities, complications, and discharge status. Furthermore, DRG weight coefficients are calculated and determined by integrating the DRG assignment results with the severity of the disease.
The challenge in the DRG grouping process lies in assessing disease severity, specifically determining whether a patient has major complications or comorbidities (MCC), general complications or comorbidities (CC), or no CCs, thereby stratifying the severity of the patient’s condition. For the same diagnosis and treatment modality, factors such as age, the presence of MCCs or CCs, or the absence of CCs can influence the final DRG assignment. Therefore, CCs and MCCs better reflect variations among cases in terms of disease severity, overall treatment plans, physicians’ clinical expertise, healthcare resource utilization, and prognosis.
If the actual severity of a patient’s condition cannot be accurately reflected by secondary diagnoses during the DRG grouping process, it will inevitably compromise the scientific validity of both DRG classification and weight calculation, as well as affect the determination of reimbursement standards for medical expenses covered by health insurance funds. To better differentiate disease severity, the Australian AR-DRGs system employs a modeled approach to assess the severity of illness for each secondary diagnosis recorded in a patient’s medical record, in addition to the principal diagnosis.
Furthermore, countries need to annually update and continuously optimize the DRG grouper and its corresponding relative weights, taking into account advances in clinical technology and evolving real-world cost patterns.
Based on the groupings and various data collected in the preliminary phase, calculate the base rates and payment standards for different DRG groups. Typically, when the DRG payment system is first introduced, base rates can be established at three levels: national, regional, or hospital-specific. During the initial pilot phase, individual hospitals will set their own base rates. After a transitional period of several years, these base rates will gradually converge across hospitals and regions, ultimately forming a unified national base rate for payment, determined annually in accordance with laws and regulations enacted by Congress.
Meanwhile, DRG pricing must also account for special circumstances, including the handling of extreme outliers, adjustments or subsidies based on hospital tier, geographic location, and teaching status, as well as the formulation of excluded services or lists of drugs/consumables. The final actual reimbursement standards and pricing payment ranges are determined through negotiation during the development of DRG payment policies.
Taking Germany as an example, the German G-DRG system is the most fundamental method for allocating health insurance funds to medical institutions. Approximately 85% of financial resources are allocated annually through the G-DRG system, making Germany one of the countries with the highest proportion of medical expense payments based on the DRG model internationally. The method for calculating the total payment amount to each hospital under the German G-DRG system is as follows: Total Reimbursement = Relative Cost Weight × State Base Rate + Additional Costs + Surcharges for Excess Length of Stay − Deductions for Short-Stay and Transferred Patients.
Clear provisions are also made for the calculation methods of surcharges and deductions. Specifically: For long-term inpatients, an upper threshold is established for the in-range value; if this upper threshold (marginal cost) is exceeded, an additional daily compensation fee is charged. For short-term inpatients, a lower threshold is established for the in-range value; if expenditures on major service items fall below this lower threshold, a daily fee deduction is applied.
In addition, Germany has established a two-tier negotiation mechanism for DRG-based payments (at both the federal and regional levels), primarily conducted between associations of sickness funds and hospitals along with their alliance organizations, each representing their respective stakeholder interests. The negotiations focus mainly on two aspects: payment of costs and monitoring of healthcare service quality. If the parties fail to reach an agreement, the Federal Joint Committee shall make the final determination. The specific negotiation process is illustrated in the figure below:
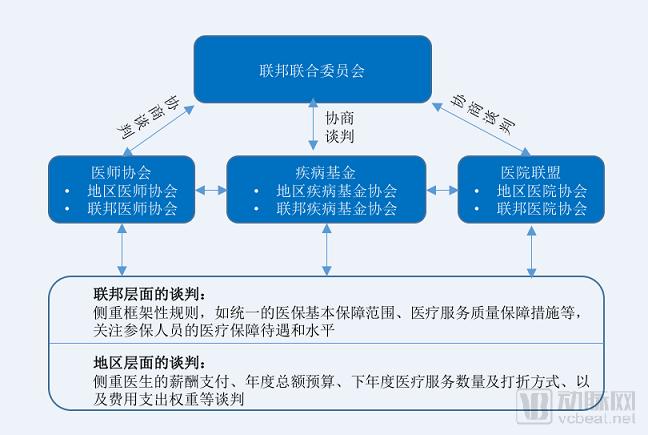
Figure 3 Negotiation Mechanism of the G-DRG Payment System
To mitigate the adverse effects potentially triggered by DRG-based payment, such as upcoding and fragmented hospitalizations, countries have implemented a series of proactive regulatory measures. These include oversight of data quality, cost containment initiatives, monitoring of medical quality and efficiency, and outcome evaluation. Leveraging robust health information systems, these nations have established relatively comprehensive sets of regulatory indicators to enable real-time monitoring of DRG implementation. Furthermore, they employ incentive and penalty mechanisms—rewarding high-performing healthcare institutions while sanctioning underperformers—to enhance regulatory effectiveness.
When implementing the DRG payment system, countries need to establish a relatively comprehensive legal safeguard framework and set up specialized professional organizations to undertake various tasks, such as the development and maintenance of grouper software, data collection and analysis, and the organization of DRG pricing negotiations. Therefore, supporting legal and organizational safeguards are also essential components in the construction of the DRG payment system.
Taking Germany as an example, upon the introduction of G-DRG, a specialized organizational body was established, and legislation clearly defined the functional division of labor and collaborative operational mechanisms among various institutions, as illustrated in the figure below:
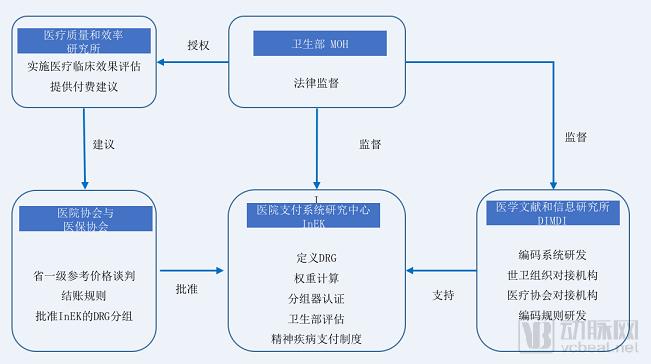
Figure 4 Organizational Safeguards and Division-of-Labor Operational Mechanism of the German G-DRG Payment System
To ensure the smooth implementation of DRG-based payment and achieve the desired outcomes, Germany has enacted a series of legal measures. These measures provide legal definitions for key aspects and relevant rules governing the DRG payment system and its operations from various perspectives. Examples include safeguarding hospitals’ rights to negotiate service prices and medical product prices in their capacity as corporate entities; clearly stipulating whether capital costs are included in medical payment rates; determining whether prices are uniform across hospitals; establishing rules for setting initial prices and transitioning toward standardized prices; and implementing measures to prevent adverse effects. As a result, Germany has effectively ensured the successful introduction of DRG, facilitated a smooth transition, and ultimately achieved significant results, making it a prominent reference case for other countries introducing or advancing DRG-based payment systems.