DRG Column Series VI: How the U.S., Australia, and the Netherlands Tackle Upcoding and Declining Healthcare Quality (DRG Oversight Edition)
Every payment method carries certain negative consequences. To proactively mitigate adverse effects potentially associated with DRG-based payment, such as upcoding and fragmented hospitalizations, countries have implemented a series of regulatory measures. These include oversight of data quality, cost-control mechanisms, monitoring of medical quality and efficiency, and outcome evaluation. Leveraging robust health information systems, various nations have established relatively comprehensive sets of regulatory indicators to enable real-time monitoring of DRG implementation. Furthermore, they employ incentive and penalty mechanisms—rewarding high-performing healthcare institutions while penalizing underperformers—to enhance the overall effectiveness of regulation.
Columnist: Dr. Liu Zhichen, Senior DRG Expert and Postdoctoral Fellow in Public Administration at Fudan University

Professional Profile: Postdoctoral Fellow at the Postdoctoral Mobile Station in Public Administration, Fudan University, and at the Postdoctoral Workstation of the Statistical Information Center, National Health and Family Planning Commission. Senior strategic expert in the big health sector. With nearly a decade of experience in strategic consulting for internet healthcare and the broader health industry, previously served as Director of Strategic Consulting and Scientific Research Business Development at a listed domestic IT solutions and services provider. Spearheaded the planning of numerous forward-looking innovative business models for the big health sector. Accurately predicted that reforms in China’s medical payment systems, particularly the implementation of Diagnosis-Related Groups (DRG)-based payment, would become a key initiative in deepening healthcare reform during China’s 13th Five-Year Plan period. Served as the overall project lead in a pilot program for DRG-based medical insurance payment reform at the prefecture-level city in China. Assisted the municipal Medical Insurance Bureau in designing the top-level framework for citywide DRG payment system reform and facilitated the deployment of supporting information technology systems.
I. Negative Impacts of DRG-Based Payment
The primary purpose and role of DRG-based payment is to guide hospitals and medical personnel in the rational utilization of healthcare resources, curb unreasonable consumption in medical services, and encourage hospitals to tap into their potential by reducing average length of stay and hospitalization costs, thereby improving quality, benefits, and efficiency. It also aims to reduce inducement-driven medical expenditures and effectively lower the average medical costs across China. This major reform has demonstrated significant effectiveness in clinical disease payment and has become the predominant payment method for healthcare cost management in more than 40 countries worldwide.
However, in the process of implementing DRG, various countries have also experienced a series of negative impacts triggered by DRG-based payment, which can be specifically categorized into the following major aspects:
Upcoding (also known as overcoding, code creep, or up-leveling) refers to the erroneous coding and classification of patient data to increase reimbursement for healthcare services. This practice leads to distortion of health statistics and abuse of the financing system. Following the implementation of Diagnosis-Related Group (DRG) prospective payment, hospitals may be inclined to engage in upcoding in response to imposed budget constraints.
"Due to the 'reasonable variability and uncertainty inherent in medical issues, subtle diagnostic nuances and slight imprecisions in wording can have significant consequences for DRG reimbursement.' This 'medical variability and uncertainty' creates information asymmetry between hospitals (healthcare professionals) and insurance companies that reimburse medical costs. Therefore, in this sense, upcoding is theoretically inevitable and will occur regardless of the measures taken."
In the first decade of DRG implementation in the United States, each revision to the DRG system was followed by a new wave of upcoding. Silverman and Skinner also demonstrated the widespread nature of upcoding risk, finding that 25% of non-profit hospitals and 32% of for-profit hospitals exhibited such risks. Many countries are exploring measures to curb this phenomenon, such as establishing incentive systems to encourage accurate coding by hospitals. German studies have found that medical record documentation alone is insufficient to provide adequate coding information. However, other research indicates that coding errors in many hospitals are primarily concentrated in “under-coding,” leading to inadequate reimbursement for hospital costs; hospitals are often more concerned about this issue than about “over-coding.” Therefore, methods to enhance coding accuracy, such as continuous education and training for coders, need to be significantly strengthened.
Since the DRG-PPS payment mechanism lacks positive incentives for healthcare quality, some medical institutions and healthcare professionals may compromise on quality in an effort to control costs and reduce the average length of stay.
However, a review of the literature and practices in the United States and European countries by Reinhard Busse et al. (2011) revealed that the impact of DRG implementation on quality varied in two opposing ways: on the one hand, DRG-based payment intensified competition among providers, thereby incentivizing healthcare institutions to improve quality to attract more patients; on the other hand, healthcare institutions might indeed reduce the quality of services provided to patients as a means of controlling costs.
For instance, regarding the issue of premature discharge of inpatients: The Research Center for Payment Systems in Germany has established clear regulations on readmissions within one month for patients under the same Diagnosis-Related Group (DRG), but has not given sufficient consideration to arrangements for early discharge. Consequently, some hospitals arrange for patients to be discharged during the initial phase of recovery. Although this practice does not have severe adverse effects on patients’ health, it significantly impairs their quality of life and increases the difficulty of rehabilitation. Langenbrunner JL. (2009) also found that DRGs lead providers to reduce the average length of stay, resulting in earlier patient discharges and greater clinical instability among patients.
Furthermore, some hospitals, facing reduced revenues, have been forced to discontinue certain high-cost clinical services that are nonetheless socially necessary, leading to the underutilization of medical resources. Essential high-cost specialty drugs and advanced diagnostic and therapeutic procedures are not being employed when indicated, resulting in missed optimal treatment windows, compromised therapeutic outcomes, and an increase in doctor-patient disputes.
Therefore, when implementing DRG-based payment systems, countries introduce healthcare quality oversight measures to mitigate the risk of potential declines in medical quality that may arise from DRG reimbursement.
To reduce patients' actual length of stay, hospitals have unbundled DRG-covered medical services and shifted them to other departments (outpatient clinics), other hospitals, or post-acute care facilities. Some hospitals even attempt to increase admission rates by arranging for patients to be discharged and then readmitted, thereby fragmenting hospitalization episodes to secure higher reimbursement.
For instance, the German DRG payment model was designed exclusively for inpatients, with no consideration given to outpatients. This directly led hospitals to shift a large number of patients who should have been hospitalized to outpatient settings, resulting in a sharp rise in outpatient costs.
Additionally, numerous studies have shown that "rapid and safe" hospital discharge can also increase the additional burden of rapidly growing demand for "home hospital beds."
Since the specific implementation method of the DRG payment scheme is based on the DRG category to which each patient belongs, rather than on their actual costs, a hospital makes a profit if a patient’s actual hospitalization costs are lower than the payment standard for that patient’s DRG category, and incurs a loss otherwise. This mechanism inherently incentivizes hospitals to refuse critically ill patients and favor those with mild conditions.
Meanwhile, this payment model does not differentiate between cases with high or low dependency, leading hospitals to avoid accepting patients with high dependency, thereby threatening the equity of health services.
The DRG payment system inherently discourages hospitals from adopting resource-intensive new diagnostic methods, therapeutic approaches, and service offerings, which, to a certain extent, hinders the innovative development of clinical medicine and impedes technological progress.
The DRG system focuses solely on reimbursing disease treatment, while neglecting disease prevention and health promotion. Furthermore, there are certain difficulties in applying the DRG system to psychiatric patients and chronic diseases, even though the population seeking services in these areas is growing increasingly large.
II. Construction of the DRG Regulatory System
In view of the aforementioned adverse effects that may arise from the DRG payment system, countries around the world must simultaneously establish a relatively comprehensive DRG regulatory framework when implementing reforms to the DRG payment system, so as to mitigate potential negative impacts to the greatest extent possible. Specific measures include the following key areas:
Lu Hui et al. (2008), through a review of international literature, found that the likelihood and influencing factors of high coding risk exhibit distinct characteristics across different markets, control mechanisms, and case-mix systems. These are illustrated in the figure below:
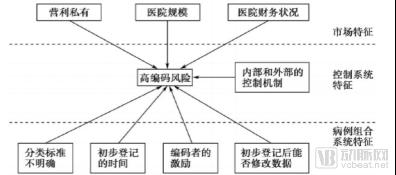
Figure 1. Factors Influencing the Risk of Upcoding in the DRG System
(1) Relationship between Market Characteristics and High Coding Risk, and Regulatory Measures
Typically, a higher risk of upcoding is more likely to occur in regions with a high market share of for-profit hospitals, indicating a strong correlation between upcoding risk and for-profit ownership structures. Furthermore, even non-profit hospitals exhibit elevated upcoding risks in areas where for-profit hospitals hold a substantial market share. Cutler and Horwitz argue that “a high market share of for-profit hospitals will drive non-profit hospitals to adopt similar profit-seeking strategies.”
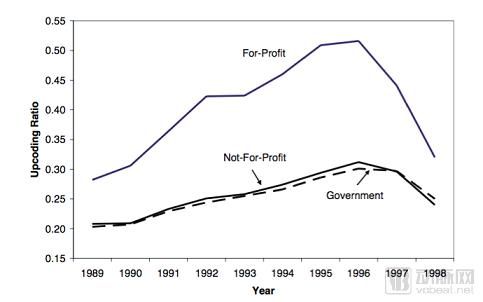
Figure 2. Comparison of Upcoding in For-Profit and Nonprofit Hospitals in the United States (1989–1998)
Furthermore, hospitals with stronger financial positions are more likely to face risks of upcoding. This risk is also correlated with hospital size; Dafny found that larger hospitals can provide advanced training to coding staff to optimize revenue.
Therefore, during the initial phase of DRG-based payment, excluding for-profit hospitals and prioritizing the supervision of large-scale hospitals with strong financial conditions can effectively control the generation and incidence rate of high-coding risks.
(2) The Relationship Between Characteristics of the Diagnosis-Related Group (DRG) System and High-Coding Risk, Along with Regulatory Measures
According to Lu Hui et al. (2008), a review of international literature reveals that differences among various DRG systems in the following aspects may stimulate the risk of upcoding:
Unclear Classification Criteria
Classification standards involve ambiguous categorizations. The classification criteria of case-mix systems determine the assignment of patients to Diagnosis-Related Groups (DRGs), and hospital reimbursements are also based on the outcomes of these classification criteria. Simborg argues that the widespread presence of upcoding risk stems from the recognition of medical diversity and uncertainty in many diagnoses. If classification criteria lack medical significance and do not align with clinical practice, they are considered ambiguous, thereby leading to high upcoding risks or fraud. A key reason for the introduction of DRGs in the United States was that the classification scheme could provide clear medical justification. Although healthcare professionals continue to strive for DRG optimization, DRG systems in both the United States and Australia still contain classification criteria lacking clinical significance. For example, the "chest pain" DRG is defined as "severe pain related to cardiac conditions." This DRG lacks clinical meaning. As a result, unreasonable reimbursement costs attributable to this issue reached $173.7 million in 2004, indicating that 19.2% of patients were assigned to this DRG group.
Upcoding the principal and secondary diagnoses to secure higher reimbursement constitutes another form of high-coding risk. For instance, a study by Psaty et al. found that coders frequently modified the assignments of principal and secondary diagnoses for patients with heart failure, resulting in an average payment increase of $3,445 (in 1997 dollars). This suggests that secondary diagnoses have become a standard avenue for fraudulent profit-making. Serdén et al. observed that “the introduction of DRG-based prospective payment systems has led to an increase in the coding of secondary diagnoses.” They argued that hospitals operating under DRG-based prospective payment systems coded more secondary diagnoses than those without such systems. Fan Guigao and Xia Zongming (2004) reached similar conclusions based on a review of Swedish literature, noting a sharp rise in the number of secondary diagnoses recorded by hospitals after Sweden implemented the DRG prospective payment system.
To mitigate the risks of fraud or upcoding, the U.S. case-mix system has adopted a structured DRG classification framework. This framework fixes the relationships between all DRG groups and the principal diagnosis, other diagnoses (complications and comorbidities), as well as their corresponding average length of stay and relative weights (see Figure 2-26), with annual updates.
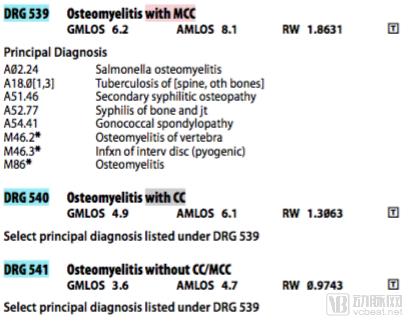
Figure 3. U.S. DRG Groups, Weights, and Average Length of Stay Lookup Table (2015)
The design of the U.S. system accounts for the most severe complications and permits hospitals to report secondary diagnoses, thereby incentivizing them to maximize upcoding by extending the list of secondary and additional diagnoses as much as possible to secure higher reimbursement.
Compared with the United States, Australia’s DRG system incorporates the PCCL model in its design to calculate the cumulative effect of CCs/MCCs for a patient based on the average level of all complications, thereby assigning patients to DRG groups. This approach offers a fairer method for measuring the impact of secondary and additional diagnoses on hospital resource utilization. In 2015, the new version AR-DRG 8.0 further introduced the ECC model, which, by taking into account clinical realities and the influence of diagnoses and their quantity on costs, adopted a precise cost-calculation mode. This enabled a more accurate and reasonable assessment of the cumulative effects of CCs/MCCs and their impact on resource consumption than the PCCL model, thus achieving more precise grouping. Consequently, the Australian DRG system, built upon precise model-based calculations, provides less incentive for upcoding risk than the U.S. system.
Timestamp of Original Registration During Service Delivery
A comparison of the timing for initial patient classification across the DRG systems in Australia, the United States, and the Netherlands reveals substantial evidence that the risk of upcoding is higher after the completion of diagnostic and therapeutic procedures than at their initiation. Since patients in the United States and Australia are assigned to DRGs only upon discharge, these systems carry a greater risk of upcoding compared to the Dutch system. Therefore, when designing DRG-based payment systems, careful consideration should be given to the timing of DRG assignment to minimize incentives for upcoding.
Incentives for Medical Coders
If coders’ compensation is not tied to the final patient classification outcomes, there is no potential conflict of interest, and the incentive for upcoding is minimal. In the Netherlands’ case-mix system, coders are healthcare professionals themselves, and their remuneration is based on DRG classifications. In contrast, in the DRG systems of the United States and Australia, coders are employed by hospitals, and their income is unrelated to DRG grouping; therefore, the associated risk is relatively lower than in the Netherlands.
Likelihood of Changes to Original Registration Codes
The possibility of altering DRG codes after initial registration provides coders with opportunities for upcoding. In the Netherlands’ case-mix system, healthcare professionals can make multiple coding adjustments in a timely manner. In contrast, original coding cannot be modified in the United States or Australia. Therefore, regarding this criterion, the risk of upcoding is higher in the Netherlands.
(3) Relationship Between Control System Characteristics and High Coding Risk, and Regulatory Measures
In response to the widespread risk of upcoding, different countries have established distinct control systems. For instance, the case-mix systems in the United States and Australia rely primarily on external controls and/or retrospective reviews, whereas the Dutch system is mainly based on internal controls and requires the submission of a board declaration. Experience from some European countries involves intensifying random inspections through external audits or regulatory oversight, while simultaneously implementing measures to circumvent or reduce hospitals’ capacity for non-compliant practices and increasing penalties for such violations.
Table 1 Comparison of DRG Upcoding Control Systems in the United States, Australia, and the Netherlands
Country | Regulatory Measures | Specific Content | Remarks |
United States | Hospital Payment Monitoring Program | This program monitors the appropriateness of payments for emergency inpatient services over both long-term and short-term periods. Fiscal intermediaries process the payments, while Quality Improvement Organizations (QIOs) are responsible for ensuring coding accuracy, coverage, and medical necessity. | Both programs evaluate “whether medical services should be reimbursed, medical necessity, coding accuracy, and documentation completeness” by reviewing patient cases.
|
Comprehensive Error Rate Test Protocol | Monitor the allowable payment amounts by fiscal intermediaries for inpatient and outpatient services under non-prepayment systems | ||
Error Rate of the Service Fee Payment System | Error rate is a composite metric, established on the basis of the error rates of the first two schemes. | In 2004, the synthesis error rate was approximately 5.2%, corresponding to improper overpayments and underpayments totaling about $12.1 billion, including $11.2 billion in overpayments and $0.9 billion in underpayments. The overpayment and underpayment rate for the prospective payment system for emergency inpatients was approximately 5.2% ($4.8 billion). | |
Mandatory Use of Bundled Software with Embedded Checks | Partially serves to prevent incorrect DRG grouping of patients. | ||
Code of Ethics | Coding Professional Standards and Implementation Principles Developed by the American Health Information Management Association (AHIMA) | Professional organizations or institutions that adopt a code of conduct will require adherence to it, with violations subject to peer review. | |
Professional Standards Education for Coders | AHIMA issues credentials in health information management, coding, and privacy and security of health services; to earn these credentials, candidates must complete comprehensive education, meet degree requirements, and pass national certification examinations. | ||
Official Statement from Medical Personnel | Medical personnel must commit that "the documentation of primary and secondary diagnoses, as well as the primary procedure, must bear their signature in the medical record." | If medical personnel engage in upcoding, they will face severe penalties, including imprisonment. | |
Australia | Coding Benchmark Review | Implemented by the health and aged care departments of Australian states. This measure involves peer review of clinical coding, enabling hospitals to proactively establish comparable benchmarks in coding practices with other institutions. Targeted audits can be conducted instead of comprehensive year-long DRG audits; for example, auditing specific DRG groups characterized by ambiguous diagnoses, such as chest pain, or examining the proportion of patients with high complication/comorbidity (CC) levels across hospitals. | Implementation of the Australian Coding Standards review by 7.6% of coders. 6.6% of coders believed that external audits of the Australian Coding Standards conducted in hospitals ensured data quality.
|
“Performance Indicators for Coding Quality” (PICQ) to Ensure Data Integrity | Coded data are compared with predefined metrics to assess coding quality. The metrics provide coding quality measurements in a standardized format, facilitating easier comparison of results. | 14% of coders indicated that they use PICQ. 9% of coders believed that external analysis via PICQ can ensure data quality. | |
Sanitation Audit | State health departments use audits as a measure to ensure data integrity. For example, the Department of Human Development in local governments in Victoria conducts regular coding audits on hospitals. | If there is a disagreement between the expert and the hospital regarding coding, the patient’s case will be recoded. The entire process is anonymous and is referred to as the “gold standard.” Hospitals found guilty of upcoding will be penalized through reductions in DRG case-based payments or suspension of payments. | |
Built-in Error Grouping Checker in the DRG Grouper | Similar to the U.S. system, certain built-in checks are incorporated into the DRG grouper software to prevent incorrect patient classification. | ||
Code of Ethics | Enforced by the National Health Information Management Association and the Australian Health Information Management Committee, it defines standards for the professional performance of coders and other members. | Violation of the code will be considered unethical | |
Professional Standards for Coders' Educational Background | Coders are required to have received professional education or training to be qualified for this position. | Most coders hold a bachelor’s degree in health information management or medical record management. Some of them have obtained graduate degrees in health information management. Only 10% of coders have received only on-the-job training, without any further formal education in coding. | |
Netherlands | Built-in validation modules in the DBC (Dutch DRG system) for internal control to ensure accurate verification and reconciliation, thereby mitigating the risk of upcoding. | Medical personnel register and approve the entire DBC opening process. If a patient’s treatment has concluded, medical personnel must approve the DBC before the health insurance company can review and process payment. After approval, the validation module is used to monitor for upcoding or incorrect coding. | Based on historical hospital services and in comparison with treatments recorded by physicians, patient treatments are confirmed. If the treatment generated by the verification module is inconsistent with the physician’s treatment, the system will issue a warning, as sufficient data exists to analyze possible or impossible combinations for forming Diagnosis-Related Groups (DRGs) and treatments. These possible and impossible combinations have been developed and validated by medical personnel from scientific organizations. Whenever there is a discrepancy between DRG registration and the verification model, the DRG cannot be billed; therefore, the DRG code or the underlying registration of hospital services must be adjusted. |
Hospital Board Statement | The Board of Directors must declare whether the hospital has acted in accordance with all prescribed procedures. An independent auditor must sign this declaration. The hospital’s Board of Directors commits to assuming ultimate responsibility for DBC registration and billing. | If violations occur, board members will be subject to penalties. This can help mitigate the risk of upcoding.
|
As described in the previous section, as a payment system, Diagnosis-Related Groups (DRGs) may incentivize healthcare institutions to prioritize cost containment at the expense of medical quality—for example, by discharging inpatients prematurely or reducing the use of expensive medications and consumables—thereby introducing greater instability into patient recovery. To effectively mitigate quality-related risks, countries implementing DRG payment reforms must establish complementary measures for quality monitoring, evaluation, and control.
(1) Strengthening the Standardized Management of Patient Treatment Processes: The Introduction of Clinical Pathways
Whether the implementation of Diagnosis-Related Groups (DRGs) can effectively safeguard patients' rights and interests hinges on the development of scientific and relatively objective clinical diagnosis and treatment guidelines. It is essential to establish clinical standards for each DRG group, including diagnostic criteria, admission and discharge criteria, and treatment protocols. This facilitates comprehensive process management of medical services, ensures the quality of care, prevents healthcare providers from reducing necessary services, and ultimately protects patients' rights and interests.
To this end, countries such as the United States and Australia have introduced clinical pathway management to strengthen the standardized management of patient treatment processes after implementing DRG-PPS.
Clinical Pathway (CP) refers to a procedural and standardized diagnosis and treatment plan, developed based on evidence-based medicine with the goals of achieving expected therapeutic outcomes and controlling costs. It features strict work sequences and precise timing requirements, aiming to standardize medical service delivery, reduce delays in recovery and resource waste, and ensure that patients receive optimal medical care.
Clinical pathways place greater emphasis on process control, enabling hospitals to standardize physicians’ diagnostic and treatment behaviors by focusing on the clinical care process, thereby improving healthcare quality. As such, they serve as a crucial tool for hospitals to achieve refined management. Consequently, integrating clinical pathways with Diagnosis-Related Groups (DRGs) can effectively address the blind spots in quality oversight associated with DRG-based payment systems. Clinical pathways encourage multi-departmental, interdisciplinary support and interaction, more effectively enhancing management and quality standards. They facilitate process standardization and timely correction of arbitrary and non-compliant practices by clinicians. By transforming uncertain medical practices into relatively predictable ones with fixed costs, clinical pathways better fulfill the dual roles of cost containment and quality monitoring.
In the United States, the emergence and development of clinical pathways have spanned more than two decades. Due to their proven effectiveness in controlling healthcare costs and improving the quality of care, clinical pathways have gained broader adoption over the past five years and are now applied across health service institutions at all levels and of all types. The implementation of clinical pathways reflects a hospital’s level of refined medical management and informatization, serving as an effective tool for DRG (Diagnosis-Related Group) management.
However, due to the varying granularity of internal grouping within DRG systems across different countries, and the lack of clear clinical classification for certain conditions (such as chest pain), not all disease groups are suitable for clinical pathway management; a small number of more complex diseases are not appropriate for such management.
(2) Real-time monitoring of medical quality using information systems and regulatory indicators
Experience from various countries indicates that the DRG system establishes a database foundation for regulatory authorities, enabling real-time monitoring of quality through information systems, which has improved service quality to some extent. Based on this database infrastructure, many countries often employ specific regulatory indicators alongside DRG-based payment or financing mechanisms to ensure healthcare quality.
Germany mandates that hospitals failing to submit quality data will face payment reductions. In 2017, it further enacted new regulations stipulating “additional payments for high-quality care and payment reductions for low-quality care” (Frank Heimig, 2017). In the United Kingdom, hospitals that fail to meet quality standards are subject to a 1.5% deduction from their total reimbursement. The United States has also selectively established corresponding metrics for conditions such as acute myocardial infarction, heart failure, pneumonia, pregnancy and related conditions, surgical care, pediatric asthma care, venous thromboembolism, stroke, and emergency hospitalizations.
To more comprehensively mitigate the various adverse effects associated with DRG-based payment, some regions have established more comprehensive regulatory systems. Taking Taiwan as an example, the details are shown in Table 2:
Table 2 Comprehensive Regulatory Indicator System for DRG in Taiwan
Indicator Category | Indicator Description | Refined Metrics |
Medical Efficiency Monitoring | Trends in Length of Hospital Stay | Average Length of Stay per Hospitalization |
Discrepancy Between Medical Payment Points and Actual Medical Service Points | Average Actual Medical Points per Case Average DRG Points per Claim Ratio of DRG Points to Actual Points | |
Cost Transfer Monitoring | Reducing Essential Services and Lowering Healthcare Quality | Proportion of DRG Cases with Complications |
Transfer of Inpatient Costs to Outpatient Care | Average Number of Outpatient Laboratory and Diagnostic Tests Within 1 Week Prior to Hospitalization Average Outpatient Medical Points Within 1 Week After Discharge | |
Patient Transfer Monitoring | Refusing to admit critically ill or loss-making patients | |
Split Hospitalizations or Inappropriate Transfers | DRG Inpatient Case Transfer-Out Rate | |
Outcome Measurement Monitoring | Trends in the Number of Cases with Out-of-Range Values | |
Trends in Patient Severity Changes | CMI Value Changes | |
Trends in Readmission Rates and Re-ED Visit Rates | 3-Day Emergency Department Revisit Rate 14-Day Readmission Rate | |
Medical Quality Monitoring | Acute Myocardial Infarction Mortality Rate |
In summary, the regulatory review of Taiwan’s DRG system primarily focuses on several key areas: the necessity of admission or primary surgical procedures (interventions), the appropriateness of diagnoses and interventions, the accuracy of diagnosis and procedure coding, the shifting of costs related to inpatient care, the appropriateness of medical expenses for outlier cases exceeding the upper threshold limits, the stability of patients’ condition at discharge, and the adequacy of medical quality. These measures aim to better mitigate the potential adverse effects associated with DRG-based payment systems, offering valuable insights for reference.
References:
1. Zhao Yingxu, Jiang Qin. Experience of Medicare Inpatient Payment Reform in the United States and Its Implications for China [J]. Chinese Health Economics, 2013(6): 95-97
2. Lu Hui, Chen Jiaying. A Comparative Study on the Risk of Upcoding in Case-Mix Systems in the United States, Australia, and the Netherlands [J]. Foreign Medical Sciences (Health Economics Fascicle), 2008, 25(3): 120-126.
3. Reinhard Busse,Alexander Geissler,Wilm Quentin,Miriam Wiley. Diagnosis-Related Groups in Europe : Moving towards transparency, efficiency and quality in hospitals[M]. New York,2011: 120-128
4. Bartkowski R. Length of hospital stay due to DRG reimbursement [J]. Ther Umsch,2012,69( 1) : 15-21.
5. Langenbrunner JL.Designingand Implementing Health Care Provider Payment Systems: How to Manulas [B] . The World Bank,2009
6. Lu Yong. Operational Mechanism and Effectiveness Evaluation of the Australian Diagnosis-Related Groups Prospective Payment System[J]. Chinese Health Resources, 2011(9):343-345
7. Chuang KH,Covinsky KE,Sands LP,et al. Diagnosis-Related Group-Adjusted Hospital Costs Are Higher in Older Medical Pa- tients with Lower Functional Status [J]. Journal of the American Geriatrics Society,2003,51: 1729-1734
8. Wang Liuming, Lang Wen, Tao Hongbing. Advantages and Disadvantages of the German Diagnosis-Related Groups Payment System and Its Implications[J]. Medicine and Society, 2013(11):44-47
9. Elaine Silverman, Jonathan Skinner. Medicare upcoding and hospital ownership[J]. Jounal of Health Economics 2004(23):369-389
10. Fan Guigao, Xia Zongming. The Impact of Sweden’s DRG Prospective Payment System on Secondary Diagnoses [J]. Foreign Medical Sciences (Health Economics Fascicle), 2004, 21(1): 42-43
11. Optum. DRG Expert(ICD-10 Version): The Complete Official Draft MS-DRG Using the ICD-10 Code Set[D].2015(4): 161
12. Fan Wenyi, Wu Xinxia, Xu Xuedong. Impact of DRGs-PPS Implementation on Clinical Pathway Work [J]. Hospital Management Forum, 2012, 29(4): 24-26
13. Jiang Qin, Zhang Zhenzhong, Zhao Yingxu, et al. Relationship between Clinical Pathway Management and Disease-Based Payment[J]. Chinese Health Quality Management, 2012, 19(1): 11-13
14. Jiang Qin, Zhang Zhenzhong, Zhao Yingxu, et al. Discussion on Case-Mix DRGs and Clinical Quality Management [J]. Chinese Health Quality Management, 2012, 19(1): 2-6.
15. Frank Heimig. Experience and Lessons from Germany’s Implementation of G-DRG: What Are the Key Success Factors? [R]. Speech delivered at the China DRG Payment and Reimbursement Conference, September 14, 2017
Copyright Notice:
Most of the viewpoints presented in this article are derived from Dr. Liu Zhichen’s personal postdoctoral research project. The cited articles and viewpoints reflect those of their respective authors, obtained from publicly available sources. Unauthorized reproduction, excerpting, copying, mirroring, or any other form of use is strictly prohibited.