100,000 Capsule Gastroscope Examinations Reveal China's Digestive Health Landscape and the Societal Value of Intelligent Medical Devices: Release of the 'China Digestive Disease Screening White Paper'
Our daily activities require energy, which is derived from food through processing and conversion by the digestive system. The stomach serves as the initial site for digestion and absorption in the human body, as well as the primary gateway for obtaining energy and nutrients. If the stomach fails to function properly, it can lead to abnormalities in the entire digestive system and cause issues in other organs of the body.
With social development, environmental changes, and shifts in lifestyle, the incidence of digestive system diseases has been increasing year by year. Due to the fast-paced life and high work pressure, most modern people suffer from suboptimal gastric health. Gastric disease is a chronic condition resulting from the long-term combined effects of various factors, such as genetics, environment, diet, medication, bacterial infections, smoking, and excessive alcohol consumption. As the pace of modern life accelerates, many people frequently stay up late and work overtime, leading to irregular daily routines. They often skip meals during busy periods and engage in binge eating when idle, causing extreme hunger or overfullness in the gastrointestinal tract. Over time, this places an excessive burden on the gastrointestinal system, disrupting its normal function and contributing to the persistently high incidence of digestive tract diseases.
VCBeat and Anhan Technology jointly conducted a large-sample profiling of the Chinese population with upper gastrointestinal diseases, based on 100,000 anonymized capsule gastroscopy reports. This initiative presents the gastrointestinal health status of Chinese residents and seeks to explore the deeper social value of capsule endoscopy technology in the context of device miniaturization and intelligent advancement.
We found that:
1. The incidence of gastric cancer in males is significantly higher than that in females, with the age-standardized incidence rate being 2.4 times that of females.
2. Most gastric diseases are concentrated in the gastric antrum
3. Intelligent and miniaturized device technologies, represented by capsule endoscopy, are transforming traditional diagnostic and therapeutic workflows, serving as a paradigm of disruptive innovation
The following is an excerpt from the report. To access the full version, scan the QR code below or visit the Reports section:

1.1 Gastrointestinal Diseases Have Become Common Ailments in the New Era, with a High Incidence of Gastric Cancer
The progression of gastric diseases is a gradual process; it takes 3 to 5 years, or even longer, to evolve from initial gastritis and precancerous lesions to gastric cancer. However, this process is generally asymptomatic, and most cases are diagnosed at an intermediate or advanced stage.In China, opportunistic outpatient screening has long been employed for gastric diseases, resulting in an early diagnosis rate of less than 10%. The five-year survival rate varies significantly depending on the stage at which gastric cancer is diagnosed and treated. After surgical resection, the five-year survival rates are 90% for Stage I, 66% for Stage II, and 51% for Stage III, whereas it drops to merely 14% for advanced-stage gastric cancer.
The article “Incidence and Mortality of Stomach Cancer in China, 2014,” jointly published by the National Office for Cancer Prevention and Control, the National Cancer Center, and other institutions in Issue 3, 2018 of the Chinese Journal of Cancer Research, estimated the overall cancer burden in China in 2014 based on data from 339 cancer registries, covering approximately 21.07% of the national population:
Top 10 Cancer Types by Incidence and Mortality in China, 2014

Data source: Cancer incidence and mortality in China, 2014; VCBeat
Gastric cancer ranks second in incidence and third in mortality among all types of cancer in China, leading to the following conclusions:
In 2014, there were 410,400 newly diagnosed cases of gastric cancer nationwide, accounting for approximately 11% of all cancer incidences. The crude incidence rate was 30.00 per 100,000 population, while the age-standardized rates based on the Chinese standard population and the World Standard Population were 19.62 per 100,000 and 19.51 per 100,000, respectively. The term “Chinese age-standardized rate” refers to the incidence (or mortality) rate adjusted according to the Chinese standard population, whereas the “World age-standardized rate” refers to that adjusted according to the World Standard Population.
The incidence rate of gastric cancer in males is significantly higher than that in females, with the age-standardized incidence rate being 2.4 times that of females.
In 2014, there were 293,800 gastric cancer-related deaths nationwide in China, with a mortality rate of 21.48 per 100,000 population.
Both the incidence and mortality rates of gastric cancer are higher in rural areas than in urban areas.
Gastric cancer is one of the most common gastrointestinal malignancies, posing a serious threat to human life and health. According to the article “Cancer Statistics in China, 2015,” published in 2016 in the prestigious oncology journal CA: A Cancer Journal for Clinicians, estimates of cancer incidence in China for 2015 were based on data from 72 registry sites of the Cancer Registration Center covering 6.5% of the Chinese population during 2009–2011. The incidence rate has remained consistently high, with an estimated 679,100 new cases of gastric cancer and 498,000 deaths in China in 2015. Combined with the World Health Organization’s reported global figure of 754,000 gastric cancer deaths in 2015, China accounted for 66% of all gastric cancer deaths worldwide.
Estimated New Cancer Cases and Deaths in 2015 (Thousands)

Data source: Cancer Statistics in China, 2015
1.2 Gastrointestinal Diseases Are Showing a Trend Toward Younger Onset
Over the past six decades, the global incidence and mortality rates of gastric cancer have declined significantly due to improvements in sanitation and dietary conditions, as well as the widespread adoption of early prevention and screening programs. However, high-incidence regions remain concentrated in East Asian countries, with China alone accounting for more than half of all gastric cancer cases worldwide.
Regarding age-related differences in gastric cancer, the national incidence and mortality rates among men in China in 2015 both exhibited a spindle-shaped distribution. Rates increased with age, remaining at a low level among those under 30 years old, beginning to rise in the 30–44 age group, increasing rapidly among those aged 45 and above, peaking in the 60–74 age group, and declining among those aged 75 and older. Incidence and mortality rates were higher in men than in women within the same age groups. Specifically, the gastric cancer incidence rate among men aged 60–74 was more than twice that of women in the same period, and the mortality rate was 2.5 times that of women.
A comparison of cause-of-death statistics for residents across multiple years in the *China Health Statistics Yearbook* reveals that gastric cancer exhibits a trend toward affecting younger patients compared with other cancers. Although lung cancer has higher overall incidence and mortality rates than gastric cancer, the incidence of gastric cancer among young adults aged 20–25 years is even higher than that of lung cancer in some cases.
1.3 The Phenomenon of Self-Diagnosis and Self-Treatment for Gastric Diseases Is Prevalent
In recent years, driven by changes in China’s healthcare landscape and the growing consumer awareness of self-medication, a pattern has emerged in which serious conditions are treated at hospitals, minor ailments are managed in community health centers, and common medications are purchased at pharmacies. This trend, coupled with the rise in self-diagnosis and self-treatment of gastric disorders, has fueled the continuous expansion of the over-the-counter (OTC) gastrointestinal drug portfolio.
Gastrointestinal medications primarily consist of several major categories, including anti-ulcer and antacid agents, digestive aids, prokinetics, and antidiarrheals. The accelerating pace of modern life has led to changes in dietary habits, resulting in a higher incidence of gastrointestinal disorders with high recurrence rates. According to relevant data, the five-year recurrence rate ranges from 50% to 90%. To avoid the time spent queuing for registration, many consumers opt to purchase medications directly from retail pharmacies, causing some gastric conditions to miss the optimal treatment window and leading to further deterioration of the disease.
Currently, major gastric medications can be categorized into three main classes: proton pump inhibitors, H2 receptor antagonists, and gastric mucosal protective agents. It is evident that over-the-counter (OTC) options are available for each class, making self-diagnosis and self-treatment of gastric disorders the choice for the majority of individuals.

Data Source: Public Information, VCBeat
Comparison of Five-Year Survival Rates for Gastric Cancer in China, Japan, and South Korea
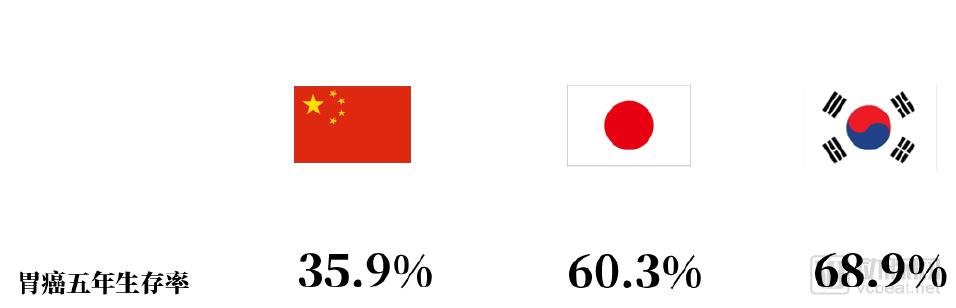
Data source: CONCORD-3
In contrast to the high incidence of gastrointestinal tumors, the early diagnosis rate remains low. Many gastrointestinal tumors have an insidious onset and are asymptomatic in the early stages; consequently, most patients are diagnosed at an advanced stage. A significant contributing factor is the lack of routine screening habits. Without early screening and diagnosis, patients often seek medical attention only after obvious symptoms appear, by which time the disease has typically progressed to an advanced stage.
According to the report on global trends in cancer survival from 2000 to 2014 published in The Lancet, namely the third round of global cancer survival analysis (CONCORD-3), there is a significant gap between our country and neighboring countries in terms of the 5-year survival rate for gastric cancer.
Japan and South Korea report high five-year survival rates for gastric cancer, primarily because most cases are detected at an early stage. Early-stage disease progresses more slowly, carries a lower risk of recurrence and metastasis, and, given patients’ younger age and better physical condition, allows for greater tolerance to surgery, radiotherapy, and chemotherapy, thereby yielding superior treatment outcomes. In Japan, 400,000 individuals underwent gastric cancer screening in 1964; this number rose to 4 million by 1970, and since the 1990s, approximately 6 million people have been screened annually. The early diagnosis rate for gastric cancer in Japan reaches as high as 50% to 70%. Given that Japan’s high gastric cancer cure rate is attributable to early detection and timely treatment, how has this been achieved?
Screening relies primarily on endoscopy. It is reported that Japan, with a population of approximately 127 million, performs around 15 million gastroscopies annually, equivalent to 12.5% of the population undergoing the procedure each year. In contrast, the gastroscopy rate in China is very low. According to Li Zhaoshen, Director of the National Center for Quality Control in Digestive Endoscopy, more than 6,000 medical institutions in China were performing endoscopic procedures in 2015. There were nearly 30,000 digestive endoscopists qualified to perform endoscopies, along with approximately 20,000 nurses responsible for endoscopy care, enabling the completion of 30 million digestive endoscopy cases per year. Nevertheless, there remains a significant gap in endoscopy rates compared to Japan and South Korea, particularly as screening for asymptomatic individuals is virtually nonexistent.
In 2005, China officially launched its first major national public health initiative for cancer prevention and control—the Early Screening and Treatment Project for Cancers in High-Incidence Rural Areas. This project primarily targets rural regions and areas with high cancer incidence, aiming to improve early diagnosis and treatment rates and reduce mortality for seven common high-incidence cancers in China, while providing single-cancer screening for specific populations.
Zhuanghe, Liaoning Province, serves as the demonstration base for early diagnosis and treatment of gastric cancer in this project. From 2008 to 2013, based on the local incidence of gastric cancer in the Zhuanghe area, cluster sampling was employed to identify townships with higher gastric cancer incidence rates as screening sites. Gastric cancer screening, along with early diagnosis and treatment, was conducted among high-risk individuals aged 40–69 years in these areas.
From 2008 to 2013, Zhuanghe conducted gastric cancer screening along with early diagnosis and treatment. A total of 9,328 individuals were screened, including 3,845 males (41.22%) and 5,483 females (58.78%). All participants underwent pepsinogen (PG) testing and gastroscopy. Among those who received gastroscopy, 6,132 underwent pathological examination. The results revealed 3,565 cases of non-atrophic gastropathy, 2,057 cases of atrophic gastritis, 454 cases of low-grade intraepithelial neoplasia, 19 cases of high-grade intraepithelial neoplasia, 25 cases of early-stage gastric cancer, and 12 cases of advanced-stage gastric cancer.
From the trend of gastric cancer incidence in the Zhuanghe region from 2004 to 2012, the world-standardized rates showed a
A significant downward trend was observed, with a slightly more pronounced decline in females than in males. The overall age-standardized incidence rate of gastric cancer decreased from 27.91 per 100,000 to 19.45 per 100,000, representing an average annual decrease of 4.02%. The mortality rate of gastric cancer also showed a significant downward trend, with a slightly more pronounced decline in females than in males. The overall age-standardized mortality rate of gastric cancer decreased from 30.05 per 100,000 to 13.53 per 100,000, representing an average annual decrease of 9.34%.
2.1 Data Overview
Currently, the National Urban Cancer Early Diagnosis and Treatment Program is underway, with cost-effectiveness analyses for gastric cancer screening still in progress. At present, there are two primary approaches for the diagnosis and examination of gastrointestinal diseases, particularly gastric cancer:
1. Conduct initial screening using serum pepsinogen (PG) testing and a risk factor questionnaire; individuals with positive results proceed to gastroscopy.
Second, directly perform gastroscopy and implement corresponding follow-up plans based on the screening results.
Regardless of the screening method employed, endoscopy remains the “gold standard” for diagnosing gastrointestinal diseases. During the preparation of this report, Anhan Technology (Wuhan) Co., Ltd. and Shanghai Anhan Medical Technology Co., Ltd. (hereinafter referred to as “Anhan Company”) provided us with de-identified capsule endoscopy reports from 100,000 patients. This large-scale endoscopic dataset enabled us to analyze the current status of gastric diseases in China, allowing for a more granular assessment of gastric disease patterns and an understanding of the incidence of gastrointestinal diseases under novel gastroscopic examination techniques.
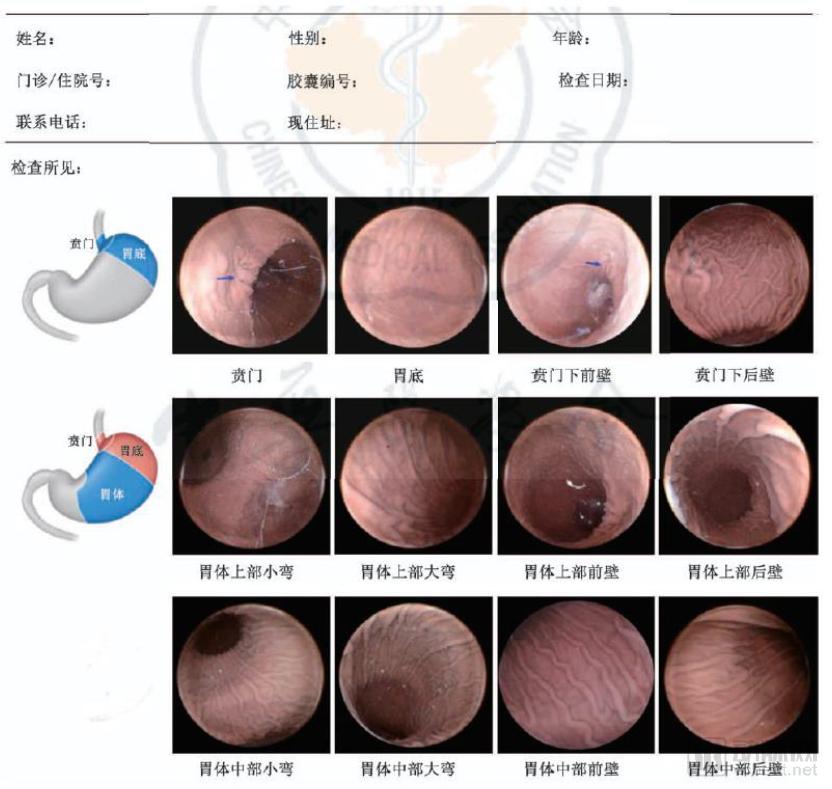
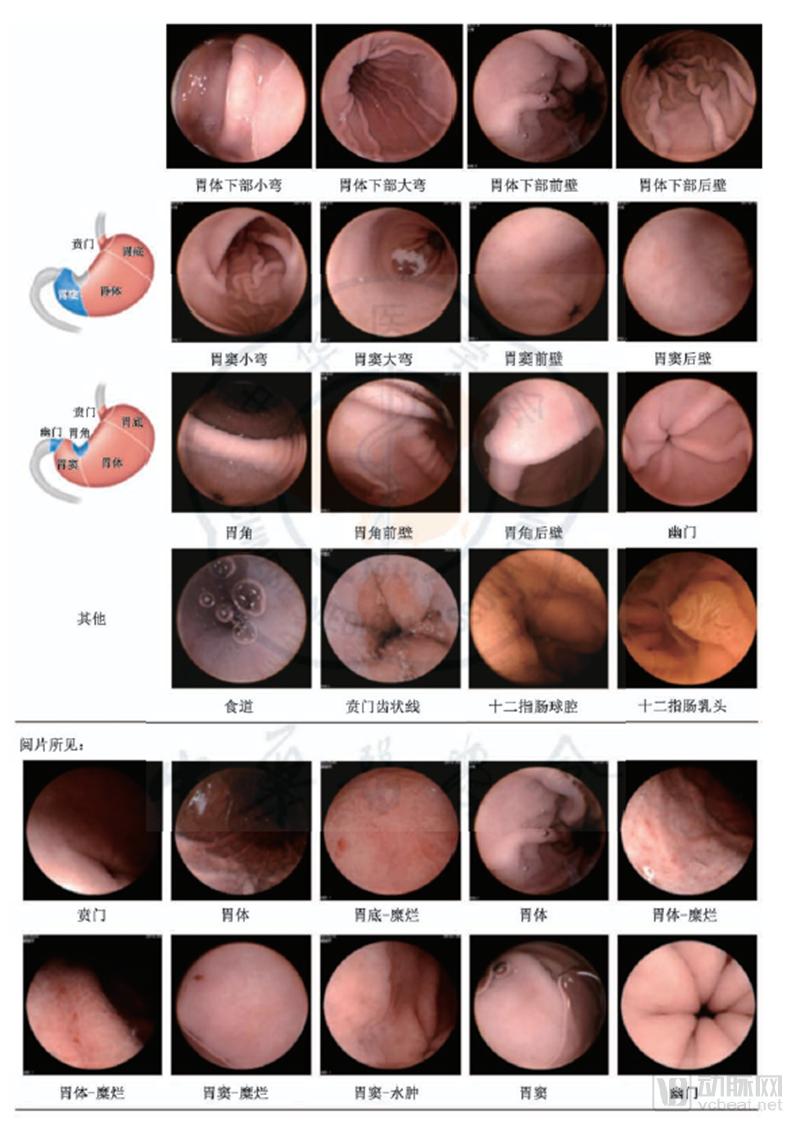
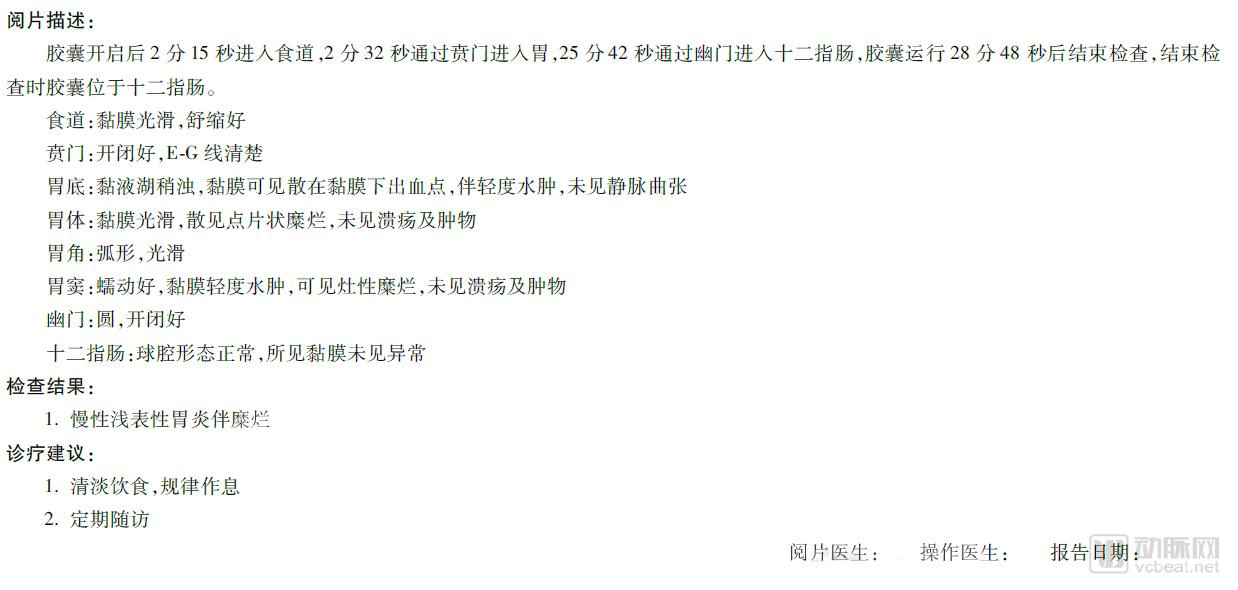
a)Report Example
b) Overview of Sample Data
Sample size: 100,000 cases, participants in the Anhan “Magnetic-Controlled Capsule Gastroscopy” system from January 2017 to June 2018
Randomly selected from patients undergoing examination
Each data record includes: ID, gender, age, examination date, city, and examination results.
Research Process:
1. Organize the data and exclude samples with significant deviations in age, gender, or test results.
2. Map cities to provinces for statistical analysis
3. Structure non-standardized test results by disease site, disease category, and disease progression stage
4. Data Statistics: Grouped statistical analysis of structured data
5. Data Analysis: Comparative analysis of statistical results
C) Sample Patient Profile
Patient Sources: The patients in this dataset were primarily recruited from two channels: hospitals and health examination institutions.
Patient Age Distribution: In this sample, patients were predominantly middle-aged and young adults, with a notable gap at age 56, which may be attributed to patient referral sources and the cost of capsule endoscopy.
Age Distribution of Sample Subjects
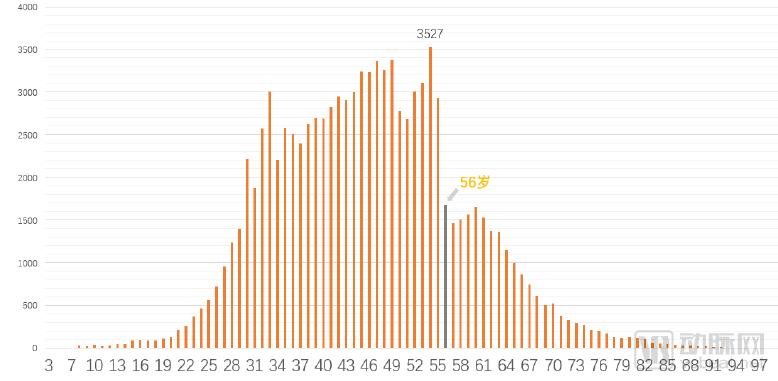
Data sources: Anhan Company, VCBeat
Patient Gender: In the current sample data, male patients accounted for 58.50% and female patients for 41.49%, which is similar to the general population distribution.
Gender Statistics of Sample Subjects
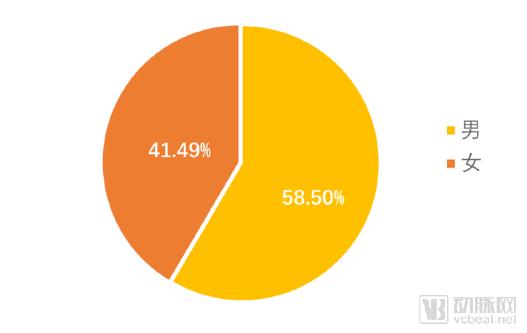
Data source: Anhan Company, VCBeat
Geographic Distribution: The inspection sites in this sample covered 31 provinces, municipalities, and autonomous regions across China. Guangdong Province and Beijing ranked in the first tier in terms of sample size, while populous provinces such as Shandong, Sichuan, and Henan, along with the Yangtze River Delta region, fell into the second tier. This disparity indirectly reflects variations in the consumption capacity for capsule endoscopy across different provinces and municipalities.
Figure 8: Geographic Distribution of Sample Subjects
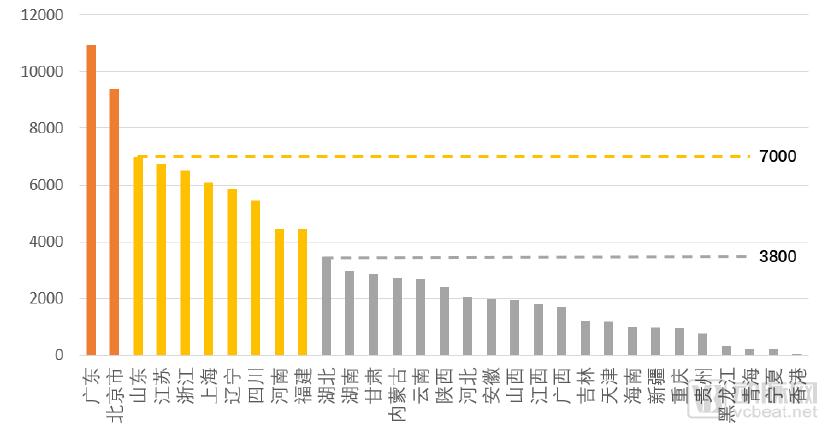
Data Source: Anhan Medical, VCBeat
Sample Inspection Scenario: The usage scenarios for capsule endoscopy are divided into two categories: health check-ups (including private health examination centers and public hospital health examination centers) and gastroenterology consultations (including public hospitals and private hospitals), with an approximate ratio of 9:1.
Statistics on Sample Subject Examination Scenarios
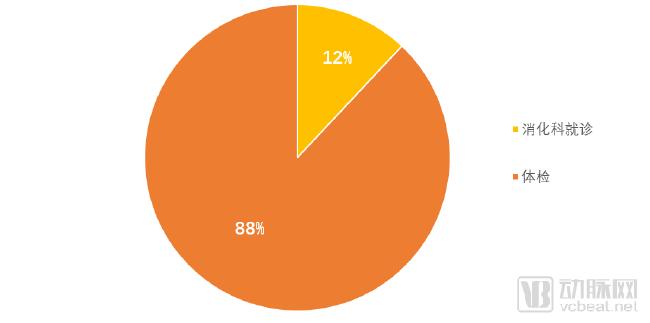
Data source: Anhan Company, VCBeat
Examination Period: The samples in this study primarily consist of patients who underwent capsule endoscopy between 2017 and June 2018. The number of examinations fluctuated significantly, influenced by factors such as the pace of capsule endoscopy adoption and holidays like the Spring Festival.
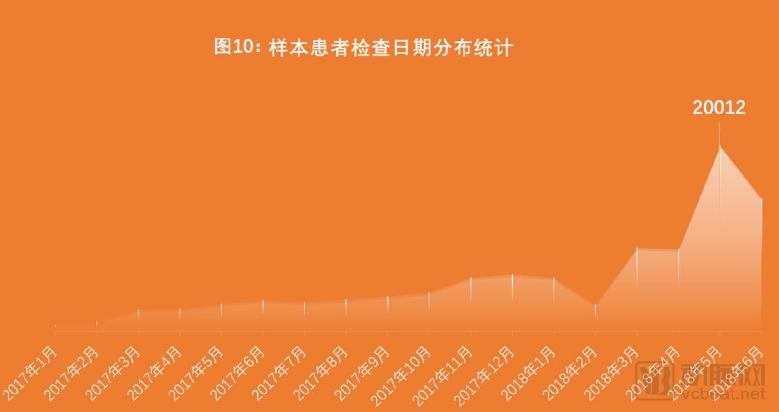
Data sources: Anhan Company, VCBeat
2.2 Spectrum of Upper Gastrointestinal Diseases
2.2.1 Anatomical Distribution of Upper Gastrointestinal Diseases
Analysis by anatomical site reveals that gastric diseases are predominantly localized to the gastric antrum, accounting for over 15% of cases. Meanwhile, the esophagus, duodenum, and small intestine also exhibit high prevalence rates within the gastrointestinal tract and should be carefully evaluated during examination.
Statistics on the Anatomical Locations of Digestive Tract Diseases
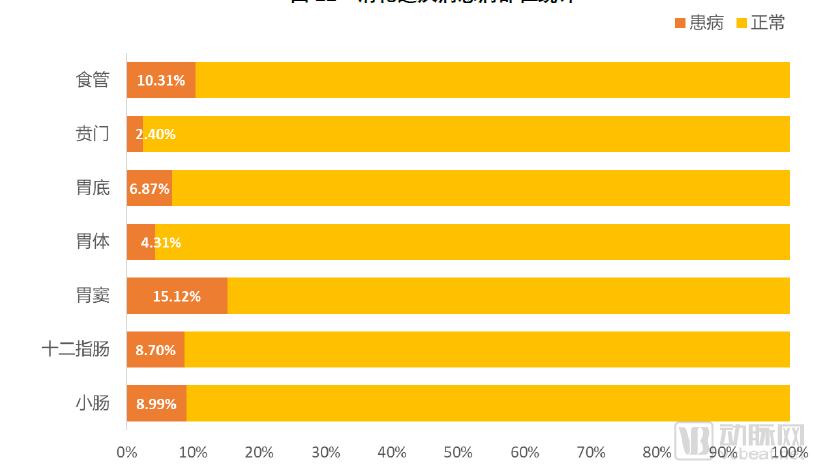
Data Source: Anhan Company, VCBeat
2.2.2 Statistics on the Nature of Diseases by Body Part
As the site with the highest prevalence, over 50% of diseases in the gastric antrum are erosions, with the probability of accompanying atrophic changes approaching 30%. We analyzed the nature of diseases across six anatomical sites—the gastric antrum, gastric fundus, cardia, gastric body, duodenum, small intestine, and esophagus—and found that erosion, atrophy, and polyps are the three most prevalent pathological findings in gastrointestinal disorders. (For details, please refer to the full report.)
2.2.3 Geographic Distribution of Upper Gastrointestinal Diseases
We analyzed the regional distribution of upper gastrointestinal disorders. Contrary to traditional perceptions, Sichuan, Chongqing, and Hunan—regions known for their heavy oil and spicy cuisine—did not exhibit high prevalence rates. Instead, higher prevalence was observed in northwestern regions such as Shaanxi and Ningxia. We hypothesize that this may be associated with factors including dietary habits and climate.
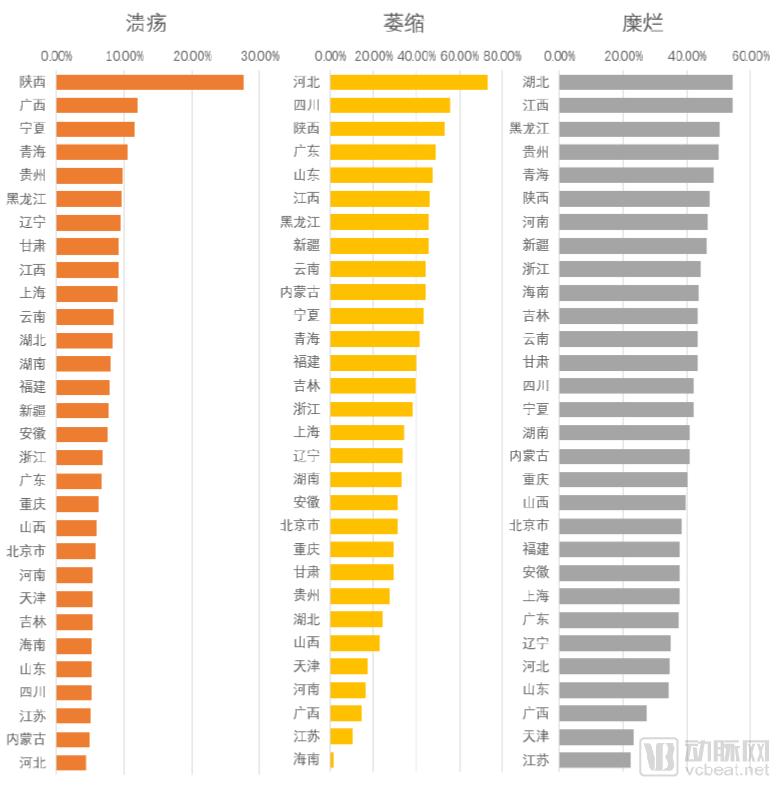
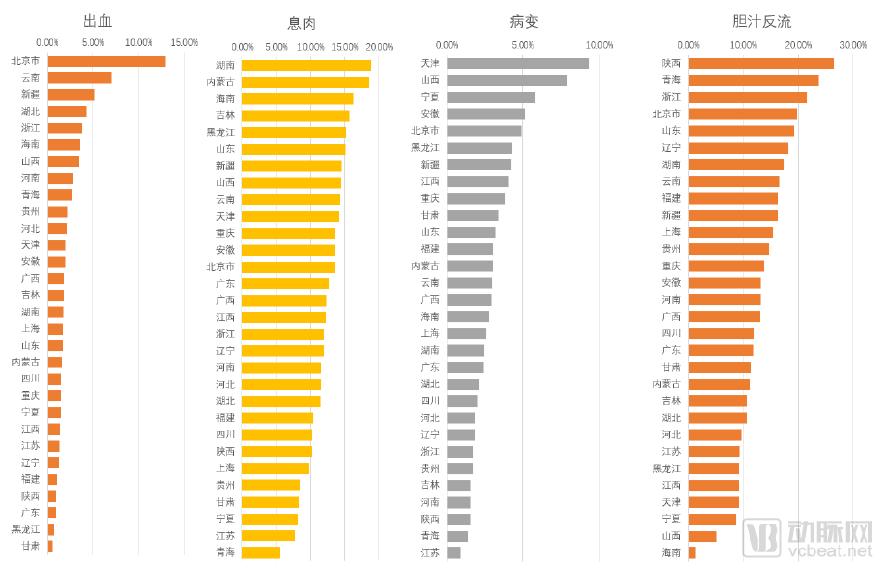
Data sources: Anhan Company, VCBeat
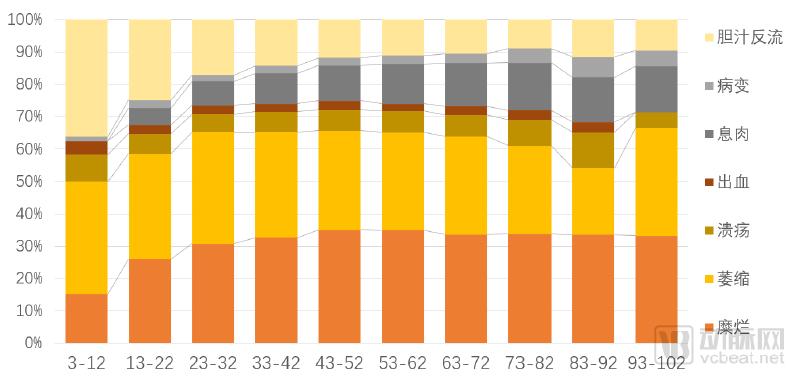
2.2.4 Age Distribution of Upper Gastrointestinal Diseases
We stratified the sample population into groups using a 10-year age interval, yielding the following distribution of disease phenotypes across age groups. As shown, the prevalence of erosive diseases rises rapidly between ages 0 and 30 and stabilizes after age 40, whereas atrophic diseases exhibit an opposite trend. Notably, the incidence of polypoid diseases continues to increase with advancing age.
Statistics of Digestive Tract Diseases by Age Group
Data Source: Anhan Company, VCBeat
2.3 Data Analysis of Severe Gastric Diseases
We screened out samples containing "CA," "cancer," or "tumor" in their reports to serve as study samples for severe gastric diseases. Among 100,000 samples, 149 reports included these three diagnostic findings, with 114 from males and 34 from females. The incidence rate of severe gastric disease in males was three times that in females, which may be related to men’s daily dietary habits and work-related stress. Specifically, by age group, men enter a high-incidence period for gastric cancer after the age of 30, while the number of female patients begins to increase only among those aged 40 and above. It is recommended that individuals undergo regular gastric examinations according to their respective age groups.
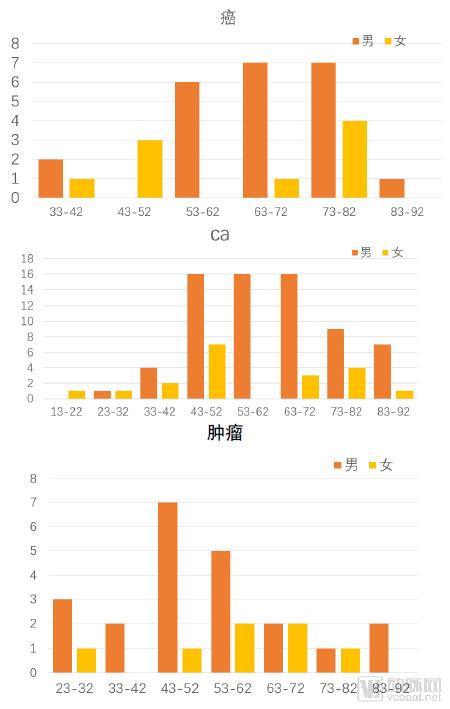
Data Source: Anhan Company, VCBeat
Note: The above data presents preliminary analysis results for short-term gastrointestinal diseases and may contain imperfections; related research is progressively advancing.
3.1 Differentiation of Electronic Endoscopy and the Emergence of Capsule Endoscopy
Current electronic gastroscopy technology is advancing rapidly, with conventional gastroscopy evolving into painless gastroscopy and capsule gastroscopy. Compared to traditional gastroscopy, these two endoscopic examination methods offer a better patient experience.
Capsule endoscopy, fully known as the Intelligent Capsule Gastrointestinal Endoscopy System and also referred to as medical wireless endoscopy, is essentially a camera-equipped capsule slightly larger than conventional oral capsules. During the examination, the patient swallows the intelligent capsule with water, similar to taking medication. The capsule then traverses the various structures of the gastrointestinal tract—esophagus, stomach, duodenum, jejunum and ileum, colon, and rectum—either following the peristaltic rhythm of the gastrointestinal muscles or under external control. Throughout this process, it continuously captures images of the gastrointestinal tract. Standard capsule endoscopes can operate for 6–8 hours. Physicians assess the patient’s gastrointestinal condition by reviewing the captured images. The capsule is typically excreted from the body within 1–3 days after ingestion.
Capsule endoscopy, first invented by Israeli scientists in 2000, has become the first-line diagnostic method for small bowel diseases after nearly two decades of development. With the emergence of new types of capsule endoscopes, the indications for capsule endoscopy have expanded from the small intestine to the esophagus, colon, and even the stomach. For instance, both esophageal and colonic capsule endoscopes have entered clinical application, with colonic capsule endoscopy having received FDA approval in the United States. However, capsule endoscopy is not suitable for diagnosing gastric diseases because traditional capsule endoscopes rely on gravity and gastrointestinal peristalsis for passive movement, capturing random images of the digestive tract mucosa. This approach fails to provide comprehensive and effective imaging of the gastric cavity, which offers a larger space compared to the small intestine.
To achieve the goal of gastric examination using capsule endoscopy, effective gastric distension and active control of the capsule endoscope are essential. Gases such as air or carbon dioxide, which are used in conventional electronic gastroscopy, are not suitable for capsule gastroscopy because air escapes from the stomach through the cardia. Therefore, water filling can be employed to distend the stomach and flatten its rugae, thereby facilitating observation and imaging by the capsule endoscope. Additionally, further gastric distension can be achieved by ingesting powder that generates carbon dioxide.
Achieving actively controlled, multifunctional capsule robots for the gastrointestinal tract is currently a major research focus worldwide. There are two primary approaches to the active control of capsule endoscopes: internal drive and external drive. The clinical application of the internal drive mode is limited by the need for extensive ethical review regarding its feasibility, making it difficult to popularize. The mainstream approach for external drive relies on extracorporeal magnetic field control, which currently comprises three main categories of magnetic control methods: handheld, magnetic resonance imaging (MRI) coil-based, and robotic arm-based magnetic control. Among these, the first two methods have not yet been formally approved for clinical use in gastric examinations.
Major Capsule Endoscopy and Examination Scope

Source: Public information, VCBeat Eggshell Research Institute
China has pioneered the development of the world’s first magnetically controlled capsule gastroscopy system, which utilizes a robotic arm for precise multi-dimensional rotation and movement, along with adaptive matching to achieve accurate control [NaviCam magnetically controlled capsule gastroscopy system, Anhan Technology (Wuhan) Co., Ltd. and Shanghai Anhan Medical Technology Co., Ltd.]. This system employs a C-shaped robotic arm-style permanent magnet outside the body to precisely maneuver and control the capsule within the gastric cavity. Clinical studies have confirmed its high diagnostic accuracy. It has obtained the registration certificate for the “Magnetially Controlled Capsule Gastroscopy System” from the China Food and Drug Administration (CFDA) (Registration No.: Guo Xie Zhu Zhun 20173223192) as well as EU CE certification, making it currently the only magnetically controlled capsule gastroscopy system applied in clinical practice.
The permanent magnet application intensity of the Anhan “Magnetic Controlled Capsule Gastroscope” system is approximately 200 Gauss (1/100 of the MRI magnetic field strength). Through precise external magnetic control, it achieves millimeter-level small-step (2mm) translation in three-dimensional linear directions, allowing the capsule gastroscope to be accurately aligned with specific areas.
Anhan "Magnetically Controlled Capsule Gastroscopy" System

Image source: Anhan Company, VCBeat
Capsule Endoscopy System: Primarily Composed of Three Components:
(1) Capsule endoscopy refers to the imaging component; after being swallowed by the patient, it captures images and transmits them to an image recorder.
(2) Image recorder, commonly designed as a wearable vest worn by the patient during examination; some are about the size of a radio and carried on the patient’s back to receive and record images captured by the capsule endoscope. Physicians retrieve the recorded images to assess conditions within the patient’s gastrointestinal tract.
(3) Control Equipment: The translation-rotation stage and control console, composed of a C-arm magnet and a control unit, are used to precisely control the movement of the capsule within the stomach across five degrees of freedom.
Physicians performing capsule endoscopy procedures can be general practitioners, while image interpretation is typically conducted by senior physicians with both clinical and endoscopic expertise. This is primarily because capsule endoscopy is mainly used to examine gastric and small bowel lesions; although small bowel diseases are relatively rare, they encompass a wide variety of pathologies. Only senior physicians with combined clinical and endoscopic experience can minimize missed diagnoses and misdiagnoses to the greatest extent.
4.1 The Impossible Trinity Model Preceding Gastroscopic Screening

Image source: VCBeat
In most healthcare scenarios, improving the quality of care, increasing access to medical services, and lowering the cost of care cannot be achieved simultaneously without breaking existing rules; we refer to this as the “Healthcare Impossible Trinity Model.”
The only solution to this medical trilemma is the introduction of new technological increments. The emergence of new technologies will transform operational models, industrial structures, and institutional arrangements. Their advent will trigger extensive adjustments in prices and production networks within the economic system. Controllable capsule endoscopy technology is precisely such a technology.
In the gastric cancer screening protocols of Japan and South Korea, gastroscopy serves as the critical final step for definitive diagnosis, playing a pivotal role. China has also incorporated endoscopic examination into its technical manual for gastric cancer screening. However, there is a significant disparity in endoscopy penetration rates between China and Japan. This gap stems not only from differences in economic development and public awareness but also from objective challenges dictated by factors such as population size, medical resource availability, and geography. Conventional organizational approaches have proven unable to break this “impossible triangle.” The emergence of controllable capsule endoscopy offers a technological solution that brings hope to this endeavor, which has long been constrained by multifaceted difficulties, thereby making the large-scale promotion of endoscopic screening feasible.
4.2 Technology Transforms the Landscape of Gastroscopy, Exponentially Enhancing Accessibility to Gastric Examinations
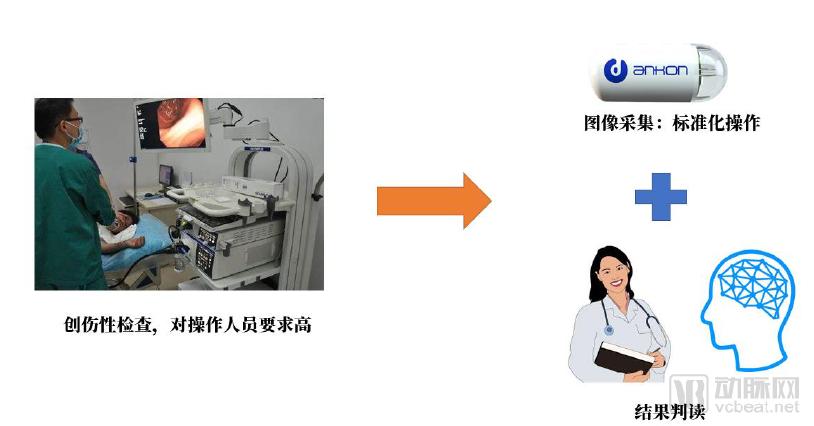
Image source: VCBeat
Conventional gastroscopy is an invasive procedure associated with a high “pain index,” prone to causing tissue trauma, and carrying a risk of cross-infection. The procedure poses risks of mechanical injury, must be performed by specialized physicians, and is considered a “quasi-surgical” examination. In contrast, while maintaining accuracy highly consistent with that of conventional electronic gastroscopy, capsule endoscopy is extremely simple to operate, and the image acquisition process does not require the involvement of specialized physicians. Furthermore, capsule endoscopy features such advantages as being painless, non-invasive, anesthesia-free, and free from the risk of cross-infection, making it better suited for patients with poor compliance, contraindications to anesthesia, susceptibility to mucosal bleeding, or high infectivity. Additionally, during conventional gastroscopy, patients often experience adverse reactions such as nausea, vomiting, and abdominal distension, leading to reluctance or fear toward undergoing the examination. Capsule endoscopy can effectively avoid these adverse reactions, thereby alleviating patients’ fear of gastroscopic examinations.
Comparison Between Traditional Gastroscopy and Capsule Endoscopy
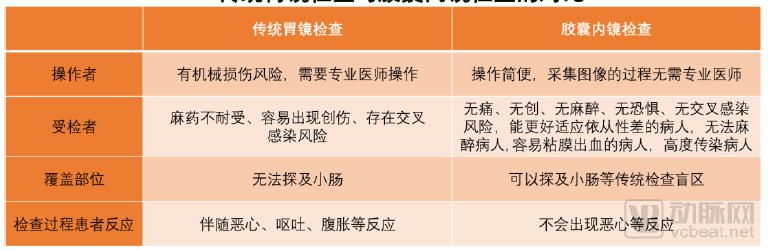
Data source: Public information, VCBeat.
The capsule endoscope focused on small intestine examination was first successfully developed and brought to market by Israel’s Given Imaging in 2000. After being swallowed, the pill-sized capsule advances through the digestive tract via peristalsis, capturing images of the small intestine to diagnose mucosal lesions. This is a painless and non-invasive endoscopic examination method. However, small intestine capsule endoscopes operate passively; they cannot be actively controlled and move only with natural intestinal peristalsis. For large hollow organs such as the stomach, imaging is limited to whatever areas the capsule happens to pass through, rather than allowing targeted visualization, thereby precluding comprehensive gastric examination. Consequently, many universities, research institutions, and companies have invested in the development of actively controlled capsule endoscopes, yet no breakthrough progress has been achieved to date.
Since 2009, Anhan has pioneered a magnetically controlled capsule methodology that enables stable and precise maneuvering and rotation of the capsule within the gastric cavity. The company also invented techniques for achieving stable suspension and movement of the capsule in gastric fluid. By leveraging a five-axis robotic magnetic control system and sensor feedback from the capsule endoscope, Anhan developed algorithms that allow for comprehensive, no-miss examination of the gastric mucosa. Anhan is the first company globally to obtain clinical registration approval for a magnetically controlled capsule endoscopy system. It is also the first to complete multicenter, double-blind clinical trials comparing its technology with conventional gastroscopy, thereby confirming the safety and efficacy of capsule endoscopy. The related clinical studies were published as cover articles in *Clinical Gastroenterology and Hepatology* (CGH), the official journal of the American Gastroenterological Association. In addition to direct manual control via a joystick, the control system supports an intelligent automatic cruising function that actively adjusts the capsule’s position and posture. Utilizing artificial intelligence for image recognition and real-time feedback, the system enables a complete gastric examination in a painless and non-invasive manner. It is particularly suitable for upper gastrointestinal health check-ups and early screening for gastric cancer.
Magnetic-Controlled Capsule Gastroscopy Product Portfolio

Image source: Anhan Medical, VCBeat
The magnetically controlled capsule gastroscopy system consists of five components: the magnetic control capsule endoscopy control system, the magnetically controlled capsule gastroscopy robot, the examination gown, the capsule locator, and the display software.
The control system employs remote-controlled magnetic field technology, enabling a series of maneuvers such as horizontal and vertical rotation, diving, jumping, hovering, and U-turns of the capsule within the body via a joystick. As long as the patient actively cooperates with the operator by changing body positions, blind-spot-free scanning of any location in the stomach can be achieved. In contrast, traditional capsule gastroscopy relies on natural peristalsis of the human digestive tract for propulsion, preventing operators from actively controlling the capsule’s position within the patient’s body. This often results in blind spots during gastric examinations, thereby limiting diagnostic accuracy.
The capsule endoscopy robot measures approximately 27 mm in length and 11.8 mm in width, weighs 5 grams, and contains over 300 components. It employs an automatic frequency-modulated imaging mode to capture images of the gastrointestinal tract, which are then transmitted wirelessly to an external receiver for storage. The magnetically controlled capsule is ingested with water, mimicking the normal eating process; this ensures that gastric kinetic changes resemble physiological gastric motility, thereby providing a more accurate representation of real stomach movement and creating an optimal environment for examination. As a single-use device, the capsule is naturally expelled from the body through the digestive tract after the procedure, effectively minimizing the risk of disease transmission.
Examination Vest (also known as a Portable Recorder): Easy to wear, with adjustable buckles to accommodate patients of different body sizes; data storage capacity exceeds 4 GB, enabling continuous operation for more than 8 hours.
The capsule locator utilizes magnetic scanning localization technology to detect in real time whether the magnetically controlled capsule gastroscope remains within the body, offering a safe and radiation-free alternative. In contrast, traditional capsule endoscopy relies on abdominal imaging for detection, which exposes patients to X-ray radiation.
The monitor can display the movement trajectory and status changes of the magnetically controlled capsule in real time, facilitating precise control by the operator.
As the magnetic-controlled capsule gastroscopy system employs minimal magnetic force, it is highly safe and eliminates the risk of mechanical injury associated with traditional gastroscopy. This significantly lowers the operational requirements for medical personnel, facilitating the widespread adoption of gastric examinations. The capsule gastroscopy offers a novel solution for patients with poor compliance to conventional endoscopy, those who cannot undergo anesthesia, individuals prone to mucosal bleeding, and patients with highly contagious diseases. Particularly in the realm of health screening, robotic capsule gastroscopy has gained widespread popularity among the general public due to its painless, non-invasive, and convenient nature. It addresses the critical challenge in China, where the high incidence of gastric cancer is compounded by inadequate diagnostic capabilities and a lack of early screening mechanisms, thereby serving as a powerful tool for the early prevention, control, and treatment of gastric cancer.

Image source: VCBeat
The key feature of asynchronous and spatiotemporally decoupled capsule gastroscopy divides the procedure into two distinct processes: image acquisition and diagnosis. Advances in internet technology enable these two stages to occur at different times and locations, transforming image acquisition into a simple, standardized operation. Patients only need to swallow the capsule at the front end, while high-quality medical resources at the back end can interpret the gastric images, thereby exponentially improving the accessibility of gastroscopic examinations.
Image review for capsule endoscopy consumes significant time and effort from physicians, as each examination generates tens of thousands of capsule endoscopy images. Frame-by-frame interpretation for diagnosis poses a considerable time challenge even for top-tier endoscopists, while presenting substantial technical difficulties for operators of magnetically controlled capsule gastroscopy at lower-tier hospitals or health checkup centers. Therefore, leveraging internet technology, a remote image review platform has been established. This platform enables real-time upload of data from various high-end health checkup centers to the remote capsule endoscopy image review system. Experienced endoscopists can flexibly schedule image reviews according to their availability, allowing a limited number of diagnostic experts to interpret images anytime and anywhere, thereby addressing the technical shortcomings in image interpretation at health checkup centers and lower-tier hospitals. Furthermore, the remote image review platform aggregates tens of thousands of examination records nationwide. AI-powered intelligent image review technology, developed through big data analysis, mining, and training, enables automatic image review and annotation of suspicious lesions for physician verification, significantly improving the efficiency of image interpretation.
Anhan has conducted research in the field of intelligent image interpretation, leveraging globally leading gastrointestinal imaging acquisition technologies, “Internet Plus,” and artificial intelligence. Building upon capsule endoscopy, the company enables the acquisition, secure transmission, and cloud storage of gastrointestinal medical images, providing them to physicians’ mobile terminals for remote review. By employing deep learning techniques and utilizing massive image datasets for modeling and training on typical lesions, Anhan has developed an auxiliary diagnostic software suite that offers significant clinical value to physicians.
Anhan Intelligent Image Reading Cloud Platform
Data source: Anhan Company, VCBeat
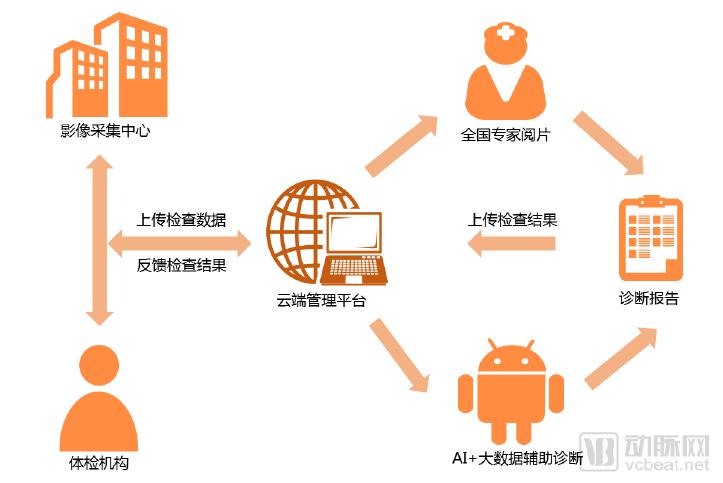
Patients ingest the capsule at nearby physical examination centers, where staff operate the controlled capsule endoscopy system to perform gastroscopy. The imaging acquisition center collects gastroscopy images from various physical examination institutions (or hospital-based health checkup centers), categorizes and structures the data, and then uploads the processed images to a remote management platform. The cloud-based management platform receives and stores these images. Experts from across China log into the cloud platform to remotely review the images, aided by AI and big data-assisted diagnostic software, and issue gastroscopy diagnostic reports for the respective patients. Finally, the diagnostic reports are transmitted back via the cloud platform to the offline institutions, providing a scientific basis for local physicians’ diagnoses.
This technology enables end-to-end quality control and comprehensive screening for lesions throughout the entire gastrointestinal tract. Built on a technical foundation of endoscopic image acquisition, storage of images and structured medical data, cloud computing, and data mining, it is scalable to networked systems. By enhancing the utilization efficiency of high-end medical resources through remote image interpretation, it pioneers a new service model of “local examination, remote diagnosis and treatment.” This approach prioritizes resolving the bottleneck of limited medical resources for gastrointestinal examinations despite a large population requiring screening, breaks through geographical constraints in the distribution of medical resources during large-scale gastrointestinal population screenings, further expands incremental markets, and captures market share in domestic Grade A tertiary hospitals and international high-end markets.
5.1 Flexible Configuration to Enhance the Effectiveness of Utilizing Limited Medical Resources
Currently, China’s healthcare resources lag behind its economic development in both total volume and per capita terms. Specifically, for upper gastrointestinal examinations, there is an even smaller number of physicians capable of performing conventional electronic gastroscopy.
Data from the “100-Village Observation” longitudinal survey conducted by the China Institute for Rural Studies at Central China Normal University show that in 2014, China had 0.88 clinics, 1.44 medical personnel, and 2.33 hospital beds per 1,000 people. These figures reveal a significant gap compared with developed countries.
The shortage is even more acute when it comes to the number of specialists performing gastroscopy. Li Zhaoshen, Director of the Department of Gastroenterology at Changhai Hospital Affiliated to the Second Military Medical University and President of the Endoscopist Branch of the Chinese Medical Doctor Association, once stated that, based on projections, if the screening rate reaches 10%, China will have a population of 120 million requiring endoscopic examination by 2030. Given that there are currently 10,000 hospitals in China, completing endoscopic screening for this population would require at least 200,000 specialized digestive endoscopy physicians. However, China currently has fewer than 40,000 such specialists.
Physician training is characterized by its long duration and high costs. The traditional process of acquiring images with electronic gastroscopes is cumbersome and time-consuming, limiting the number of patients each physician can examine per day.
The complex and highly technical nature of traditional electronic gastroscopy results in low operational efficiency and suboptimal utilization of limited medical resources. Capsule endoscopy decouples the gastroscopic examination into two distinct processes: image acquisition and diagnosis. By transforming image acquisition into a simple, standardized procedure that can be performed by general healthcare personnel, physicians can focus exclusively on the diagnostic phase, thereby significantly enhancing the effectiveness of medical resource utilization.
5.2 Reshaping the Competitive Landscape of the Existing Market: Leveraging Incremental Market Space to Disrupt Traditional Markets
As previously mentioned, conventional electronic gastroscopy is highly specialized. Since gastroscopy is an invasive procedure, it can only be performed by qualified physicians. Currently, China has not yet implemented large-scale population-based screening programs for gastric cancer; instead, gastroscopy is primarily conducted on an opportunistic basis among symptomatic outpatients. Under traditional electronic gastroscopy techniques, it is challenging to significantly increase the volume of examinations, thereby confining the existing gastroscopy market largely to hospital settings. Capsule endoscopy standardizes the gastroscopy process, enabling operation by general healthcare personnel and thus improving accessibility.
Internet technology shifts the diagnostic process to a remote setting, enabling asynchronous image acquisition and diagnosis across different times and locations. This allows physicians to focus exclusively on diagnosis, significantly improving the efficiency of medical resource utilization. The characteristics of capsule endoscopy make it possible to decentralize gastroscopy services, transforming patient mobility into data flow.
By establishing deployment points in health checkup centers and general medical institutions, the traditional scenario limitations of gastroscopy are being broken, thereby opening up an incremental market for early gastric cancer screening. The technological evolution path of capsule endoscopy is destined to surpass existing electronic gastroscopes in terms of image acquisition, biopsy sampling, and other functions and outcomes. As their functionalities converge, capsule endoscopy will cannibalize the hospital market share of electronic gastroscopes.
5.3 Health Economic Value of Early Screening for Gastric Cancer
Cancer screening is an effective approach for the early detection of cancer, improving patients’ quality of life, and extending survival. However, not all cancers are suitable for screening, as some screening methods have limited sensitivity, are relatively costly, may cause certain trauma, and effective treatments are lacking for certain cancers. Furthermore, given the limited healthcare resources, the formulation of cancer screening strategies must adhere to the principle of cost-effectiveness.
Cancers currently recognized as suitable for screening include cervical cancer, colorectal cancer, and breast cancer. Screening strategies for these cancers are relatively mature, with recommended screening protocols supported by cost-effectiveness analyses. For other high-incidence cancers such as lung cancer, liver cancer, esophageal cancer, prostate cancer, and thyroid cancer, researchers have conducted exploratory population-based screening studies, and reports on cost-effectiveness evaluations are available. However, due to various reasons, these cancers have not yet been included in the list of recommended screenings. In recent years, many researchers have employed computer simulation methods to perform cost-effectiveness analyses of screening protocols for different cancers. The findings from these studies provide a basis for countries worldwide to select appropriate screening strategies tailored to their national contexts.
The prognosis of gastric cancer is closely related to the timing of diagnosis and treatment, with significant differences in five-year survival rates among patients at different stages. Early detection, early diagnosis, and early treatment are the most fundamental approaches to reducing mortality from gastric cancer.
A key measure to improve the health economic benefits of gastric cancer screening is the rational and accurate selection of screening targets, thereby minimizing the proportion of “ineffective screenings.” However, due to the complex etiology of gastric cancer and limited epidemiological data, it is difficult for clinicians to determine the precise incidence rates under the influence of various risk factors. Consequently, accurately defining the “high-risk population” remains challenging.
Currently, approximately 90% of gastric cancer cases identified in China are at an advanced stage. The prognosis of gastric cancer is closely related to the timing of diagnosis and treatment. Even with surgical intervention, the five-year survival rate for advanced gastric cancer remains below 30%, whereas the five-year survival rate for early-stage gastric cancer after treatment can exceed 90%, potentially achieving a cure. The five-year relative survival rate for gastric cancer patients in China from 2010 to 2014 was 35.9%. According to CONCORD-3 reports, the five-year net survival rates for gastric cancer patients in South Korea and Japan during the same period were 68.9% and 60.3%, respectively. There is still a notable gap between China’s gastric cancer survival rates and those of these countries, likely due to the higher proportion of late-stage diagnoses in China. Prognosis is tightly linked to the stage at diagnosis and treatment. Studies indicate that even with comprehensive treatment primarily involving surgery, the five-year survival rate for advanced gastric cancer remains under 30%. In contrast, most cases of early-stage gastric cancer can be radically treated via endoscopy, with five-year survival rates exceeding 90%. Therefore, greater emphasis should be placed on gastric cancer screening to enable timely detection and appropriate treatment at early stages, thereby extending patient survival and improving quality of life.
Since the 1990s, China has implemented primary prevention and secondary prevention strategies centered on screening in regions with a high incidence of gastric cancer, aiming to improve early diagnosis rates and reduce both the incidence and mortality of gastric cancer through screening of high-risk populations. Sequentially adopted approaches have included initial screening using serum pepsinogen followed by endoscopic examination for high-risk individuals, as well as direct endoscopic screening. Comparative studies of these two screening strategies have demonstrated that direct endoscopic screening significantly improves the detection rate of lesions, and its use is recommended for screening programs in areas with a high incidence of gastric cancer.
The technical protocol for the pilot program on screening, early diagnosis, and early treatment of upper gastrointestinal cancers in China, implemented in 2014, recommended direct gastroscopy as the screening method for gastric cancer in the general population. In recent years, studies conducted in high-incidence areas have demonstrated that endoscopic screening for gastric cancer in rural regions with a high prevalence of upper gastrointestinal malignancies yields significant benefits, markedly improving the rate of early diagnosis. Currently, countries such as Japan and South Korea have implemented gastric cancer screening programs. Asymptomatic patients detected through these screenings are typically at an early stage of cancer, exhibit better survival outcomes compared to those diagnosed outside of screening programs, and experience a corresponding reduction in mortality. The "Three-Year Action Plan for Cancer Prevention and Control in China (2015–2017)" explicitly states that it is necessary to promote and refine strategies for cancer screening, early diagnosis, and early treatment in China, expand the coverage of these initiatives, and strive to achieve an early diagnosis rate of 50% for key cancers in priority regions.
Therefore, implementing early gastric cancer screening measures in the general population and conducting precise endoscopic examinations for high-risk groups represent feasible and highly effective approaches to improving the severe situation of gastric cancer diagnosis and treatment in China. However, only South Korea and Japan currently have relatively comprehensive systems for gastric cancer prevention and screening. An analysis of gastric cancer incidence and mortality rates in Asia in 2012 showed that South Korea, Mongolia, and Japan ranked in the top three for age-standardized incidence rates, while Mongolia, Tajikistan, and Kyrgyzstan ranked in the top three for age-standardized mortality rates. It is evident that although Japan and South Korea have high gastric cancer incidence rates, their mortality-to-incidence ratios are significantly lower than those in Western countries. A plausible explanation is that both countries rank among the world leaders in gastric cancer screening, early diagnosis, and treatment. In particular, Japan has long maintained a global leading position in the endoscopic diagnosis and treatment of early gastric cancer. Consequently, its current practices and standards warrant our attention and study.
5.4 Analysis of the Benefits of Gastric Cancer Screening
Historically, the combined use of serum pepsinogen (PG) and Helicobacter pylori (Hp) antibody testing (known as the “ABC method”) has been employed to assess gastric cancer risk and identify high-risk populations. In this method, PG positivity is defined as PG I ≤ 70 μg/L and a pepsinogen ratio (PGR) ≤ 3, while Hp positivity is defined as a serum Hp antibody titer ≥ 30 U/mL. Based on serological test results, the screened population is stratified into four groups: Group A [Hp(−) PG(−)], Group B [Hp(+) PG(−)], Group C [Hp(+) PG(+)], and Group D [Hp(−) PG(+)]. The risk of developing gastric cancer increases progressively from Group A to Group D, with Groups C and D exhibiting higher incidence rates of gastric cancer.
A recent study in China evaluating a gastric cancer screening strategy that combines five serological markers—PG I, PG II, PGR, Hp antibody, and G-17—demonstrated that decreased levels of PG I and PGR are associated with a high risk of gastric cancer, while G-17 levels both below 0.5 pmol/L and above 4.7 pmol/L are also associated with a high risk. These findings suggest that a screening strategy incorporating multiple serological markers helps identify individuals at high risk for gastric cancer. Even in Western populations with lower Helicobacter pylori infection rates, pepsinogen-based serological screening offers significant advantages in improving the effectiveness of gastric cancer screening and reducing healthcare costs.
In the United States, implementing a serological pepsinogen (PG) screening strategy among individuals aged 50 years and older can reduce the risk of gastric cancer by approximately 26.4%, while an endoscopic screening strategy can reduce the risk by 21.2%. Furthermore, a combined screening strategy utilizing both serological testing and endoscopy offers a better cost-effectiveness ratio. [A]
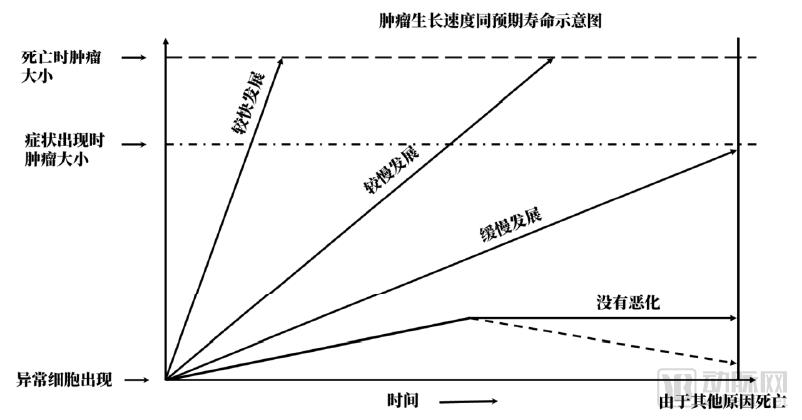
Image source: VCBeat
Rapidly growing cancers present symptoms and lead to death within a short period, making them difficult to detect early through cancer screening.
Slow-growing cancers can be detected through cancer screening before symptom onset, thereby extending potential survival time via subsequent treatment.
Early screening and early treatment of cancer can significantly improve the 5-year survival rate, as has been demonstrated by practices in Japan and South Korea.
According to the latest update of the “Japanese Guidelines for Gastric Cancer Screening” by Japan’s Ministry of Health, Labour and Welfare, the introduction of radiographic screening in cancer screening programs in Japan has reduced the 10-year probability of death from gastric cancer by 13.5%, while the introduction of endoscopic screening has reduced the 10-year probability of death from gastric cancer by 30.5%.
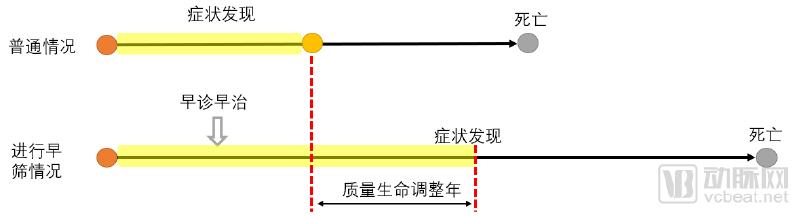
Image source: VCBeat
Using quality-adjusted life years (QALYs) as the reference metric, and incorporating China’s 2018 per capita GDP along with Japan’s experience in cancer screening, we find that the introduction of endoscopy into gastric cancer screening programs enables screened patients to gain approximately three additional QALYs compared to unscreened individuals. Based on China’s 2017 per capita GDP of RMB 59,200 and the national per capita disposable income of RMB 25,900, the economically adjusted benefit per individual patient from early screening amounts to an additional contribution of RMB 177,600 to GDP and an increase in disposable income of RMB 77,700.
The full version of the report includes the following content:
The above is an excerpt from this report,To download the full report, scan the QR code below:
