DRG Payment System Construction: International Experience in Clinical Data – Series II
From a global perspective, the development of DRG systems, along with accurate case grouping and weight determination, relies on two foundational types of data: first, clinical information contained in medical record face sheets, including diagnosis codes and procedure codes; second, cost information derived from medical records. Based on the clinical information, each case is assigned to a specific DRG group. Using DRG cost data, the homogeneity of different DRG groups is assessed; if homogeneity is insufficient, consideration should be given to splitting them into separate groups.
Therefore, the collection and analysis of data from medical record front pages and cost data are crucial for correct DRG grouping and weight determination. This column will separately introduce international experiences in the collection and analysis of medical record front page data and cost data.

Dr. Liu Zhichen, Senior DRG Expert and Postdoctoral Fellow in Public Administration at Fudan University
I. What Is the Medical Record Face Sheet
The medical record face sheet is a summary of the patient’s inpatient diagnosis and treatment. It constitutes the most concentrated, important, and core part of the entire medical record. The items on the face sheet essentially cover all basic patient information and all data required for Diagnosis-Related Group (DRG) grouping—including patient demographics, hospitalization process details, diagnostic and therapeutic information, and cost information—thereby serving as the basis for DRG implementation.
The completeness and accuracy of data on the medical record face sheet, as well as the rigor of the intrinsic quality of the original medical record data, will directly affect the quality of DRG grouping and the effectiveness of its application. Therefore, healthcare professionals need to use text, symbols, codes, numbers, and other methods to concisely summarize relevant information from the patient’s hospitalization period on the medical record face sheet, thereby forming a data abstract of the patient’s case.
II. Relationship Between Core Information on the Medical Record Front Sheet and DRG Grouping
On the front page of the medical record, standardized names for disease diagnoses and surgical procedures shall be used. This serves as a critical basis for Diagnosis-Related Group (DRG) classification. The core principle of DRG grouping is based on commonalities; among the information used for grouping, the patient’s diagnosis is the most important factor. For diseases and diagnoses, such commonality is reflected in the consistency of categorical attribution.
Therefore, the implementation of Diagnosis-Related Groups (DRGs) necessitates the selection of an appropriate disease classification methodology. The actual DRG grouping process relies on computerized processing, thereby requiring the “coding” of the grouping procedure. Cases of different categories are typically distinguished using diagnosis codes, while different treatment modalities are differentiated using procedure classification codes. Patient-specific characteristics are represented by factors such as age, sex, and birth weight (used for the classification of neonatal cases). Evidently, disease diagnoses and corresponding procedures constitute the key “axes” for DRG case classification.
Furthermore, disease diagnosis and surgical procedure codes not only form the basis for establishing Diagnosis-Related Groups (DRGs) but also serve as the criteria for determining the DRG category for patient reimbursement. According to estimates from the U.S. Medicare program for fiscal year 1996, the erroneous payment rate (primarily due to coding errors) was 14%, amounting to $23.2 billion; in 1999, the erroneous payment rate was 8%, totaling $13.5 billion; and in 2000, it was 6.8%, totaling $11.9 billion. The U.S. Health Care Financing Administration aimed to reduce the erroneous payment rate to 5% by 2002. According to reports from the U.S. Office of Inspector General, these errors were entirely attributable to inaccurate medical information provided by physicians and incorrect coding.
Therefore, standardized and uniform disease diagnosis and coding can not only improve the accuracy of DRG grouping but also ensure the effective operation of the DRG payment system, thereby avoiding unnecessary losses of medical insurance funds due to coding errors.
III. Development of the International Classification of Diseases Coding
As early as the 18th century, Sir George Knibbs, an Australian statistician, began attempting to systematically classify diseases. In 1891, the International Statistical Institute established a special committee dedicated to the classification of causes of death, with Jacques Bertillon, the head of statistical affairs for the City of Paris, serving as its chairman. In 1893, Jacques Bertillon submitted a unified classification system for causes of death, originally proposed in 1853, to the International Statistical Institute’s conference held in Chicago. This method was accepted and became known as the Bertillon Classification of Causes of Death.
Subsequently, this method was adopted by multiple countries and many cities. In 1898, at the meeting of the American Public Health Association held in Ottawa, North American countries including the United States accepted the Bertillon Classification of Causes of Death and recommended that it be revised every ten years. In 1946, the World Health Organization (WHO) took over the revision of this classification. Starting with the sixth revision, the classification began to incorporate disease classification. In 1975, WHO released the Ninth Revision of the International Classification of Diseases, abbreviated as ICD-9, which was widely used worldwide. In 1992, WHO released the Tenth Revision, titled “International Statistical Classification of Diseases and Related Health Problems, Tenth Revision,” abbreviated as ICD-10.
When determining classification, ICD-10 primarily references etiology, anatomical site, pathology, and clinical manifestations (including symptoms, signs, staging, typing, gender, age, and acute or chronic onset timing). These attributes constitute independent classification criteria, known as classification axes. The International Classification of Diseases, Tenth Revision (ICD-10), is a multi-axial classification system in which categories are distinguished by codes. Basic categories are identified by three-digit category codes, and each category can be further subdivided into up to ten subcategories, identified by a fourth character.
The first character of the code is a letter, followed by three digits for the second through fourth positions, with a decimal point separating the third and fourth digits. For example, in the code “H25.0”, “H25” represents the category, which stipulates that all cases of “initial senile cataract” are classified under this subcategory. Subcategories provide greater detail than categories, but each subcategory must belong to a specific category.
The ICD-10 classification features a hierarchical and granular structure, with mutually exclusive codes, meaning that a specific disease condition can only be assigned an appropriate code under a single category. This is inconsistent with the principle of DRG grouping, which relies on coding the entire hospitalization process—i.e., using a set of codes to document and represent the information for each inpatient case regarding that episode of care.
Therefore, upon its release, the International Classification of Diseases, 10th Revision (ICD-10), stated that its purpose was to “permit the systematic recording, analysis, interpretation, and comparison of mortality and morbidity data collected in different countries or areas and at different times.” “The ICD is not intended nor suitable for indexing individual clinical cases. The ICD also has certain limitations when used for financial purposes, such as billing or resource allocation.” This is a general description of the uses of ICD-10 as outlined in Volume 2 of ICD-10.
To meet diverse usage requirements, the ICD must be appropriately extended through coding refinement. The impetus for coding refinement primarily stems from two sources:
One aspect is the clinicians’ need for diagnostic terminology that aligns with clinical practice. The International Classification of Diseases (ICD) provides textual descriptions corresponding to its classification codes; some of these descriptions are identical to diagnostic names, others are similar, and still others differ substantially from diagnostic names. When applying ICD coding, there is a natural requirement to ensure that actual clinical diagnoses align closely with the ICD in both form and content.
In actual practice, the situation is reversed: it is necessary to adopt standardized terminology or de facto standard phrases as the basis for formulating diagnostic names that correspond to codes. This inevitably results in multiple diagnostic names, each emphasizing different clinical conditions, being categorized under a single subcategory. To distinguish these diagnostic names in coding, each diagnosis must be assigned a unique code, thereby generating refined extension codes for classification.

Another driver for coding refinement stems from the application of classification and coding systems. The International Classification of Diseases (ICD) system features predefined classification axes, a fixed order of axis usage, and specific metrics; however, as explicitly noted by the World Health Organization (WHO) in its guidelines on disease classification systems, these rules are not universally applicable. Other statistical models, such as Diagnosis-Related Groups (DRGs), although also based on disease classification and leveraging the ICD framework, differ in their details. One technical approach to bridging this gap is to refine and expand the ICD, thereby generating more granular codes.
In summary, the ICD-10 falls short of clinical needs in terms of classification methods, terminology, granularity, and documentation expressiveness, and the same applies to DRG and other evaluation and analysis models. Therefore, when implementing DRGs, countries have systematically expanded the International Classification of Diseases based on their actual clinical requirements, giving rise to country-specific “Clinical Modifications” (CM).
The clinical version is a system developed and established to better characterize patients' clinical conditions. The development of the expanded International Classification of Diseases (ICD) "Clinical Version" is subject to prerequisites and basic requirements, including: codes must not conflict with those in the standard version; it should appropriately inherit and adhere to the coding principles of the standard version; it should allow for simple and rapid conversion to the standard version; and it must not impede the use of the standard version.
Country | Diagnostic Code |
United States | ICD-9-CM or ICD-10-CM |
Australia | ICD-10-AM |
Germany | ICD-10-GM |
Canada | ICD-10-CA |
IV. Development of the International Classification of Surgical Procedures
The development and evolution of the International Classification of Diseases (ICD) have spanned over a century. Early versions of the ICD did not include a classification system for surgical procedures. However, as understanding of medicine deepened and the processing of hospital medical record information became more sophisticated, it became evident that a coding system was needed to supplement the International Classification of Diseases.
The United States developed a classification of surgical procedures as a supplement to the ICD as early as 1959. The purpose of this procedural classification is to standardize the various terms used by physicians for the same surgical procedure, translating them into standardized codes based on established principles. This classification system serves as one of the primary tools for processing, retrieving, aggregating, and analyzing hospital medical record information. Its importance is comparable to that of disease classification, whether applied in healthcare delivery, research, education, management, or in areas such as medical reimbursement, clinical pathways, and hospital evaluation.
Subsequently, recognizing the need for a classification of medical procedures across countries, the WHO published the trial version of the International Classification of Procedures in Medicine (ICPM) in 1978, which covered diagnostics, tests, prevention, surgical operations, other treatments, and auxiliary processes. In the early 1980s, the WHO decided to discontinue updates to the ICPM, primarily because this classification failed to achieve global consensus comparable to that of ICD-9. Over the following two decades, no unified international classification of surgical and procedural interventions emerged; while some countries developed their own standards, these were often mutually incompatible.
Country | Surgical Procedure Classification Code |
United States | ICD-9-CM-3 or ICD-10-PCS |
Australia | ICD-10-AM(ACHI) |
Germany | OPS-301 2.0 |
Canada | CCI |
United Kingdom | OPCS 4 |
From late 2006 to early 2007, the WHO decided to develop the International Classification of Health Interventions (ICHI). The ICHI is largely derived from the Australian Classification of Health Interventions (ACHI), which is part of the Australian version of ICD-10. The ACHI was basically created based on ICD-10 and the US clinical modification of ICD-9-CM. In 2010, the structure, content patterns, and coding rules of the ICHI were finalized. The alpha version of the ICHI was released in October 2012. It was updated to the beta version in 2017 and remains in the testing phase to date.
In 1978, the U.S. National Center for Health Statistics organized numerous academic organizations to revise and publish the Clinical Modification of the Ninth Revision of the International Classification of Diseases (ICD-9-CM) in response to diverse needs. The term “Clinical” emphasizes that its revised content is more suitable for disease data reporting, statistical compilation, and data comparison. It facilitates internal and external assessments of the timeliness and appropriateness of healthcare services. ICD-9-CM consists of three volumes. Volumes I and II are fully compatible with ICD-9 but include additions at the fifth digit of the codes. Volume III is an adaptation of the International Classification of Procedures in Medicine. To keep pace with clinical practice and contemporary scientific advancements, ICD-9-CM-3 is revised and supplemented annually to correct errors and add new entries, ensuring more comprehensive and up-to-date content.
The coding structure of the ICD-9-CM-3 Classification System for Surgical and Diagnostic Procedures follows the three-tier tree structure of ICD-9. The first tier consists of categories, represented by two-digit codes (00–99); the second tier comprises subcategories, represented by a single digit (0–9); and the third tier includes subclassifications, also represented by a single digit (0–9), although this level is not defined for certain subcategories. Each subclassification serves as the final classification level and may encompass different surgical techniques within the same type of procedure. While this classification system exhibits strong clustering capabilities and facilitates statistical analysis, its relatively coarse coding precision limits in-depth applications. In practice, clinical care and scientific research require higher-precision coding.
Following the tenth revision of the International Classification of Diseases, the United States conducted relevant research and developed the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) for clinical use, as well as the International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS). The ICD-10-PCS was officially implemented in October 2015.
A comparative analysis of the aforementioned major surgical procedure classification systems is presented in the table below:
Examples and Comparison of Different Surgical Procedure Classification Methods
Classification System | Coding | Coding Instructions |
ICD-9-CM-3 | 36.07 | Drug-Eluting Coronary Stent Implantation |
0.47 | Triple-Vessel Stent Implantation | |
0.66 | Percutaneous Coronary Balloon Angioplasty | |
0.42 | Three-Vessel Procedure | |
ICD-10-PCS | 02725DZ | No. 1: Chapter on Medical Procedures 0 |
Second: Heart and Great Vessels 2 | ||
Third: Dilating the lumen of a specific body part7 | ||
Fourth: 3-vessel coronary artery disease, type 2 | ||
Fifth: Percutaneous Intraluminal Access 5 | ||
Sixth: Intracavitary Device D | ||
7th: No Z | ||
ICHI | ADL FD AF | Part I: ADL Coronary Artery |
Part II: Expansion of FD’s Equipment Usage | ||
Part III: AF Endoluminal |
Comparison of the Characteristics of Different Surgical Procedure Classification Systems
Classification System | Objective | Application Scope | Clinical Applicability | Ease of Operation | Is there an index? |
ICD-9-CM-3 | Classification of Surgical Procedures | Clinical Examination, Payment | Best | Convenience | Yes |
ICD-10-PCS | Replacement for ICD-9-CM-3 | Clinical Examination, Statistical Management, Payment, etc. | General | General | Yes |
ICHI | Classification of Health Interventions | Clinical Examination and Statistical Management | General | More Complex | None |
In summary, the aforementioned major surgical procedure classification systems each have their own characteristics: ICD-10-PCS has broader coverage, ICHI is more fundamental, and ICD-9-CM3 demonstrates the strongest clinical applicability.
V. The Relationship Between the Data Quality of the Medical Record Front Page and Correct Grouping
DRG grouping is based on data from the front page of inpatient medical records, including principal diagnosis, secondary diagnoses, and surgical procedures. The accuracy of metrics such as average length of stay and average cost for DRG groups depends on the volume and quality of case data for similar conditions within the region. Therefore, improving the data quality of the front page of medical records and standardizing its completion and coding practices are essential for accurate DRG grouping.
Although DRG versions in various countries incorporate localized designs tailored to national characteristics, the overall grouping logic and methodology remain broadly similar, encompassing the following classification strategies:
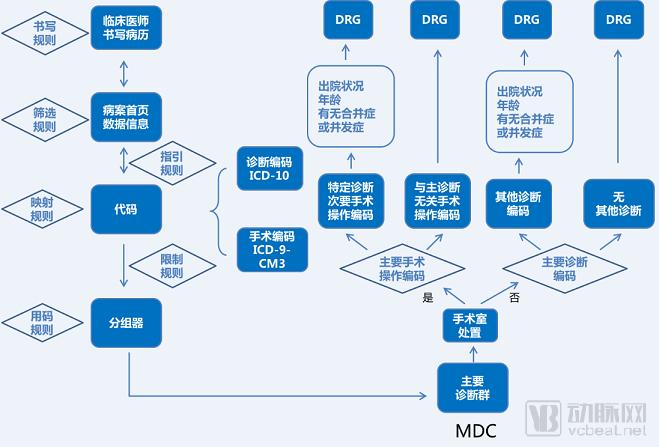
First, cases are classified according to the principal diagnosis to form Major Disease Categories (MDCs), which are categorized primarily by anatomical and physiological systems (MDC refers to the result of classifying principal diagnoses by anatomical systems and other major categories). Then, by comprehensively considering the principal diagnosis and primary procedure, cases are further subdivided into Adjacent Diagnosis Related Groups (ADRGs). ADRGs refer to case groups with identical principal diagnoses or primary procedures; from a classification perspective, they denote case categories derived solely from principal diagnoses and procedures, without considering individual patient characteristics, comorbidities, or complications. Each ADRG contains one or more DRGs. In the third step, ADRGs are further subdivided into Diagnosis Related Groups (DRGs) by comprehensively considering other individual patient characteristics, comorbidities, and complications.
The process of MDC classification typically relies solely on the principal diagnosis code. The assignment from MDCs to ADRGs utilizes both the principal diagnosis code and the principal procedure code, while the refinement from ADRGs to DRGs incorporates additional diagnoses and procedures, along with other variables reflecting individual patient characteristics. This is illustrated in the figure below:
The Relationship Between the DRG Grouping Process and Coding
Therefore, the DRG grouping process itself imposes extremely high requirements on the data quality of the medical record face sheet, particularly the coding data quality. Taking the data field requirements for the medical record face sheet needed by the CN-DRG grouping scheme as an example:
Classification Axis | Information/Data |
Disease Severity and Complexity | Primary diagnosis, comorbidities and concomitant diseases, individual factors (e.g., age, sex, infant birth weight, days since birth, neonatal admission weight, etc.) |
Medical Needs and Usage Intensity | Surgical procedures in operating rooms, non-operating room surgical procedures, and other ancillary medical and nursing services (e.g., ventilator use) |
Medical Outcomes | Discharge Status (Death, Discharged by Medical Order, Discharged Against Medical Advice, Transferred) |
Resource Consumption | Medical Costs, Cost Classification, Length of Stay |
Coding System | Diagnosis: ICD-10 Clinical Version; Surgical Procedures: ICD-9-CM Volume 3 Clinical Version |
Data Source | Front Sheet of Inpatient Medical Record |
If errors occur in completing the data on the medical record front sheet, they typically lead to incorrect DRG grouping. Common key data quality issues related to DRG grouping are shown in the table below:
Question Category | Causes of the Problem |
Data Quality Reflecting Disease Severity and Complexity: Diagnostic Issues | 1. Inconsistent diagnostic nomenclature; 2. Errors, omissions, non-standardization, and incompleteness in principal diagnoses; 3. Errors, missing entries, and non-standardization in secondary diagnoses; 4. Missing or inaccurate individual factors such as age and sex |
Data Quality Reflecting Healthcare Resource Utilization and Intensity: Issues with Surgical Procedures and Ventilator Use | 1. Inconsistent naming of surgical procedures; 2. Omission or inaccuracy in recording primary surgeries; 3. Omission or inaccuracy in recording other surgeries or procedures; 4. Complete absence of data on intensive care unit (ICU) stay duration and mechanical ventilation time |
Medical Outcomes: Discharge Status Issues | Incorrect discharge status (death, physician-ordered discharge, non-physician-ordered discharge, incorrect transfer information) |
Cost and Time Consumption: Cost Issues | 1. Surgical procedures were performed, but the surgical fee is 0; 2. The sum of itemized charges does not equal the total cost; 3. The admission time is later than the discharge time. |
Encoding Issues | 1. Incorrect code selection; 2. Inconsistent coding dictionary database |
Therefore, strengthening the management standards for the data quality of medical record front sheets requires close coordination among multiple departments within the hospital:
Clinicians shall accurately complete diagnostic and surgical procedure information as required and assume responsibility for the content entered; coders shall accurately distinguish between disease classification codes and surgical procedure codes as required (if a clinician has made a clear diagnosis but the documentation format does not comply with the rules for disease and surgery classification, coders may assign codes in accordance with the classification rules); medical institutions shall properly categorize fees/costs on the front page of inpatient medical records to ensure that each fee/cost category is clear and accurate; information management personnel shall upload data in a timely manner in accordance with data transmission interface standards to ensure the completeness and accuracy of data on the front page of inpatient medical records. Meanwhile, in regions implementing Diagnosis-Related Groups (DRG), conducting regular supervision and inspection of the front page of medical records, continuously identifying data quality issues through such inspections, proposing corrective measures, and strengthening ongoing training for physicians and coders are also critical foundational tasks for improving the overall quality of data on the front page of medical records across the region.
VI. DRG Implementation and Up-coding Issues
Upcoding (also known as overcoding, coding escalation, or upcoding) refers to the erroneous coding and classification of patient data to increase reimbursement for healthcare services. This practice leads to the distortion of health statistics and the abuse of financing systems. Following the implementation of Diagnosis-Related Group (DRG) prospective payment, hospitals may be inclined to engage in erroneous coding in response to imposed budget constraints.
"Due to the 'reasonable variability and uncertainty inherent in medical issues, where subtle diagnostic nuances and slight imprecisions in wording can have significant consequences for DRG reimbursement,' this 'medical variability and uncertainty' creates information asymmetry between hospitals (healthcare professionals) and insurers responsible for reimbursing medical costs. Therefore, in this sense, upcoding is theoretically inevitable and will occur regardless of the measures taken."
In the first decade of DRG implementation in the United States, each revision to the DRG system was followed by a new wave of upcoding. Silverman and Skinner also demonstrated the widespread nature of upcoding risk, finding that 25% of non-profit hospitals and 32% of for-profit hospitals exhibited such risks.
Many countries are exploring measures to curb such phenomena, for example, by establishing incentive systems to encourage accurate coding in hospitals. A German study found that medical records alone are insufficient to provide adequate coding information. However, other studies have shown that coding errors in many hospitals are predominantly characterized by “under-coding,” which leads to inadequate reimbursement for hospital costs; hospitals are more concerned about this issue than about “over-coding.” Therefore, methods to enhance coding accuracy, such as ongoing education and training for coders, need to be significantly strengthened.
Copyright Notice: The majority of the viewpoints presented in this article constitute the personal research findings of Dr. Liu Zhichen’s postdoctoral project. All cited articles and viewpoints reflect the perspectives of their respective authors, obtained from publicly available sources. Unauthorized reproduction, excerpting, copying, mirroring, or any other form of use is strictly prohibited.
References:
1. Deng Xiaohong. Research and Application of the Beijing DRGs System [M]. Beijing: Peking University Medical Press, 2015.
2. At the ISO/TC 215 Plenary and Working Group Meetings, held in conjunction with the DRG Standardization Sub-forum of the International Summit on Health Information Standardization on April 17, 2017, Huang Feng, Head of the ICD Coding Group at the DRG Quality Control Center under the Bureau of Medical Administration and Hospital Supervision of the National Health and Family Planning Commission, and Director of the Information Center and Medical Records Statistics Department at Peking University People’s Hospital, delivered a speech entitled “Application Requirements of ICD Coding for DRG-PPS.”
3. Chen Hua, Zhang Xiao. Formulation of the Chinese Version of Diagnosis-Related Groups and Its Application in Medical Insurance [J]. Journal of Nanjing Medical University (Social Sciences Edition), 2007(12): 301-304.
4. Huang Feng, Yang Jian, Zhao Enhui. Disease Classification Conversion Based on Diagnostic Names [J]. Chinese Hospital Management, 2003, 8(23): 30-31.
5. Ci Puwa, Liu Aimin. Comparative Study of International Common Classification Systems for Surgical Procedures and Operations[J]. Chinese Medical Record, 2015, 16(9): 29-32.
6. Liu Aimin. International Classification of Diseases, Ninth Revision, Clinical Modification, Volume 3: Procedures and Operations (ICD-9-CM-3) [M]. 2011 Edition. Beijing: People’s Military Medical Press, 2013.
7. Huang F, Chen JM, Guo MN, et al. Design and implementation of the Beijing clinical version of ICD-10 [J]. Chinese Journal of Hospital Administration, 2011, 27(11):835-838.
8. Zhao Yingxu, Jiang Qin. Experience of Medicare Inpatient Payment Reform in the United States and Its Implications for China [J]. Chinese Health Economics, 2013(6):95-97.