Vaccines May Lose Effectiveness Faster Than Expected—And Few Are Paying Attention
Like millions of other Americans, Stanley Plotkin and his wife received their flu shots in early October last year, at the start of the Northern Hemisphere’s influenza season. As an emeritus professor at the University of Pennsylvania, Plotkin is well aware of the importance of this injection. He is one of the world’s most renowned vaccinologists, having participated in the development of various vaccines, including the rubella vaccine. He is even a co-author of the standard medical textbook Vaccinology.
This January, just three months later, the couple received another flu vaccination.
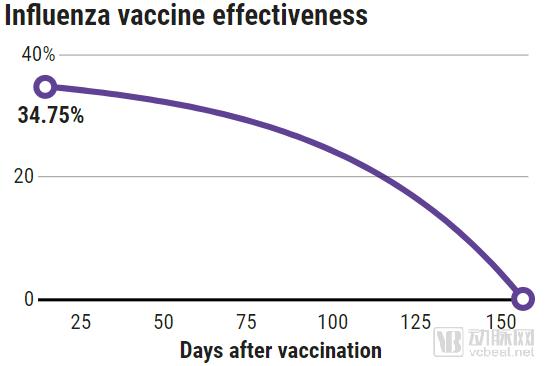
Figure: The effectiveness of influenza vaccine against H3N2 influenza wanes over time since vaccination, disappearing completely by day 150 (based on U.S. data from 2011–2015)
Source: (GRAPHIC) N. DESAI/SCIENCE; (DATA) J. FERDINANDS ET AL., CLINICAL INFECTIOUS DISEASES, VOL. 64, 544, 2017
Most people would not make such a choice to get revaccinated within a short period. The Advisory Committee on Immunization Practices (ACIP) in the United States has not recommended this either. However, growing evidence suggests that the protective immune response conferred by influenza vaccines wanes within weeks. This evidence prompted Plotkin to return to the clinic for another vaccination. “At my age, this amount of time and money is negligible compared to the risk of catching a cold,” said 86-year-old Plotkin. “For us, influenza is far more serious than just a runny nose.”
This phenomenon is not limited to influenza vaccines. Recent studies have shown that vaccines for mumps, pertussis, meningococcal disease, and yellow fever also wane in efficacy more rapidly than indicated by official vaccination schedules. Over the past few decades, vaccines have served as a critical public health tool, helping us combat diseases; however, our understanding of their durability remains limited.
This may sound somewhat counterintuitive, but it is indeed the case: vaccines were approved and brought to market before the precise duration of protection was clearly established, leading to the issue of waning vaccine efficacy being overlooked. Because widely used vaccines have largely interrupted the transmission of the pathogens they target, “breakthrough” infections have become increasingly rare. Even when viruses or bacteria continue to circulate, vaccinated individuals often acquire naturally boosted immunity. Waning vaccine-induced immunity is not an all-or-nothing phenomenon; breakthrough infections that occur during this period of declining protection tend to result in milder disease symptoms.
Researchers are making continuous efforts to understand why some vaccines provide protection for only a few weeks, while others confer lifelong immunity. “We simply do not know what induces durable immunity,” said Plotkin, who has been studying vaccines since 1957. “For many years, we developed vaccines with little understanding of their immunological properties. Everything hinges on immune memory, yet we have not systematically studied it.”
Stanford University immunologist Bali Pulendran has reached the same conclusion regarding vaccine durability. “I have been saying, ‘We don’t yet understand it; we don’t yet understand it.’ Vaccine durability is one of the key issues in vaccinology.” With respect to vaccine durability, the two foundational vaccines that prevent diphtheria and tetanus appear to last longer than previously expected.
Now, clues are emerging from those highly successful vaccines that can drive the immune system to mount effective responses for decades. For instance, the human papillomavirus (HPV) vaccine has proven to be effective in the long term since its debut approximately ten years ago. New insights into durability are also prompting researchers to scrutinize more closely the vaccination recommendations put forth by the ACIP and similar oversight bodies.
Nevertheless, Wayne Koff, an immunologist leading New York City’s nonprofit human vaccine program, stated that concerns about vaccine durability have been far from sufficient to date. “If you can figure this out, you can make all vaccines better,” said Koff.
More than 150 years ago, a natural experiment conducted in the rocky volcanic archipelago between Scandinavia and Iceland demonstrated that infection can induce lifelong immune memory. In 1781, measles spread rampant among the residents of the Faroe Islands. For the next 65 years, the disease did not reappear on this isolated island until a visitor reintroduced it. A subsequent study found that none of the individuals who survived the initial outbreak on the island contracted the disease again. Their aged immune systems had retained memory of the virus.
Subsequently, vaccine developers have been striving to replicate this durable immune memory function. They have created harmless mimics of pathogens—such as viruses, bacteria, or their toxins—to train the immune system to recognize actual pathogens and rapidly mount a robust immune response. Immunologists believe that memory B cells are key to this immune response for many infectious diseases. When confronted with known enemies, these cells rapidly expand and produce large quantities of antibodies that latch onto invaders, preventing infection. Vaccines can also cultivate “killer” T cells. These T cells eliminate infected cells when antibodies prove ineffective.
“When we use vaccines to prevent pathogens, antibodies play a major role in the protective mechanism,” said Mark Slifka, an immunologist specializing in vaccine research at the Oregon National Primate Research Center. “For diseases that are more difficult to prevent with vaccines, such as tuberculosis, malaria, and HIV, antibodies can provide some level of protection, but you also need T cells to be involved.”
Vaccine manufacturers are engaged in heated debate over the optimal approach to triggering these responses. Some insist that live pathogens, such as attenuated strains or those genetically modified to remove toxicity, can act as a “Trojan horse,” inducing the most durable and potent immune responses. The measles vaccine, which uses an attenuated virus, has already saved countless lives from the ravages of measles. Pulendran, however, believes that this view oversimplifies the matter. He and others argue that killed pathogens or genetically engineered variants of pathogens can be equally effective.
Regarding influenza, we have both live-attenuated and inactivated viral vaccines. However, neither provides sufficiently robust protection. Even when strictly matched to circulating influenza strains, these two types protect only about 60% of vaccinated individuals. Furthermore, the immune responses they elicit wane rapidly.
In a 2018 review on the durability of influenza vaccines, researchers concluded that the effectiveness of the flu vaccine may last only up to 90 days after vaccination. The article, published in Clinical Infectious Diseases, further pointed out that 20% of Americans receive their flu shots at the specific time point of late September—meaning the vaccine’s protection may wane by the peak flu season in January and February of the following year. “The longer it has been since your last flu vaccination, the higher your risk of contracting influenza. This is critically important,” said Kunal Rambhia, a pharmacy expert and doctoral candidate, who was a co-author of the study.
Rambhia stated that, given that more than 100 million Americans receive vaccinations annually, it is necessary for the relevant authorities to urge people to get vaccinated in a timely manner. “They have made the right decision now. They acknowledged that the vaccine may be less effective toward the end of the flu season.”
He and others also pointed out that there are benefits even when vaccines “fail.” For those who contract influenza despite being vaccinated, their symptoms are significantly milder. This mechanism of partial protection was first observed more than a century ago with the smallpox vaccine. While the smallpox vaccine provided complete disease prevention only during the first decade or so after vaccination, it effectively protected individuals from severe illness and death.
Before the mumps vaccine entered the market in 1967, more than 90% of American children had contracted this viral disease. Mumps causes swelling of the salivary glands, leading to facial puffiness and fever. By the year 2000, only a few hundred cases were reported annually in the United States. However, in 2006, mumps outbreaks occurred on university campuses in the Midwest. Statistics showed that there were a total of 6,500 cases by the end of 2006. Among those infected, approximately 85% had received the recommended two doses of the mumps vaccine. Despite widespread vaccination, mumps outbreaks have continued to occur on U.S. university campuses and in densely populated religious communities.
Some researchers have speculated that vaccine failure is due to viral mutations enabling the virus to evade immunity generated by vaccination. However, Joseph Lewnard, an epidemiologist at the University of California, Berkeley, and Yonatan Grad, an immunologist at the Harvard T.H. Chan School of Public Health in Boston, recently analyzed mumps incidence data from the United States, Canada, Europe, and Asia. They reported last year in Science Translational Medicine that the disease exhibits a peak incidence among individuals aged 18 to 29 years. Lewnard and Grad argue that this age distribution suggests waning vaccine efficacy, as new mumps strains arising from genetic mutations would be expected to infect other age groups equally. Similar signs of declining vaccine-induced immunity have also been observed in more than a dozen studies conducted by researchers worldwide.
Lewnard and Grad’s model indicates that administering a third dose of the mumps vaccine at around age 18, followed by booster shots every 10 years, can substantially reduce the likelihood of outbreaks. Researchers note that since 1991, the U.S. military has provided mumps vaccine boosters to all new recruits, and no mumps outbreaks have occurred in the armed forces since then.
Vaccine-induced immunity wanes over time, and the pattern of decline varies by disease. Based on outbreak case data and rates of vaccine waning, mathematical models can predict the duration of immunity conferred by completion of the full vaccination series.
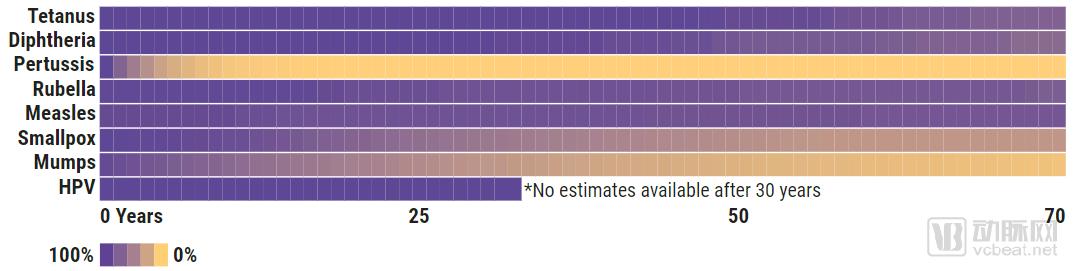
Figure: Durability varies across different vaccines; from top to bottom, they are tetanus, diphtheria, pertussis, rubella, measles, smallpox, mumps, and HPV.
Source: (GRAPHIC) N. DESAI/SCIENCE; (DATA) JOSEPH LEWNARD/UC BERKELEY; HIROSHI NISHIURA/HOKKAIDO UNIVERSITY; T. F. SCHWARZ ET AL., CANCER MED, 11, 2723, 2017; N. KLEIN ET AL., VACCINE, 35, 3395 2017
The mumps outbreak in Arkansas in August 2016 demonstrated that isolating waning immunity from other factors affecting vaccine efficacy is not straightforward. More than half of the cases in this outbreak were among school-aged children, and, as reported in The Lancet Infectious Diseases, 92% of these children had been vaccinated according to the standard schedule. “Initially, we thought the data must be wrong because they did not align with our models,” said Grad.
The outbreak persisted until September 2017, primarily affecting the Marshallese population and causing nearly 3,000 cases. These individuals lived in a large community in rural Arkansas, attended the same church, and resided in equally crowded housing. In densely populated communities, high concentrations of the mumps virus overwhelmed people’s immune systems. “The protection provided by the vaccine is not binary,” said Grad. “The more exposure you have to the source of infection, the more likely you are to become infected.”
In 2018, the ACIP began recommending a third dose of mumps vaccine for individuals in “areas at high risk for disease outbreaks.”
As understanding of the rate of waning vaccine-induced immunity has deepened, concerns have emerged in recent years regarding certain public health decisions. In 2016, the World Health Organization (WHO) in Geneva, Switzerland, revised its mandatory requirements for yellow fever vaccination. The yellow fever vaccine, a live-attenuated vaccine that has been widely used since the 1940s, has helped millions avoid infection and death. Three years prior, an expert committee on yellow fever reported in a document that only 12 cases of yellow fever had been identified among more than 540 million people vaccinated worldwide against the disease. Consequently, the WHO changed its yellow fever vaccination schedule from requiring a booster dose every 10 years to recommending a single lifetime dose.
Slifka considers this a mistake. In addition to his role as a researcher, he is the President of Najít Technologies, a company that produces a novel yellow fever vaccine. In the December 2016 issue of Expert Review of Vaccines, he and his colleague at Najít, Ian Amanna, pointed out that behind the near-perfect protection perceived by expert committees lies another critical issue: many vaccinated individuals have never been exposed to the yellow fever virus. They cited a study from Brazil in their article, which reported 459 cases of yellow fever among individuals in Brazil who had been vaccinated no more than 35 years prior. Among these patients, 52% had received their last vaccination more than 10 years earlier. “Only 80% of people develop lifelong immunity after a single dose of the yellow fever vaccine,” Slifka stated.
Data on yellow fever antibodies support this argument. Slifka and Amanna noted that, in a review by the Centers for Disease Control and Prevention (CDC), researchers analyzed blood levels of yellow fever antibodies capable of “neutralizing” the virus. This metric is critical to vaccine effectiveness. The review included nine relevant studies. Four of these studies were conducted among populations in areas where yellow fever virus is transmitted, and subsequently found that 97.6% of individuals still had detectable concentrations of yellow fever virus antibodies ten years after vaccination. However, in the other five studies, which focused on regions with little or no yellow fever, only 83.7% of vaccinated individuals maintained this level of immunity. Slifka believes that this finding indicates that people gradually lose the protection provided by the vaccine without periodic exposure to the pathogen. “We need at least one booster dose,” he said.
Plotkin stated that he also believes the WHO should reconsider its recommendation to reduce booster vaccinations.
A spokesperson for the World Health Organization’s expert committee responsible for vaccine assessment stated that they would continue to review new data on yellow fever cases and closely monitor the duration of immunity in populations receiving a single dose. “The evidence to date is insufficient to support the need for booster vaccination,” the spokesperson said. He also noted that the WHO had previously cautioned against overinterpreting antibody data.
In 1991, some vaccinologists also questioned the decision to switch to a safer pertussis vaccine. In the preceding decades, vaccines made from inactivated *Bordetella pertussis* had achieved tremendous success in the United States and other countries. However, this “whole-cell” vaccine became the focal point of an anti-vaccination movement approximately 40 years ago, due to claims—still somewhat controversial—that the inactivated vaccine caused severe neurological damage in rare cases. Consequently, it was later replaced by inactivated pertussis toxin.
The novel pertussis vaccine has been formulated as a triple vaccine in combination with tetanus and diphtheria vaccines. The Advisory Committee on Immunization Practices (ACIP) recommends six doses of this triple vaccine between infancy and 12 years of age. Subsequently, booster immunization for tetanus and diphtheria is recommended every 10 years for adults. Despite rigorous implementation of vaccination programs, California experienced two large-scale pertussis outbreaks during the 2010–11 and 2014–15 periods, resulting in approximately 20,000 cases.
To determine whether waning immunity was a contributing factor, Kaiser Permanente Northern California examined more than 4,000 children from 2006 to 2015. Through analysis, the team found that immune protection in children who had received the fifth dose of the vaccine (typically administered at ages 4–6 years) declined by approximately 27% per year. “We are becoming increasingly vulnerable to pertussis until a vaccine that provides more durable protection becomes available,” concluded the researchers in their paper published in Vaccine.
Slifka stated that replacing whole-cell vaccines with acellular vaccines was unnecessary and even erroneous. “Acellular vaccines provide 80% to 90% protection immediately after vaccination, but this protection wanes rapidly over the subsequent years,” he said. “This leaves many children highly susceptible to infection between the fifth and sixth vaccine doses, administered at ages 11 or 12.” (While pertussis causes only mild symptoms in adolescents and adults, it can be fatal in young children.)
Ironically, the other two components of the triple vaccine exhibit surprisingly durable protection. The primate center where Slifka works draws blood from experimental animals to monitor potential infections in monkeys and other non-human primates. Slifka, Amanna, and their colleagues collected blood samples over a 26-year period and assessed the rate of antibody decline against tetanus and diphtheria bacteria following vaccination. They reported in PLOS Biology in 2018 that individuals do not begin to lose protective immunity against these two pathogens until 40 years after vaccination. “Our immunity levels are much higher than we previously thought,” Slifka said.
Slifka pointed out that the World Health Organization no longer recommends booster immunization against tetanus and diphtheria for adults who received complete vaccination in childhood. He believes that the ACIP should also consider withdrawing its recommendation for booster immunization. He estimates that reducing these vaccinations would save the United States approximately $1 billion annually.
The phenomenon that one vaccine in the triple-vaccine regimen wanes rapidly while others remain effective for nearly a lifetime only adds to the mystery of vaccine durability, rather than providing clues for its study. However, a specific vaccine targeting HPV has offered new insights.
Concerned that attenuated or inactivated HPV vaccines might still contain carcinogenic viral components, researchers used genetic engineering to modify another virus to produce non-toxic HPV surface proteins. These proteins self-assemble into so-called virus-like particles (VLPs). Trials have shown that nearly all individuals vaccinated with these non-infectious VLPs develop high levels of HPV-neutralizing antibodies. Although these antibody levels decline slowly after two years, they provide immune protection for at least ten years. John Schiller, an oncologist and developer of this vaccine, stated, “Before we conducted clinical trials with the vaccine, we really did not know that we would elicit such highly effective and durable antibody responses.”
VLPs have changed people’s understanding of vaccine durability. Before VLPs, it was widely believed that durability mainly resulted from the reactivation and proliferation of memory B cells upon infection. Schiller pointed out that neutralizing antibody levels in the blood of HPV vaccine recipients remain stable over the years. “If it followed the pattern we previously assumed, you would expect to see antibody levels fluctuate,” he said.
Schiller and others believe that VLPs induce the generation of another type of B cell, known as long-lived plasma cells (LLPCs). These cells reside in the bone marrow and continuously produce specific antibodies against various foreign antigens. “Virus-like particles are clearly the best way to induce LLPCs,” says Schiller.
With the success of HPV vaccines, virus-like particles (VLPs) have become a popular vaccine strategy. The hepatitis E vaccine available on the Chinese market utilizes VLP technology. VLP-based vaccines for influenza, norovirus, chikungunya, encephalitis, malaria, and dengue fever are also under development.
However, no one knows exactly how VLPs stimulate the immune system to produce LLPCs. Schiller pointed to the work of Rolf Zinkernagel, a Nobel laureate at the University of Zurich in Switzerland, and his then-graduate student Martin Bachmann. Twenty-five years ago, they reported that densely packed, highly repetitive proteins on the surface of viruses elicit the strongest antibody responses. VLPs constitute precisely such a structure. In theory, this allows viral antigens to “cross-link” numerous receptors on the surface of B cells. This, in turn, triggers a cascade of signals within immune cells, leading to the production of potent, long-lasting antibodies. But what are the precise mechanisms involved? “That question is worth its weight in gold,” said Slifka.
“He said these unknowns were frustrating. He was also disheartened by the disconnect between the laboratory’s vaccine research and the epidemiological survey data. ‘How can we address this issue?’ he asked. ‘We need to facilitate communication between epidemiologists and immunologists so they can share their findings. Everyone stands to learn a great deal from this.’”
The 2019 flu season in North America is drawing to a close. The Centers for Disease Control and Prevention (CDC) estimates that the virus infected nearly 40 million people, resulted in 500,000 hospitalizations, and caused up to 50,000 deaths. Meanwhile, Stanley Plotkin and his wife, who received another flu vaccination this January, both remained healthy. This suggests that we should pay greater attention to the durability of vaccine-induced immunity, as there is no one-size-fits-all or permanent protective solution.
Original Article Link:https://www.sciencemag.org/news/2019/04/how-long-do-vaccines-last-surprising-answers-may-help-protect-people-longer