Novartis and Gilead: Divergent Paths in CAR-T Commercialization
Editor’s Note: This article is republished from MedTrend, with authorization granted to VCBeat.
Two or three decades ago, treating cancer with a patient’s own living immune cells was nothing short of science fiction. Today, however, this technology has become a reality.
In 2017, the successive approvals of CAR-T therapies from Novartis and Gilead pulled patients with certain previously incurable blood cancers—whose survival was typically measured in weeks to months—back from the brink of death. The industry was abuzz!
* CAR-T is the abbreviation for chimeric antigen receptor T cells. Through genetic engineering, these T cells are programmed to identify specific proteins on tumors, thereby killing tumor cells.
However, as these two products move beyond cautious, tightly controlled clinical studies and into the more complex and diverse landscape of commercialization, they—and their respective companies—are heading down two distinctly different paths.

▲ Comparison of Novartis and Gilead CAR-T Products
In August 2017, Novartis’ Kymriah became the first therapy approved for pediatric acute lymphoblastic leukemia (ALL), a rare form of blood cancer. At the time, Novartis management projected that there would be approximately 600 eligible patients per year.
In May 2018, Kymriah was approved for use in adults with a high probability of non-Hodgkin lymphoma (NHL).
In October 2017, Gilead’s Yescarta was approved for the treatment of several types of adult non-Hodgkin lymphoma (NHL).
Of course, these two products can only be used when other treatment options, such as chemotherapy and bone marrow transplantation, have been exhausted or ruled out.
The prices of both cell therapies are quite high:
Novartis’ Kymriah: A one-time fee of $475,000, with a refund available if it proves ineffective after one month;
When used to treat non-Hodgkin lymphoma (NHL), the one-time charge is $373,000, with no refunds.
Gilead’s Yescarta: Priced at $373,000, non-refundable.
That is to say, for the common indication of NHL, the pricing of the two products is consistent.
Theoretically, Novartis’ Kymriah, which received approval first and has two indications, should have decisively outperformed Gilead’s Yescarta in terms of revenue. However, the reality has been startlingly disappointing!
The first three quarters of 2018,
Gilead’s Yescarta: Commercial Performance Exceeds Expectations, Generating $183 Million in Revenue.
Novartis’ Kymriah: Revenue of only $48 million. In other words, the world’s first CAR-T product generated less than a fraction of the revenue of Yescarta, the second approved therapy!
What Has Led to the Polarized Revenue Outcomes Following Commercialization?
To date, Gilead’s CAR-T product, Yescarta, has delivered surprisingly strong commercial results, exceeding physicians’ expectations and approaching the efficacy seen in successful clinical trials. Dr. Caron Jacobson, who treats patients with leukemia and lymphoma at the Dana-Farber Cancer Institute in Boston, noted that Yescarta’s safety profile is particularly “reassuring.”
* The Dana-Farber Cancer Institute is one of the leading CAR-T therapy centers in the United States.
In December 2018, two studies were presented at the annual meeting of the American Society of Hematology: patients receiving commercial treatment with Gilead’s Yescarta showed slightly poorer outcomes compared to the 101 patients in the ZUMA-1 trial. At first glance, this may not seem cause for celebration. However, once a drug is marketed, patients typically are near death or have other comorbidities, resulting in more complex clinical presentations that are harder to predict and less strictly controlled.
* Kite Pharma previously secured FDA approval through the ZUMA-1 trial.
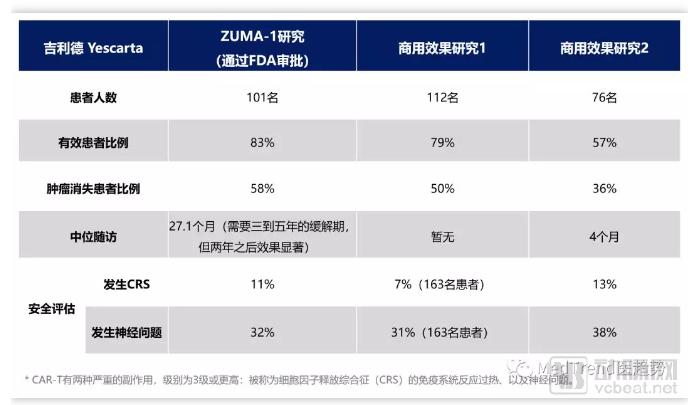
▲ Comparison of Clinical Trial Results and Commercial Performance Data for Gilead’s Yescarta
In the ZUMA-1 trial, many patients have been more than two years post-single infusion. In the updated data from December 2018, Yescarta helped reduce tumor burden in 83% of patients, with 58% achieving complete remission. (Median follow-up: 27.1 months.)
Some observers say that CAR-T therapy requires a remission period of three to five years, but the effects are significant after two years.
In the report released in December 2018, the follow-up period for patients was not as long. Nevertheless, the results were equally promising.
Among 112 patients treated at 17 medical centers (including MD Anderson and the University of California, San Francisco), one-month results showed that 79% of patients responded to treatment, and 50% showed no signs of cancer. In the same study, 163 patients underwent safety evaluation. CAR-T therapy has two serious side effects graded as level 3 or higher: an overactive immune response known as cytokine release syndrome (CRS), and neurological issues. CRS occurred in 7% of patients, while neurological problems were observed in 31%. These figures are very similar to those from the ZUMA-1 trial (where the rates were 11% and 32%, respectively).
Among 76 patients treated at various centers, including Dana-Farber Cancer Institute and the Seattle Cancer Care Alliance, 57% responded to treatment, and 36% showed no evidence of cancer. The median follow-up for patients receiving CAR-T therapy was 4 months. Thirteen percent of patients experienced grade 3 or higher cytokine release syndrome (CRS), and 38% had grade 3 or higher neurological events. The ZUMA-1 trial did not have data available at the 4-month mark; however, at the 6-month assessment conducted two years prior, approximately 35% of patients were found to have essentially complete remission of their cancer.
It is worth noting that in this study, more than 60% of patients did not meet the eligibility criteria for ZUMA-1, partly because their condition was too severe. Jacobson, the first author of the study and Medical Director of the Immune Cell Therapy Program at Dana-Farber Cancer Institute, stated that similar results “may indicate that data from ZUMA-1 provide an accurate representation of Yescarta’s safety,” regardless of patients’ clinical status.
To date, the efficacy gap between Yescarta’s clinical trial results and its real-world commercial use has been minimal. “The efficacy of every oncology drug tends to decline in real-world settings, but with Yescarta, I was surprised,” said Neelapu from The University of Texas MD Anderson Cancer Center. He was particularly encouraged that the safety data from both studies were comparable to those from ZUMA-1. “I had anticipated higher toxicity, given that the patients were more severely ill.”
Neelapu stated that a potential factor contributing to the better-than-expected outcomes was the administration of short-term “bridging” therapy to patients with a life expectancy of only weeks or months.
Yescarta and Kymriah are autologous CAR-T products, with production and administration taking approximately three weeks. The process requires extracting the patient’s T cells, genetically modifying them in a laboratory, expanding their population through culture, and then reinfusing them into the patient.
Since CAR-T cell production takes three weeks, some patients may not survive long enough to receive the therapy. Therefore, physicians administer radiation or other treatments as a “bridge” to CAR-T therapy. The side effects of CAR-T therapy are amplified by the tumor burden in the patient’s body; radiation or other interventions can shrink tumors, thereby reducing CAR-T-related adverse effects. Imagine the “killer” T cells as sharks feeding voraciously, with cancer serving as their prey. The less prey available, the less collateral damage occurs during the attack. This bridging approach also carries side effects. Consequently, trained staff, steroids and other medications to suppress potentially runaway immune responses, and intensive care units are typically kept on high alert.
Gilead’s Yescarta has been widely praised and favored by physicians for its better-than-expected real-world performance, making its strong revenue generation well deserved. So, is Novartis’ Kymriah underperforming in revenue due to inferior efficacy?
Actually, it is not.
Novartis’s Kymriah has also demonstrated strong clinical efficacy, but its real-world utilization is significantly lower. In addition to the fact that pediatric acute lymphoblastic leukemia (ALL), the first indication for which Kymriah received approval, is a rare disease with a smaller patient population than that of Hodgkin lymphoma, the indication for which Gilead’s Yescarta was approved, Novartis has encountered challenges in the large-scale manufacturing of this complex product.
Maloney of the Bezos Clinic stated that experimental records for Novartis’s Kymriah suggest its side effects may be less severe due to engineering differences. However, he prefers using Yescarta to treat lymphoma patients for a simple reason: “Novartis is still struggling to produce Kymriah, and I cannot yet obtain it from them.”
MD Anderson Cancer Center is one of the top CAR-T therapy centers in the United States. According to Sattva Neelapu, a hematologic malignancy expert at the center, the number of patients treated with Kymriah was “only in the single digits” as of late November 2018.
Similarly, at another major CAR-T center—the Dana-Farber Cancer Institute—this figure is also in the single digits, standing at 2.
The path to commercialization is the path to scale. The primary manufacturing challenge for Novartis’s Kymriah has been insufficient yield of active “killer” T cells following ex vivo gene editing, making standardized CAR-T manufacturing a critical issue. Eric Althoff, a spokesperson for Novartis, stated, “Final products fail to meet specifications typically because the proportion of viable cells is lower than expected.” (In Novartis’s pivotal clinical trials of Kymriah for acute lymphoblastic leukemia and lymphoma, 7%–9% of patients did not receive CAR-T cell infusions due to manufacturing failures.)
An executive at the company responsible for cell and gene therapy once stated that, because Novartis could not charge for a product that failed to meet commercial specifications, many patients received Kymriah treatment free of charge.
At the recently concluded JPM Healthcare Conference, executives from several CAR-T companies, including Celgene, agreed on the need for better control over the production and delivery of cell therapies. Manufacturing has become a key differentiator in determining the commercial success of CAR-T immunotherapies.
Novartis’s current predicament stems precisely from this issue. The company is striving to address manufacturing challenges by continuously improving its processes to enhance efficiency and reduce product variability. Novartis has also stated that it is pursuing automation of the CAR-T manufacturing process to increase consistency while ensuring a safe and high-quality final product.
Gilead, a competitor, is also pursuing automated manufacturing and focusing on next-generation automated manufacturing systems.
Novartis executives are attempting to view Kymriah from a positive perspective.
Elizabeth Barrett, former head of Novartis Oncology, stated, “Despite the challenges we encountered in manufacturing, we have actually exceeded expectations, and centers continue to place orders for Kymriah.”
Novartis Global CEO Vas Narasimhan stated that Kymriah’s safety profile has encouraged Novartis to expand production in France, Switzerland, and China. (Data from the commercial use of Kymriah have not yet been released.)
Vas Narasimhan is also optimistic that CAR-T therapy can treat patients in the early stages of cancer, not just those with advanced disease. “We truly believe this is a long-term game, and we are very confident in the prospects of our drugs.”
However, to instill the same confidence in others, more data beyond that of first-generation CAR-T products are required. The industry is closely monitoring safety data for next-generation CAR-T therapies, with several companies, including Novartis and Gilead, developing experimental CAR-T treatments for cancers such as blood cancers. If these therapies demonstrate improved safety profiles, the use of CAR-T in broader clinical settings will become feasible.
The breakthrough nature of CAR-T therapy led to Kymriah and Yescarta being labeled as “blockbuster drugs” upon their market launch. This high expectation is evident from Novartis CEO’s ambition to extend CAR-T therapy to patients in the early stages of cancer, as well as Gilead’s $11.9 billion acquisition of Kite Pharma just before Yescarta’s approval. A third CAR-T therapy, JCAR017, developed by Juno Therapeutics (a subsidiary of Celgene, now part of Bristol Myers Squibb), is also poised for launch.
However, beyond therapeutic efficacy, it is also essential to strengthen the industrial chain. The commercial setbacks encountered by the world’s first marketed CAR-T drug have highlighted the imperative need to optimize manufacturing processes. If domestic companies dedicated to CAR-T development can strategically position themselves in advance, they may gain a competitive edge in the commercial application of their products post-launch.