DRG Payment System Construction: International Experience in DRG Pricing
DRG-based payment refers to the classification of inpatients into several groups (i.e., DRG groups) based on factors such as disease severity, complexity of treatment methods, and consumption of medical resources, with payment standards established on a per-group basis.
The base price of DRGs, i.e., the payment standard, refers to the standard payment amount for each DRG group, which consists of two components: the DRG relative weight (RW) and the base rate (BR). The base price for the i-th DRG group is equal to the relative weight of the i-th DRG group multiplied by the base rate, namely Pi = RWi × BR. In actual pricing, factors such as annual changes in medical service costs, the consumer price index, and the inflation rate, as well as the specific circumstances of healthcare providers and patients within a given DRG group, must be taken into account. Based on the base price, additional payments may be added or unnecessary payments deducted.
Columnist: Dr. Liu Zhichen, a senior DRG expert and postdoctoral fellow in Public Administration at Fudan University

Professional Profile: Postdoctoral Fellow at the Postdoctoral Mobile Station in Public Administration, Fudan University, and the Postdoctoral Workstation of the Statistical Information Center, National Health and Family Planning Commission. A senior strategic expert in the big health sector. With nearly a decade of strategic consulting experience in internet healthcare and the broader big health industry, he previously served as Director of Strategic Consulting and R&D Business Development at a listed domestic IT solutions and services provider. In this role, he spearheaded the planning of numerous forward-looking innovative business models for the big health sector. He presciently predicted that reforms in China’s healthcare payment mechanisms, particularly the adoption of Diagnosis-Related Groups (DRG)-based payment, would become a key initiative in deepening healthcare reform during China’s 13th Five-Year Plan period. As the overall project lead, he participated in a pilot project for DRG-based medical insurance payment reform in a prefecture-level city in China. He assisted the city’s Medical Insurance Bureau in designing the top-level framework for the citywide DRG payment system reform and facilitated the implementation of supporting information technology systems.
I. Relative Weights
DRG Relative Weights Are a Key Component in Establishing DRG Rates and Payment Standards. The DRG relative weight is equal to the ratio of the average cost for patients in that DRG group to the average cost for all inpatients, reflecting the relative level of resource consumption for the DRG group. A relative weight greater than 1 indicates that the resource consumption for that DRG group is above the average level; conversely, it is at or below the average level.
The accuracy of DRG relative weights significantly impacts the effectiveness and fairness of the DRG payment system. If relative weight values are set too high, it becomes difficult to incentivize hospitals to improve efficiency through enhanced treatment methods. Conversely, if relative weight values are set too low, hospitals may compromise medical quality to reduce healthcare costs. Therefore, the accuracy of relative weights is also key to compensating hospitals under the DRG payment system, and many hospitals and research institutions in Europe and the United States are dedicated to studying methods for determining DRG relative weights.
The study by Barbara O. Wynn and Molly Scott (2008) suggests that different cost accounting methods have varying impacts on the calculation of DRG relative weights. This column has already provided a detailed introduction to various cost accounting methods in the section on DRG costs. Specifically, the relationship between different cost accounting methods and the calculation of DRG relative weights is illustrated in the figure below:
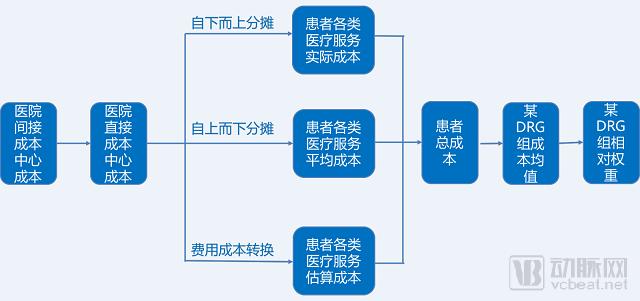
Figure 1. Relationship between Different Cost Accounting Methods and the Calculation of DRG Relative Weights
Typically, countries select a cost accounting system based on their actual medical cost data, the status of their accounting systems, and data quality, while also weighing the input-output ratio of different methods. Furthermore, calculating DRG relative weights requires defining the scope of DRG cost reimbursement; differences in this scope will inevitably lead to variations in DRG relative weights (for a detailed analysis, please refer to the introduction in the “DRG Cost” section of this column).
The calculation of DRG relative weights is a step-by-step process that requires the establishment of a long-term, dynamic system for their continuous updating and maintenance. In the initial phase of DRG implementation, incomplete information and the difficulty in cost forecasting mean that the accuracy and reliability of medical record data will directly impact the precision of DRG weights. As the Diagnosis-Related Group (DRG) prospective payment system is implemented, hospitals will strengthen the management of clinical practices and medical record coding, leading to progressively higher quality of medical record data. This will gradually mitigate significant intra-group variability, enabling DRG relative weights to more accurately reflect the consumption of medical resources.
From an international perspective, countries can only establish a unified system of relative weights. These relative cost weights are not fixed; rather, they are determined based on actual cost calculations and are typically adjusted annually. When implementing the Diagnosis-Related Group (DRG) system, Germany established an independent body, the Institute for the Hospital Remuneration System (InEK), to formulate the relative weights for each DRG group and to periodically revise these values. Due to variations in consumption levels and pricing models across different regions, as well as differences in clinical practices among hospitals, the formulation of relative weights must incorporate data from hospitals of varying tiers and locations. This process should be grounded in comprehensive national big data to ensure both applicability and fairness.
Typically, when calculating cost weights, hospitals with more accurate and comprehensive cost information are selected to calculate DRG relative weights, and continuous efforts are made to improve hospital data quality. For example, Germany has established a set of quality assessment standards for cost accounting, using predefined quality indicators to compare and screen the cost accounting systems of selected hospitals. Although the Netherlands requires all hospitals to submit their cost data, the calculation of relative weights is based solely on cost accounting data from 15–25 hospitals. France provides hospitals with additional compensation for the collection and calculation of cost data, with the amount directly linked to the quality of the hospital’s data.
II. Base Rate
Base rate refers to the monetary value of each relative weight point in pricing, which essentially represents the average cost per patient. It can be regularly updated and adjusted based on changes in factors such as annual healthcare service costs, consumer price index, and inflation rate in different regions.
International experience indicates that the base rate can be applied at three levels: national, regional, or hospital. If a uniform base rate is adopted at the national or regional level for funding allocation or payment purposes nationwide or within the region, the base rate is calculated by dividing the total DRG budget (or payment) amount at the national or regional level by the sum of the relative weights of all DRG groups in that country or region.
During the initial phase of the DRG pilot program, each hospital establishes its own base rate. The basic calculation steps involve dividing the hospital’s average budget (or payment) from the previous year or historical period by the total sum of relative weights for the same period; alternatively, it can be calculated by dividing the hospital’s average inpatient costs from the previous year or historical period by the average Case-mix Index (CMI). Here, CMI refers to the sum of relative weights for all cases divided by the total number of discharges, with the formula as follows:

The reform of the DRG payment system will significantly influence physician behavior, necessitating a gradual adaptation process. The calculation of disease-specific rates is an iterative process that becomes increasingly precise and convergent over time. Therefore, a transition period should be established, with annual recalculations of case-mix indices and payment rates. For instance, when the United States initially implemented DRG-based payments, there were substantial disparities in healthcare service capacity and volume across regions (the ratio of hospital length of stay between the East and West was nearly 2:1; cost variations per discharged case were associated with factors such as hospital size, geographic region, and urban versus rural location).
Therefore, a four-year transition period was implemented for the DRG payment system. During this transition, payment rates reflected each hospital’s updated cost levels from the base year (1982), with urban and rural hospital prices set separately at the local and national levels. In the first two years, payment rates were adjusted to align with the overall expenditure level of the previous payment system. After several years of transition, base rates across hospitals and regions were gradually harmonized, ultimately establishing a unified national base rate determined annually in accordance with laws and congressional mandates.
Therefore, the scope of uniform base rates has expanded from small to large, gradually achieving unification at the regional or national level. In the initial phase of implementation in Germany, base rates were established on a hospital-by-hospital basis, adopting a budget-neutral strategy for hospitals. Specifically, the DRG budget was calculated as the sum of the hospital’s historical prices and an allowable growth margin, serving as the total budget cap. This approach allowed hospitals to determine their own DRG group prices based on historical pricing, with gradual unification achieved first at the state level during the transition period, and subsequently at the national level.
Furthermore, three key issues must be addressed in the design of base rates: first, how much can be spent annually on inpatients; second, how much funding is actually distributed among hospitals; and third, the issue of dynamic adjustment. Only partial answers exist for the first two questions, because DRGs establish a base rate per discharge. If the case mix and the number of discharges change annually, total annual expenditures will fluctuate significantly, making it impossible to fix total spending or set a definitive overall budget. This has prompted an increasing number of countries to implement global budgets alongside DRG systems.
Dynamic adjustments must account for the rate of change in payment prices over time and internal structural modifications, considering how to incorporate prices and other influencing factors into the adjustment of relative weights and base rates. While maintaining relative consistency between prices and the efficient operating costs of hospitals, full consideration should be given to adjusting for numerous factors, including technological innovation, shifts in clinical diagnosis and treatment models, and changes in the prices of input factors invested by hospitals per discharged patient.
III. DRG Payment Standards and Pricing
DRG-PPS (Prospective Payment System Based on Diagnosis-Related Groups) is a method that, building upon DRG classification, categorizes inpatients with similar diagnoses, treatment approaches, and medical costs into distinct groups based on multiple factors such as patient age, disease diagnosis, comorbidities and complications, treatment modalities, disease severity, and treatment outcomes. It establishes scientifically calculated payment standards for each group and provides prospective reimbursement to healthcare institutions based on these standards.
With the DRG weight values established, the basic model for applying DRGs to health insurance fund management is as follows:

Figure 2. Calculation of DRG Payment Standards
The determination of DRG payment standards primarily involves two components: the DRG relative weight and the base rate. The DRG relative weight represents the relative point value among different DRG groups based on resource consumption; higher resource consumption results in a higher weight. Therefore, the relative weight itself reflects the relative relationship of resource consumption across different disease groups, and its formulation is a scientific process. The base rate refers to the monetary value per point, which is linked to the total health insurance fund and the total number of points generated during actual operations, and it is adjusted annually. The standard payment amount for each DRG group is calculated as the product of that group’s DRG relative weight and the base rate.
For medical institutions implementing a global budget based on Diagnosis-Related Groups (DRGs), the calculation method for the global budget is as follows:

where k is the number of DRG groups covered by the hospital's discharged cases.
(1) Adjustment Factors for Multiple Considerations and Cost Variations in DRG Pricing
Based on international experience, when countries establish diagnosis-related group (DRG)-based pricing, they typically use the payment standards derived from the aforementioned formulas as a baseline. In addition, they differentiate cost categories according to various medical services (such as nursing and laboratory testing) and make corresponding adjustments to the payment standards by comprehensively considering multiple factors (such as geographic region and hospital tier).
A series of adjustment factors are typically established. For instance, in the United States, base rates are adjusted according to factors such as hospital type, level of care, patient age, and disease severity to determine the final reimbursement rate. Consequently, hospitals serving a larger proportion of low-income patients or undertaking teaching responsibilities may receive additional subsidies calculated as a percentage of the DRG benchmark price. Furthermore, approximately 5% of the budget is generally reserved to compensate for outlier cases with exceptionally high costs, thereby mitigating the financial risk hospitals face when treating complex and challenging cases.
(2) Payment Pricing for Out-of-Network Cases
Payment systems based on Diagnosis-Related Groups (DRGs) as the fundamental unit of reimbursement set a cap on patient treatment costs. This incentivizes healthcare institutions to strengthen cost accounting and expense control management, encouraging them to proactively manage medical costs and thereby reduce overall societal healthcare expenditures. However, in clinical practice, a small subset of patients continues to exhibit poor disease control despite aggressive treatment, resulting in hospital stays and costs that are significantly higher than the average for their respective DRG group.
These patients pose significant financial risks to healthcare institutions. Without special regulatory policies, their inclusion could dampen healthcare institutions’ enthusiasm for participating in the DRG-PPS system and lead to the refusal of critically ill patients. Therefore, countries implementing DRG-PPS generally adopt special reimbursement methods for this group of patients (i.e., outliner cases).
Internationally, the definition of outlier cases is based on two criteria: hospitalization costs and length of stay (LOS), with standardized statistical segmentation methods used to define thresholds (i.e., so-called cut-off points). Cots et al. compared four statistical methods for identifying outlier cases and found that using the geometric mean plus or minus two standard deviations was the optimal approach for both high-cost outliers and LOS outliers. However, Magili argued that medical costs follow a log-normal distribution, with a geometric mean close to zero. Consequently, using the geometric mean plus or minus standard deviations to distinguish between outlier and non-outlier cases yields suboptimal results, particularly for low-cost cases.
He advocates the use of the quartile method, which sets the upper and lower bounds at the upper and lower quartiles, respectively, with values exceeding 1.5 times the interquartile range considered outliers. There are two approaches to defining outliers in hospital length of stay (LOS). Earlier practices in Germany, Spain, and the U.S. Medicare program defined outlier thresholds as the mean LOS plus or minus 2 or 3 standard deviations. In contrast, some countries, such as the United Kingdom, India, and Denmark, employ a non-parametric method that defines the threshold as the upper quartile plus 1.5 times the interquartile range. France combines both parametric and non-parametric methods to define outlier thresholds for hospital LOS.
In summary, the choice of any method should be based not only on the data characteristics of the available samples but also on the objectives that health policy makers aim to achieve through the implementation of Diagnosis-Related Groups (DRG).
High-cost outlier cases refer to patients whose hospitalization costs or length of stay exceed the average hospitalization cost or length of stay for patients within the same DRG group by a certain multiple. The criteria for defining outlier cases vary across countries. In Victoria, Australia, an outlier case is defined as one with a length of stay exceeding three times the average length of stay. In the United Kingdom, the threshold for outlier cases is calculated using the formula [Q75i + (Q75i - Q25i) * 1.5]. France, Spain, and Italy also have their own standards, which are more complex.
Overall, countries provide additional payment subsidies for the portion of costs exceeding the high-cost threshold, but these subsidies are insufficient to fully cover the costs (covering only 40%–60%). This approach both reduces the financial risk for healthcare institutions and prevents them from intentionally prolonging patients’ hospital stays to increase medical expenses in order to obtain additional subsidies.
The methodology for defining low-cost outlier cases abroad is consistent with that for high-cost outlier cases. In Germany, deductions are applied on a daily basis for patients transferred to other hospitals before the average length of stay is reached. If treatment for the same patient is jointly provided by two hospitals, it should be reimbursed as a single case. Exceptions are made for inter-institutional collaborations of particular significance and referrals involving affiliated entities (e.g., when surgery and intensive care are performed at a specialized cardiovascular hospital, followed by transfer to a hospital with lower specialization requirements for subsequent cardiovascular care).
In many countries, DRG-PPS payment standards are primarily cost-based. They categorize costs according to different medical services (such as nursing and laboratory testing) and adjust the payment rates by taking into account various factors, including geographic region and hospital tier.
Taking Estonia, an Eastern European country, as an example (John C. Langenbrunner, 2017), the process of using activity-based costing for cost accounting and DRG price calculation is as follows:
(1) Prepare basic data files, handle outliers, and perform data quality checks;
(2) Assess the structural changes in the average cost per case and changes in the medical service fee schedule;
(3) Calculate the adjusted average cost per case;
(4) Calculate the base rate, weight, and cost outlier threshold;
(5) Forecast changes and conduct a budget impact assessment;
(6) Prepare the draft specifications for fee-for-service payments and adjust the input files for the EHIF database (the EHIF database incorporates a central batch grouper for DRG-based allocation; Estonia implements a hybrid payment model consisting of 70% DRG-based payments and 30% fee-for-service payments).
Furthermore, it is particularly important to emphasize that, in order to safeguard the medical insurance fund and hospitals, extensive exclusion of outliers (also known as extreme values) falling beyond 3 and 2 standard deviations from the mean is performed when determining cost-based DRG prices. The specific methods and procedures are as follows:
(1) Calculate the standard deviation (STD) of the average cost and average price for each DRG group;
(2) Exclude cases with costs more than three standard deviations above or below the mean cost;
(3) Calculate the new mean cost and standard deviation for the remaining cases in the DRG group;
(4) Exclude cases with costs exceeding two standard deviations above or below the mean cost;
(5) Calculate the new average price for each DRG group based on the remaining cases in the DRG group;
(6) If fewer than 25 cases remain in the DRG group after dual processing, no new price will be calculated; only the base rate and the new weight will be used to define the price for that DRG group.
The specific calculation process is shown in Figure 3:
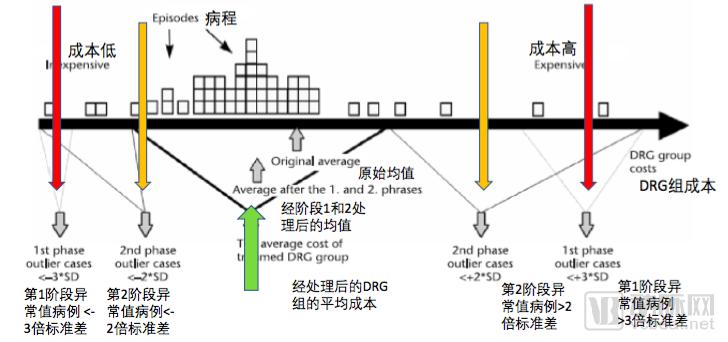
Figure 3. Cost-based DRG Payment Pricing Calculation Process in Estonia
DRGs are primarily applicable to short-term acute inpatients. In practice, countries need to define the pricing scope of DRGs in advance, taking into account their national characteristics. The vast majority of countries, including the United States, include acute inpatient care within the scope of DRGs. However, not all acute inpatient services are covered by DRGs. Some countries exclude high-cost services, such as radiotherapy, chemotherapy, renal dialysis, and expensive medications, from the DRG coverage.
In addition to acute inpatient services, countries such as Australia and Germany have incorporated day surgery into their coverage, while France has expanded its scope to include outpatient and day surgery. Furthermore, supplementary payments are provided based on the services delivered to patients, costs, or specific treatments. These supplements include daily add-ons (e.g., resuscitation, intensive care, continuous monitoring, prenatal care, and excessively long hospital stays) and fixed inpatient bundles (e.g., pediatric radiotherapy and cardiac defibrillators), but exclude pharmaceuticals and expensive implantable medical devices.
In terms of payment scope, Germany includes readmissions within 30 days after discharge under the same DRG case. It has achieved "two comprehensive coverages" in its application scope: the DRG system covers nearly all patients; regarding disease coverage, except for mental illnesses, the DRG system covers almost all types of diseases, with special payments limited to a few conditions such as hemodialysis.
DRG pricing and the determination of relative weights are two separate and independent processes. Pricing itself is a political process involving negotiation and strategic interaction among various stakeholders with differing interests. Therefore, when implementing DRG-based payment systems, countries typically establish an equitable negotiation and bargaining mechanism at the institutional level.
Taking Germany as an example, the German G-DRG system serves as the fundamental mechanism for allocating financial resources to healthcare institutions, channeling approximately 85% of such resources annually through this system. In 2013, statutory health insurance funds disbursed roughly €65 billion, making Germany one of the countries with the highest healthcare expenditures paid via DRG-based reimbursement globally. However, the allocation of healthcare costs in Germany is not determined empirically; rather, it is established through a highly sophisticated process involving empirical cost calculation and negotiation.
The Federal Joint Committee serves as a platform for negotiations between medical industry organizations, such as physician and hospital associations, and the National Association of Statutory Health Insurance Funds. Based on differing focal points, the negotiation mechanism is divided into two levels: the federal level and the regional level.
Negotiations at the federal level focus on establishing framework regulations, particularly those defining the uniform scope of basic health insurance coverage in Germany and measures to ensure the quality of medical services, with primary attention given to the healthcare benefits and coverage levels for insured individuals. In contrast, negotiations at the regional level place greater emphasis on financial matters, such as physician reimbursement, the volume of medical services for the upcoming year, and discounting mechanisms. Consequently, these arrangements vary by region, largely determined by the negotiating power and income levels of local physicians’ associations and other relevant stakeholders.
At the German state level, the primary parties to collective bargaining negotiations are the largest insurers and the largest healthcare providers, while smaller insurers or healthcare service providers engage in sub-negotiations following the same framework. State-level physicians’ associations are required to negotiate annual budgets with local sickness funds; otherwise, the budget outcomes may be vetoed by the statutory health insurance representatives at the federal level. If negotiations fail, the final budget is determined by the Federal Joint Committee.
Furthermore, Germany has established a specialized negotiation mechanism based on cost weight bargaining. The InEK (Institute for the Hospital Remuneration System) serves as the platform for negotiating DRG cost weights. Since the DRG base rate is standardized nationwide, variations primarily exist in the relative weights across states; therefore, regional negotiations are used to fine-tune hospital-specific weights. The InEK deliberately maintains a balanced structure between healthcare payers and providers: there are five seats for health insurers, five for healthcare institutions, and three neutral members (including the chairperson) who hold arbitral authority over proceedings. Additionally, there are five seats for patient representatives, though they do not have voting rights.
IV. Summary
Overall, a rational DRG pricing mechanism is crucial. Prices send important signals to all participants within the system and guide decision-making. The constructed payment system should allow prices to reflect costs; if set incorrectly, it will create perverse incentives. If prices are set too high, it leads to overprovision of services; if set too low, it results in underprovision, compromising the quality of care and even leading to the provision of inappropriate services. Meanwhile, it should also be recognized that the incentive mechanisms in pricing include the transfer of financial risk from payers to providers, with the key being to ensure that providers can bear the risks transferred to them.
Furthermore, DRG payment standards are not static indicators; they require timely dynamic adjustments based on cost factors, price indices, and the adoption of new technologies and therapies. Health insurance authorities should conduct forward-looking research on DRG group payments during the formulation of payment standards and incorporate diagnostic and treatment modalities into grouping criteria to prevent hospitals from reducing or even forgoing the use of new technologies in an effort to lower costs. Scientific and reasonable predictions of DRG group costs must be made, with continuous adjustment and improvement during implementation, to ensure the scientific rigor and rationality of DRG pricing.
Meanwhile, it is essential to establish a standardized DRG pricing negotiation mechanism and formulate a series of management rules for DRG payment in advance, providing guidance and standardized regulation through top-level design, legislation, organizational safeguards, and operational processes.
References
1. Barbara O. Wynn,Molly Scott. Evaluation of Alternative Methods to Establish DRG Relative Weights[R].WR 560-CMS,2008(4),Prepared for the Centres for Medicare and Medicaid Services
2. Zhou Yunyan, Jiang Qin, Zhang Zhenzhong. Analysis of the Calculation Methods for DRG Relative Weights in European and American Countries [J]. Chinese Health Economics, 2016(5): 94-96
3. Tan S. S., Rutten F. F. H., Vanineveld B. M., et al. Comparing methodologies for the cost estimation of hospital services[J]. European journal of health economics, 2009,10(4):39–45
4. Tan S. S.,Alexander G., Lisbeth S., et al. DRG systems in Europe: variations in cost accounting systems among 12 countries[J]. European journal of health economics, 2014,24 (6):1023–1028
5. Lang Jingjing, Yu Lihua, Zhou Hailong, Jiang Qin. Principles and Methods for Establishing C-DRG Relative Weights, Base Rates, and Service Prices[J]. Chinese Health Economics, 2017, 36(6): 18–19.
6. Julian Pettengill. Experience of U.S. Medicare in Implementing DRG-Based Hospital Payment [J]. Speech delivered at the China DRG Payment Conference, September 14, 2017
7. Zhao Yingxu, Jiang Qin. Experience of Medicare Inpatient Payment Reform in the United States and Its Implications for China [J]. Chinese Health Economics, 2013(6): 95-97
8. Xu Huaixiang. Evolution of Health Insurance Payment Methods in the United States and Its Implications for China’s Health Insurance Payment Reform[J]. Chinese Hospitals, 2012, 16(9): 69-72
9. Tan Guihong, Ren Xiaohui, Liu Zhijun, Li Ningxiu. Study on the Proportion of Diagnosis-Related Group Payment at Home and Abroad [J]. Chinese Health Service Management, 2013(9): 674-676
10. Chen Bo. Application Research of CHAID and Bayesian Network Models in DRG Grouping for Hepatobiliary and Pancreatic Diseases and Prediction of Outlier Cases [D]. Chengdu: Sichuan University, 2011
11. Magali P, Michele D, Leclercq D, et al. Analysis of cost outliers within APR-DRGs in a Belgian general hospital: two complementary approaches[J]. Health policy,2006(76):13-25
12. Stefan Felder. The variance of length of stay and the optimal DRG outlier payments[J]. International journal of health care finance and economics,2009,9(3):279-289
13. Feng Shuai, Shi Luwen. Foreign DRGs Pricing Process and Its Implications for Disease-Based Pricing in China [J]. China Pharmacy, 2012, 23(18): 1638-1641
14. Frank Haemisch. Experience and Lessons from the Implementation of G-DRG in Germany: What Are the Key Success Factors? [R]. China DRG Payment Conference, 2017(9)
15. John C. Langenbrunner. DRGs in Eastern Europe: Successes and Ongoing Challenges [R]. China DRG Payment Conference, 2017(9)
16. Jiang Qin, Zhang Zhenzhong, et al. A Discussion on Case-Mix DRGs and Clinical Quality Management. [J]. Chinese Health Quality Management, 2012(1): 2-6
17. Housseïni Holla. French National Agency for Hospital Information and Performance (ATIH): The Impact of France’s DRG Implementation on China [R]. China DRG Payment Conference, 2017(9)
18. Huang Sangui. The Development History, Current Challenges, and Future Prospects of the Taiwan DRGs Policy [R]. Speech at the First National Diagnosis-Related Groups (DRG) Forum, 2016(12)
19. Chang Feng, Ji Meiyan, Lu Yun. Germany’s G-DRG Health Insurance Payment System and Its Implications for China [J]. Chinese Health Economics, 2016(6): 92-96
Copyright Statement:
Most of the views expressed in this article are based on Dr. Liu Zhichen’s personal postdoctoral research findings. The cited articles and viewpoints reflect those of their respective authors, as obtained from publicly available sources. Unauthorized reproduction, excerpting, copying, mirroring, or any other form of use is strictly prohibited.