Global R&D Pipeline Trends Report: Phase I Trials Growing More Complex, Respiratory Diseases Emerge as Highest ROI Therapeutic Area
On April 23, 2019, IQVIA, an integrated provider of information technology and healthcare services, released its annual report, “The Changing Landscape of Research and Development.” The report provides a comprehensive overview of global drugs under development, examining aspects such as innovation, drivers of drug growth, and improvements in clinical trial productivity. Previously, VCBeat New Medicine (biobeat1) had already compiled and translated the section of the report focusing on the development of clinical drug pipelines.
This article focuses on the translational efficiency of clinical trials. By aggregating inputs and outputs, IQVIA has developed a methodology to calculate the translational efficiency of clinical trials and applied it to data analysis across different therapeutic areas and clinical phases. Through further analysis, IQVIA has outlined the trends in clinical trial translational efficiency in recent years and forecasted its future trajectory.
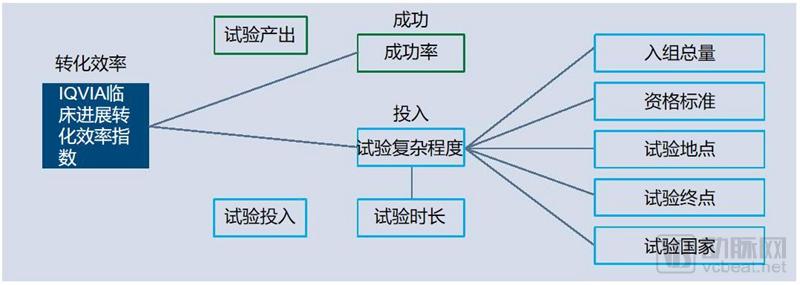
The factors influencing conversion efficiency are primarily trial success rate, trial complexity, and trial duration. To characterize the conversion efficiency of clinical trials, IQVIA has developed a specific algorithm based on these three factors, providing a mathematical definition for clinical trial conversion efficiency.

Note: 97.61 is a coefficient established by IQVIA based on existing data to ensure that the final conversion efficiency falls within the range of 0–100.
The complexity of a clinical trial is primarily influenced by five factors: total enrollment, eligibility criteria, trial sites, trial endpoints, and countries involved.
Based on a composite calculation of various factors, the algorithm ultimately yields a conversion efficiency score ranging from 0 to 100, representing the conversion efficiency of clinical trials in specific therapeutic areas. A lower score indicates that clinical trials in the relevant field are more complex, take longer to complete, and have lower success rates; conversely, a higher score suggests that such trials are simpler, require less time, and achieve higher success rates.

Figure: Trends in Conversion Efficiency Across Disease Areas, 2010–2018
Across all disease areas, oncology has consistently demonstrated the lowest translational efficiency. Furthermore, from 2010 to the present, the compound annual growth rate (CAGR) of translational efficiency in oncology has been only approximately 2%.
The translational efficiency across many disease areas is declining, particularly for infectious diseases, respiratory diseases, neurological disorders, glucose metabolism/non-alcoholic steatohepatitis (NASH), and endocrine diseases. Since 2010, the decline in translational efficiency has been most pronounced for glucose metabolism/NASH-related diseases, reaching 55%; this is followed by infectious diseases, with a 33% decrease. From 2011 to the present, the translational efficiency for respiratory diseases has significantly dropped by more than 30%.
On the other hand, the conversion efficiency for cardiovascular diseases has increased by as much as 40% from 2010 to present, with a compound annual growth rate (CAGR) of up to 4%.
Immune system diseases have shown the most stable performance across all categories, with conversion rates remaining virtually unchanged from 2010 to the present. This stability may be attributed to consistent clinical trial designs and success rates.

Figure: Trends in Conversion Efficiency of Clinical Trials by Phase, 2010–2018
Since 2010, the overall translation efficiency of clinical trials has shown a declining trend. This situation is mainly influenced by the translation efficiency of Phase I clinical trials. The translation efficiency of Phase I clinical trials decreased by more than 50% from 2010 to 2018, while the translation efficiency of Phase II/III clinical trials remained basically unchanged.
The sharp decline in the translational efficiency of Phase I clinical trials is primarily driven by increasing trial complexity. Since 2013, the complexity of Phase I clinical trials has risen by 35%, while success rates and trial durations have remained largely unchanged. The disease categories experiencing the greatest declines in Phase I translational efficiency are primarily infectious diseases, immune system disorders, respiratory diseases, neurological disorders, metabolic liver diseases (such as those related to blood glucose and non-alcoholic steatohepatitis), and endocrine disorders. In contrast, the translational efficiency of Phase I clinical trials for oncology and vaccines has remained stable, with cardiovascular diseases even showing an improvement.
The translation efficiency of Phase II/III clinical trials has remained stable, with a slight increase observed in Phase III clinical trials. In Phase II clinical trials, the translation efficiency for heart disease increased by 5% between 2013 and 2017. The average translation efficiency for oncology Phase III clinical trials was 8.4 between 2010 and 2013, rising to 10.5 by 2018.
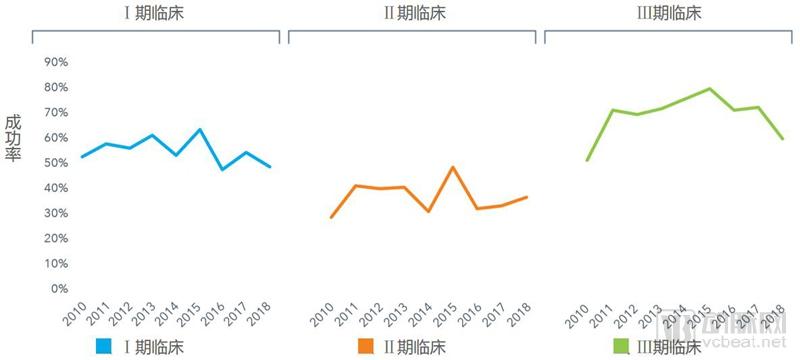
Figure: Trends in Success Rates of Clinical Trials by Phase, 2010–2018
From 2010 to 2018, the success rate of Phase I clinical trials decreased by 7%. The success rates in most subfields declined, while those for neurological disorders, vaccines, and cardiovascular diseases remained largely unchanged.
Phase II clinical trial success rates have remained consistently stable. Among various disease categories, the success rate for Phase II clinical trials in glycemic disorders and non-alcoholic steatohepatitis (NASH) declined from 67% in 2012 to 35% in 2018, whereas for cardiovascular diseases, it increased from 22% in 2010 to 44% in 2018.
In the 2018 Phase III clinical trials, success rates across various diseases ranged from 38% for cardiovascular diseases to 89% for immune system disorders. From 2010 to 2017, the compound annual growth rate (CAGR) of Phase III clinical trial success rates reached as high as 5%, yet the success rate in 2018 declined by 15%. This trend was primarily driven by outcomes in cardiovascular and infectious diseases.
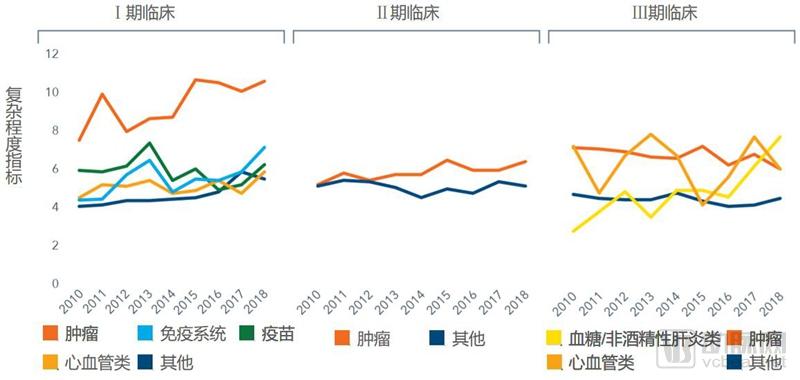
Figure: Trends in the Complexity of Clinical Trials Across Different Disease Areas and Clinical Phases, 2010–2018
As mentioned above, the complexity of a clinical trial is primarily influenced by five factors: total enrollment size, eligibility criteria, trial sites, trial endpoints, and countries where the trial is conducted.
The number of patients participating in clinical trials in 2018 increased by 10% compared to 2017. Patients with oncological and neurological diseases accounted for the largest proportions.
The overall complexity of clinical trials has shown an upward trend across nearly all dimensions. Among the five factors influencing trial complexity, only the number of trial sites and trial countries has not increased.
The complexity of Phase I clinical trials has increased significantly, rising by 35% since 2013. This increase is particularly pronounced in the fields of oncology and immune-mediated diseases.
Meanwhile, the complexity of Phase II/III clinical trials has remained largely unchanged. However, within this category, the complexity of Phase III clinical trials for diabetes and non-alcoholic steatohepatitis (NASH) reached three times the 2010 level by 2018.
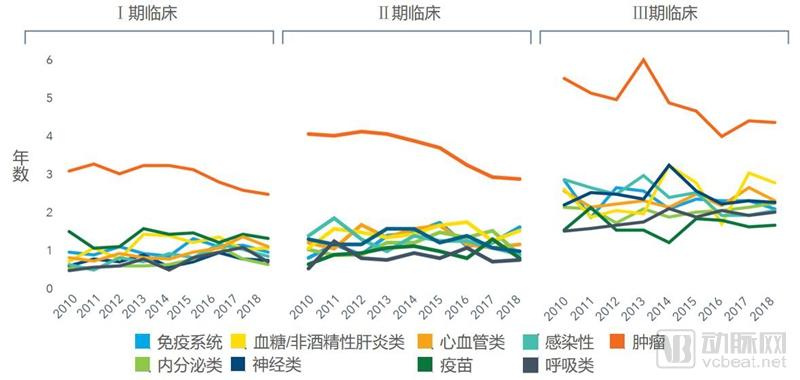
Figure: Trends in Trial Duration Across Different Clinical Phases by Disease Area, 2010–2018
Over the past five years, changes in clinical trial duration have varied across different disease areas.
For Phase I clinical trials, the duration of trials in most disease areas is increasing. This is likely because developers hope to fully test the effectiveness of drugs at an earlier stage.
Since 2013, the average duration of oncology clinical trials has decreased significantly, with Phase I trials shortened by 7 months, Phase II trials by 11 months, and Phase III trials by more than one year.
IQVIA identifies the following eight aspects as key factors currently influencing clinical trial design, duration, and success rates.
1.Digital Health/Mobile Technology: By remotely monitoring drug efficacy and safety, digital health technologies will be able to enhance patient safety, enable digital trial formats, and reduce the burden on sites.
2. PRO(Patient-Reported Outcomes, patient-reported clinical symptoms): Enhancing the focus on PROs will provide new perspectives on patient experience, drug efficacy, and safety outside clinical settings, and shorten trial duration through the adjustment of clinical endpoints.
3. Real-World Data: Real-world data will be used to optimize trial design and accelerate the trial process by assisting in the selection of investigators and study sites.
4. Predictive Analytics / Artificial Intelligence: Predictive analytics and artificial intelligence will extract new insights from data for clinical validation, reduce clinical trial risks, and accelerate enrollment through patient screening.
5. Drug Type: Shifting the drug development focus toward targeted therapies and biologics will enhance efficacy and success rates while accelerating R&D speed, but may require longer patient follow-up periods.
6. Biomarker Testing: Applying biomarker testing to clinical trials will precisely target patient populations, making treatments more effective and ultimately improving efficacy, safety, and success rates.
7. Regulatory Environment: Changes in the regulatory landscape will further support precision medicine approaches and novel experimental designs, and accelerate drug review and regulatory success.
8. Pre-screened Patient Pool / Direct-to-Patient Recruitment: Pre-screening patient populations and direct patient recruitment will facilitate trial enrollment, help achieve recruitment targets, reduce trial duration, and improve patient accessibility.
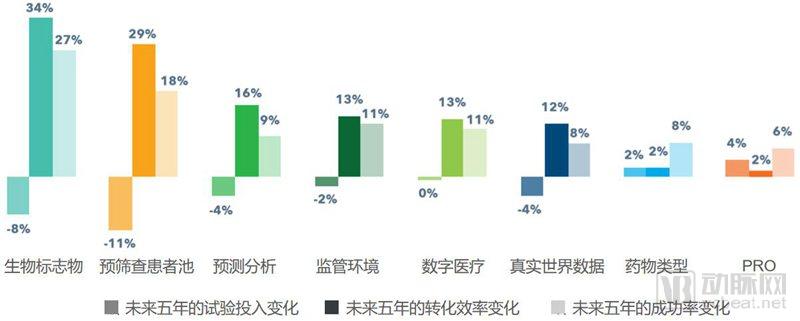
Figure: Forecast of the Impact of Eight Major Trends on Clinical Trials Over the Next Five Years
All eight major trends are expected to enhance the success rate of clinical trials, thereby improving translational efficiency. Meanwhile, they will also influence the translational efficiency of clinical trials in terms of trial complexity and duration (collectively referred to as trial investment). Most trends will reduce trial investment, with only drug type and PROs leading to an increase.
Biomarkers and pre-screened patient pools are expected to have the greatest impact on translation efficiency over the next five years, with projected contributions of 34% and 29%, respectively. Among these, the pre-screened patient pool, ranking second, is anticipated to exert the most significant influence on trial investment across all trends, potentially reducing trial costs by 11% while increasing the success rate by 18%.
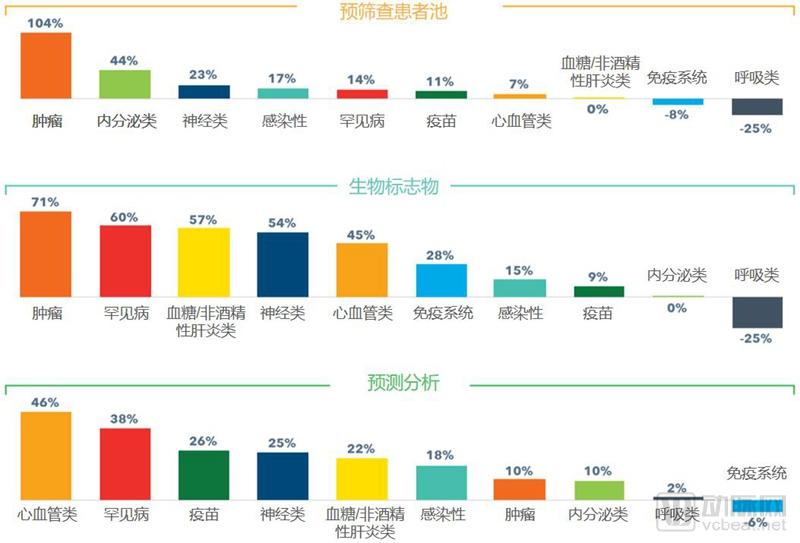

Figure: Forecast of the Impact of Various Trends on the Conversion Efficiency of Clinical Trials Across Different Disease Categories Over the Next Five Years
Beyond oncology, biomarkers will also improve the translational efficiency of clinical trials for rare diseases, glucose metabolism disorders/non-alcoholic steatohepatitis (NASH), neurological disorders, and cardiovascular diseases by more than 45%.
Both pre-screened patient pools and biomarkers have demonstrated negative effects on the translational efficiency of clinical trials for respiratory diseases. The primary challenge with pre-screened patient pools lies in the difficulty of patient recruitment, whereas the main obstacle for biomarkers is the inherent difficulty in developing them for respiratory conditions such as asthma and chronic obstructive pulmonary disease (COPD).
Predictive analytics is expected to have a positive impact on the clinical trial conversion efficiency for all disease types except immune system diseases, including respiratory diseases where biomarkers and pre-screened patient pools may have a negative impact.
As one of the primary factors influencing the complexity of clinical trials, shifts in drug types are expected to increase trial investments across all therapeutic areas except neurological disorders and oncology. This is because many clinical trials are increasingly focusing on cutting-edge modalities such as RNA interference (RNAi), gene therapy, and biologics. Meanwhile, changes in drug types are also projected to improve clinical trial success rates in most disease areas.
PRO is another major factor influencing the complexity of clinical trials. The incorporation of PROs in clinical trials is expected to increase trial costs by 4%. In particular, in the fields of respiratory diseases and immune system disorders, trial costs may rise by 20% and 60%, respectively. This also means that PROs will have a significant negative impact on the translational efficiency of clinical trials in these two areas.
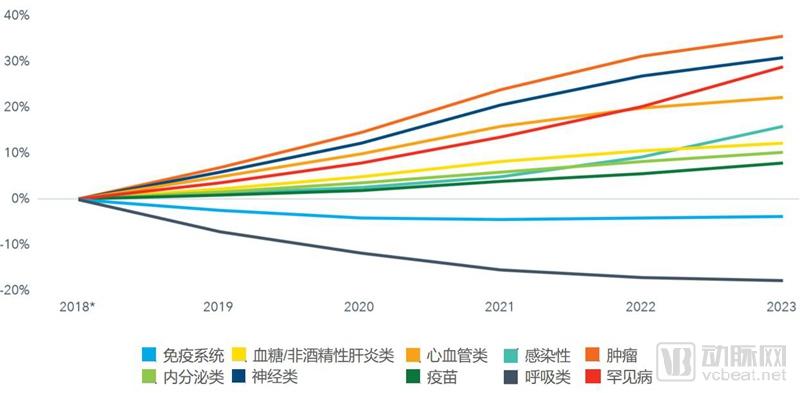
Figure: Forecast of Changes in Clinical Trial Conversion Efficiency Across Different Disease Categories Over the Next Five Years
Over the next five years, clinical trial translation efficiency is projected to improve significantly for oncology, neurological disorders, rare diseases, and cardiovascular diseases. Among these, oncology is expected to witness the most rapid increase in translation efficiency. In contrast, translation efficiency for immune system disorders and respiratory diseases may decline.
Clinical trial translation efficiency has remained consistently high for infectious diseases and endocrine disorders, and is projected to further increase in these two fields over the next five years.

Figure: Forecast of the Specific Impact of Different Trends on Various Disease Categories Over the Next Five Years
Pre-screening patient pools and biomarkers will significantly accelerate the progress of oncology clinical trials and ultimately improve their success rates. Neurological diseases are most profoundly impacted by biomarkers, alongside changes in management approaches and digital health.
Only real-world data and predictive analytics are expected to have a positive impact on respiratory diseases, both of which are based on big data analysis.

Figure: Forecast of the Impact of Various Trends on Conversion Efficiency Across Different Clinical Stages Over the Next Five Years
Phase I clinical trials exhibit the smallest change in conversion efficiency, with most of the eight trends impacting Phase I trial conversion efficiency by only 4–10%. Digital health will have an impact of more than 15% on Phase II/III trials, but it has almost no effect on the conversion efficiency of Phase I clinical trials.
Although most trends have a significant impact on Phase II/III clinical trials, not all of these impacts are positive. Changes in drug types will reduce the conversion efficiency of Phase III clinical trials by approximately 6%. This situation is likely due to the need for long-term safety monitoring of new biotechnologies, which prolongs the duration of trials at this stage.
Changes in the regulatory environment will increase the conversion efficiency of all three phases of clinical trials by 10–16%, with Phase II clinical trials showing the greatest improvement.
PROs had virtually no impact on all three phases of clinical trials. Predictive analytics will increase the conversion efficiency of Phase III clinical trials by up to 20%.