Global R&D Pipeline Trends Report: Oncology Pipelines Surge by 26%, Alzheimer’s Drug Failures Reach 86
On April 23, 2019, IQVIA, an integrated provider of information technology and medical services, released its annual report, “The Changing Landscape of Research and Development.” The report provides a comprehensive overview of global drugs under development from the perspectives of innovation, drivers of drug growth, and improvements in clinical trial productivity. Previously, VCBeat New Medicine (biobeat1) had organized and translated sections of the report covering the development of clinical drug pipelines and the translational efficiency of clinical trials. This article presents major breakthroughs in the research, development, and approval of clinical drug pipelines.
Number of Pipeline Assets by Clinical Stage Across Different Disease Areas
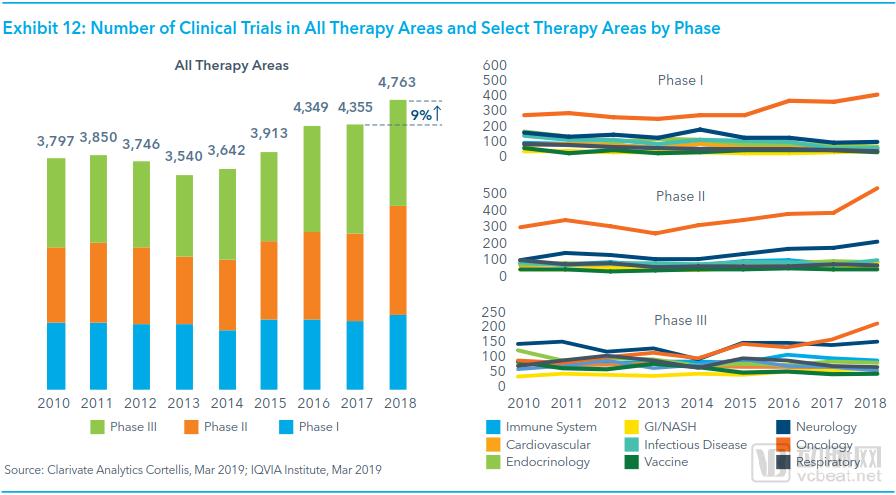
In 2018, there were a total of 4,768 Phase I–III clinical trials, representing a 9% increase from the previous year and a 35% increase compared to data from five years earlier.
In 2018, the number of clinical trials across all phases related to gastrointestinal (GI) disorders, non-alcoholic steatohepatitis (NASH), and oncology saw a significant increase. Specifically, clinical trials related to GI/NASH rose by 42%, while those related to oncology increased by 27%; in contrast, the number of clinical trials for endocrine and respiratory diseases declined.
Since 2016, the number of oncology-related clinical trials in Phase I and Phase II studies has continued to rise, while the number of non-oncology trials has steadily declined, offsetting each other. Consequently, the overall number of clinical trials in these two phases has maintained a relatively stable growth.
The number of Phase II clinical trials in 2018 increased by 26% compared with 2017, and by 61% compared with 2013.
The growth in the number of Phase II clinical trials is primarily driven by an increase in oncology-related pipelines; however, it is worth noting that the number of pipelines for neurological and hematologic diseases entering Phase II has also risen.
Average Comprehensive Progression Time Across Clinical Phases
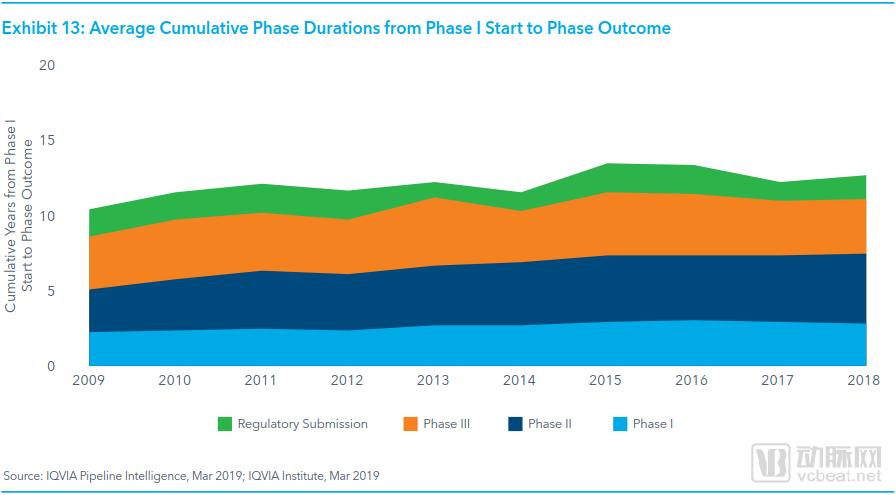
The total time elapsed from Phase I clinical trials in humans to the final market launch of a drug, regardless of success or failure, is referred to as the comprehensive development timeline. Over the past decade, the comprehensive development timeline for all drug pipelines has continued to increase. Compared with 2010, the comprehensive development timeline for all pipelines rose by 26% in 2018.
In 2018, the overall development timeline for all pipelines reached 12.5 years, which is 6 months longer than the overall average in 2017. Compared with the data from 2010,
In 2018, the average comprehensive development timeline for successfully launched oncology pipelines was 11.6 years, lower than the 12.6-year average in 2010. Over the past three years, regulatory agencies’ accelerated review pathways have benefited the approval of oncology-related pipelines, reducing the time from submission to approval to approximately one year.
Over the past decade, the average total development time for successfully launched rare disease drugs was 12.2 years, with rare disease drug pipelines also benefiting from novel approval pathways and review mechanisms implemented by regulatory agencies.
Average Overall Success Rates of Clinical-Stage Pipelines, 2008–2018
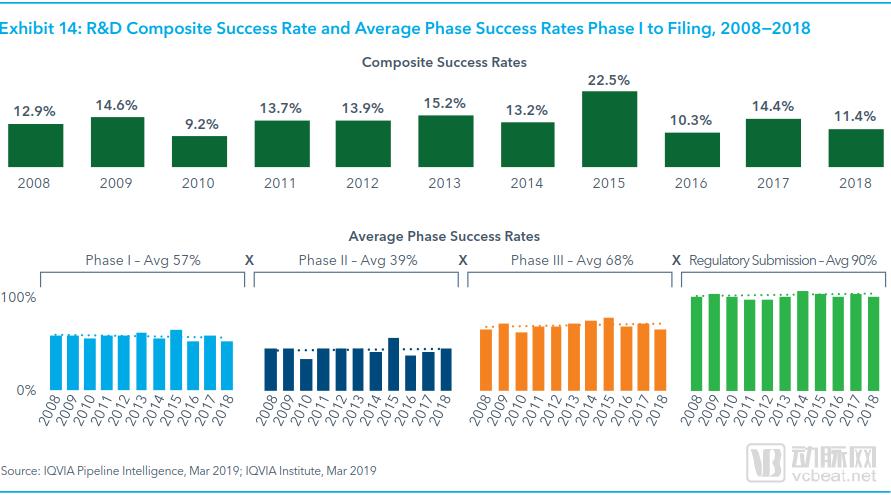
The overall success rate, defined as the probability of a drug candidate progressing from entry into clinical trials to successful trial completion and subsequent submission for review by regulatory authorities, was only 11.4% for Phase I clinical pipelines in 2018, down from 14.4% in 2017.
Over the past decade, the overall success rate of Phase I clinical pipelines has been unstable, fluctuating up and down. The data from 2015 stands out most prominently, with the overall success rate of Phase I clinical pipelines reaching as high as 22%.
The overall success rate of the Phase I clinical pipeline in 2018 was unremarkable, falling below the average level observed from 2008 to 2017. This may be partly attributed to the declining success rates of Phase III and Phase I clinical trials.
In 2018, the success rates of Phase I and Phase III clinical trials both declined by approximately 7.5%, while the success rate of Phase II clinical trials increased slightly, by less than 1%.
Over the past decade, drug development has increasingly shifted toward oncology, biologics, and therapies for specific diseases.
From 2009 to 2018, the average overall success rate for oncology pipelines was 12%, slightly lower than the 14.1% average for other drug pipelines.
Overall Launch Success Rate of Pipelines Across Different Disease Areas in 2018
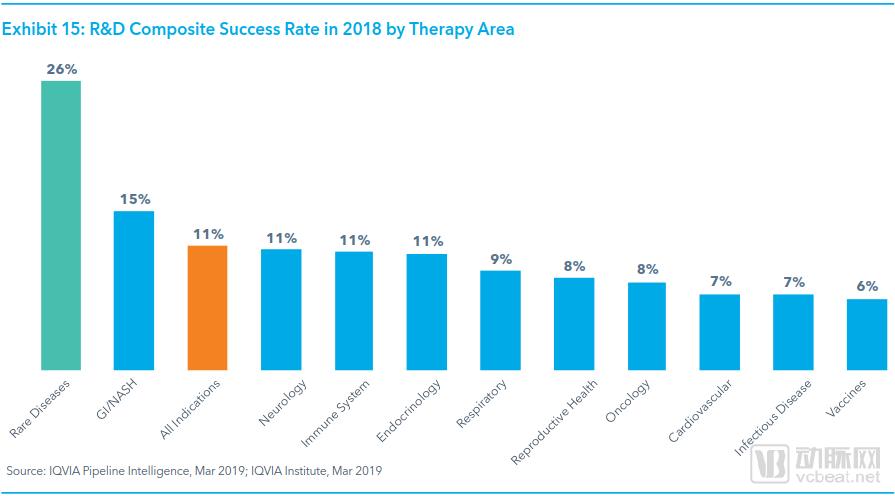
In 2018, the overall success rate of drug pipelines for gastrointestinal disorders and non-alcoholic steatohepatitis (NASH) was the only therapeutic area above the average. These drugs typically have broad indications, with recently approved indications including traveler’s diarrhea, chronic idiopathic constipation, ulcerative colitis, and Crohn’s disease.
The overall approval success rate for neurological drug pipelines is 11%. In 2018, several blockbuster drugs for neurological disorders received approval, including three innovative biologics for migraine treatment, as well as several medications for rare neurological conditions such as Lennox-Gastaut syndrome, Dravet syndrome, and hereditary transthyretin-mediated amyloidosis.
The overall probability of success for infectious disease vaccine pipelines reaching the market is the lowest, at merely 6%. This is partly because the development of such drugs faces numerous challenges specific to these diseases. For instance, high R&D costs, extreme difficulties in patient recruitment and long-term follow-up studies, and an incomplete understanding of the mechanisms by which vaccines trigger immune responses against specific diseases all contribute to this low success rate.
Although the overall success rate for all drug pipelines reaching market approval was nearly 30% in 2018, the overall success rate for oncology drug pipelines was only 8%. This discrepancy is partly due to the high complexity of clinical trials for oncology drugs, and partly because conceptual or dose-finding studies in Phase II clinical trials fail to adequately support Phase III clinical trials.
Key Advances in Oncology, Infectious Diseases, and Neurological Disorders
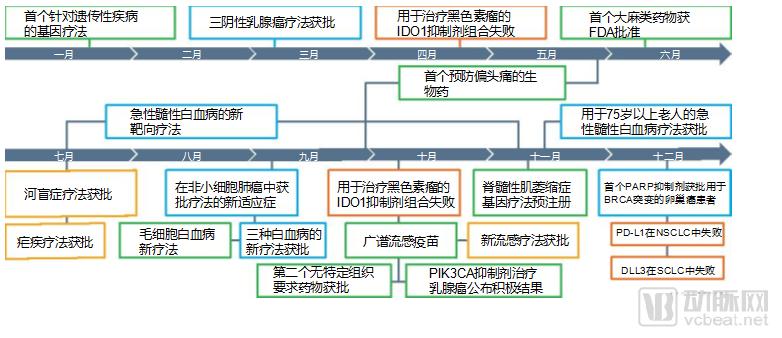
In 2018, there were many key advancements in the field of oncology, particularly for acute myeloid leukemia (AML), a therapeutic area that had seen no new approvals for many years but gained approval for three new targeted therapies this year. New treatments were also approved for non-small cell lung cancer (NSCLC) with EGFR mutations and ALK positivity. Larotrectinib became the second “tumor-agnostic” anticancer drug approved in 2018, targeting specific genetic mutations rather than specific tumor sites.
In the fields of breast and ovarian cancer, the PARP inhibitor olaparib became the first targeted therapy approved for the treatment of triple-negative breast cancer. Olaparib was also the first PARP inhibitor approved for the treatment of BRCA-mutated ovarian cancer. Furthermore, Phase III clinical trials of alpelisib demonstrated that its use in patients with PIK3CA-mutated breast cancer nearly doubled their progression-free survival.
In 2018, drug development in the oncology field also encountered numerous setbacks. The development of DLL3 antibodies as targeted therapies for small cell lung cancer and PD-L1 inhibitors for non-small cell lung cancer failed successively, while IDO inhibitors for melanoma demonstrated poor efficacy both as monotherapy and in combination regimens.
In the field of infectious diseases, moxidectin was approved for the treatment of river blindness, marking the first new therapy approved for this condition in 20 years. Tafenoquine, a 40-year-old drug, received U.S. approval for a new indication in the treatment of malaria. In 2018, a novel anti-influenza antiviral drug was approved, and a broad-spectrum influenza vaccine entered Phase III clinical trials.
In the field of neurological disorders, 2018 marked a significant breakthrough for this class of drugs with the approval of three CGRP antagonists for the prevention of acute and chronic migraine. The first cannabis-derived medication also received FDA approval for the treatment of Dravet syndrome, a rare form of epilepsy.
In the field of gene therapy, Luxturna, the first gene therapy for genetic disorders, was approved for the treatment of Leber congenital amaurosis. The first gene therapy for spinal muscular atrophy has been submitted to the FDA for registration and approval.
Average R&D Cycle for Alzheimer’s Disease
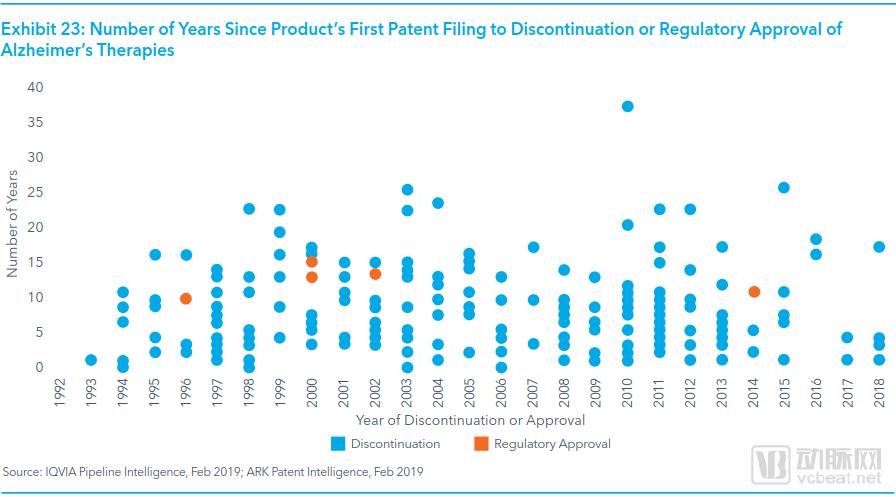
By 2030, the global number of individuals with dementia is projected to reach 82 million, with 60% to 80% of these patients likely having Alzheimer’s disease. However, only five symptomatic treatments have been approved for Alzheimer’s disease to date, and no medications for prevention or disease-modifying therapy have received approval.
From 2008 to 2018, only one Alzheimer’s disease drug was approved, while the remaining 86 candidates were discontinued. The approved drug was merely a combination therapy of two previously approved Alzheimer’s medications.
There are many reasons for the failures in Alzheimer’s disease drug pipelines, such as insufficient understanding of the disease’s etiology, inadequate animal models, difficulties in patient recruitment, and challenges in definitive diagnosis.
From 1993 to 2018, the average development timeline for Alzheimer’s disease drug candidates—from patent application to either termination or approval—was approximately seven years. However, this figure dropped to 4.5 years between 2014 and 2018. This trend indicates that a growing number of pharmaceutical developers are losing confidence in the field, choosing to cut their losses and terminate R&D efforts before committing substantial resources.
In 2018, the early-stage development of Alzheimer’s disease pipelines was halted for the fourth time due to Pfizer’s termination of its neurology R&D portfolio. In 2017, major pharmaceutical companies also reprioritized their various drug pipelines. For example, AstraZeneca and Eli Lilly terminated their Phase II and Phase I Alzheimer’s disease programs, respectively.
In 2018, three drugs whose development in the Alzheimer’s disease pipeline was terminated gained widespread attention: pioglitazone, verubecestat, and azeliragon.
By 2019, some Alzheimer’s disease-related drug development programs were also halted. In January 2019, Genentech, a subsidiary of Roche, terminated two Phase III clinical trials of its monoclonal antibody crenezumab. In March 2019, Biogen suspended the development of aducanumab, a late-stage pipeline candidate.
Current R&D Pipeline for NAFLD/NASH
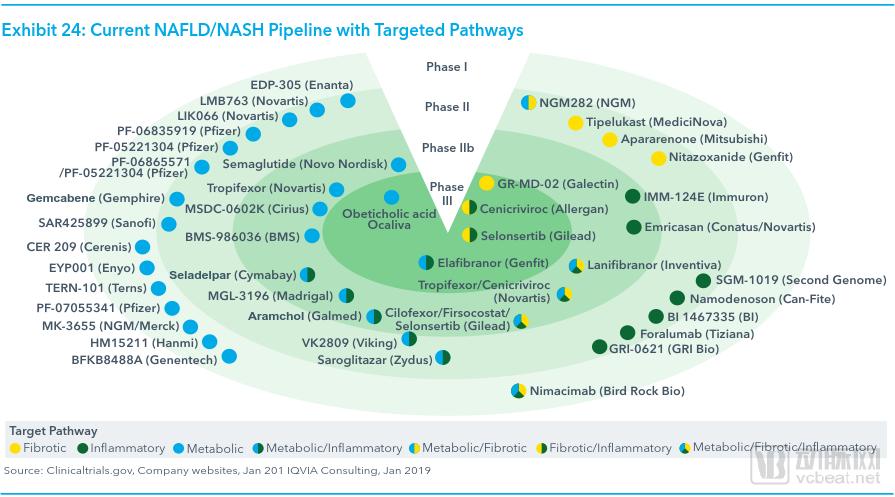
Non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) are complex, progressive conditions. Key hallmarks of these diseases include hepatic fat accumulation and fibrosis, which, if left untreated, can ultimately lead to liver failure or hepatocellular carcinoma. Current epidemiological studies indicate that nearly 42 million people in the United States have NAFLD, with approximately 20% affected by NASH.
The initial manifestation of this type of disease is NAFLD, characterized by hepatic steatosis without hepatocellular injury. As the disease progresses further, NAFLD will deteriorate into NASH.
The diagnosis of NAFLD or NASH relies on costly examinations such as imaging studies and liver biopsy; however, these tests are still subject to bias, making the diagnosis of NAFLD or NASH challenging.
Such diseases progress more commonly in patients with obesity or type 2 diabetes, and the global prevalence of these conditions continues to rise.
Currently, clinical trials in this drug pipeline lack any standardized primary endpoints, and there are no standardized care protocols. Physicians typically manage these conditions by prescribing generic medications such as pioglitazone.
Nine new drugs for NASH have entered late-stage development; these agents, with diverse mechanisms of action, hold promise for eventual market approval to meet
Unmet Treatment Needs in NAFLD/NASH. These novel drugs primarily target three distinct therapeutic areas: metabolic syndrome, fibrosis, and inflammation.
Early-stage pipelines are primarily focused on the treatment of metabolic syndrome, while late-stage pipelines are largely centered on fibrosis and
Treatment of inflammation. The results of these studies will determine the overall value of the investigational pipelines targeting these single mechanisms.
The R&D Pipeline for Neuromuscular Diseases at Different Stages
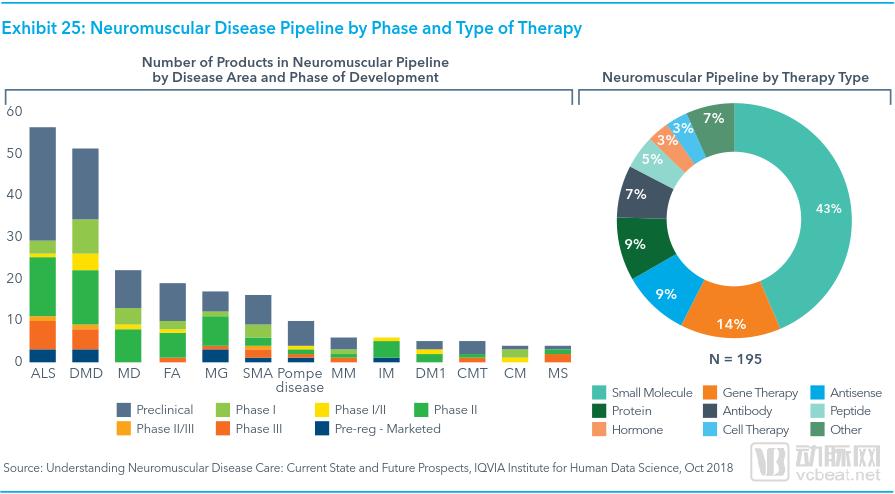
As understanding of the potential genetic factors and molecular pathways underlying neuromuscular diseases has deepened, an increasing number of drug targets have been identified, leading to a rapid surge in research and development activities in this field over the past five years.
As of April 2018, the number of drugs in Phase III clinical trials for the treatment of neuromuscular diseases increased fivefold, from nearly 20 in 2013 to almost 200. R&D activities were primarily focused on drug development for ALS (amyotrophic lateral sclerosis) and DMD (Duchenne muscular dystrophy).
As of April 2018, small-molecule drugs accounted for 43% of the pipeline for neuromuscular diseases, while gene therapies and antisense oligonucleotide therapies combined accounted for nearly one-quarter, at 23%.
In 2016, the FDA approved the first antisense oligonucleotide drug, eteplirsen (Exondys 51). Subsequently, the FDA approved the second antisense oligonucleotide drug, nusinersen (Spinraza), for the treatment of spinal muscular atrophy (SMA).
Currently, the ALS pipeline is primarily focused on targeted therapies for ALS subtypes, with gene therapy, neuroprotection, and drug development targeting neuroinflammation and oxidative stress pathways being the main research directions.
The most recently approved ALS drug is edaravone (Radicava), which was approved in 2017, marking a 22-year interval since the previous ALS drug approval. Edaravone is a small-molecule drug with antioxidant activity in the treatment of ALS, and studies have shown that it can moderately slow disease progression.