2019 Primary Healthcare Special Report: Structural Market Transformation and Eight Enterprise Development Models Across Three Segments
On May 14, 2019, VBInsight released the “2019 Report on Innovative Practices in Primary Healthcare》。Through field visits and surveys of primary healthcare institutions, VCBeat Research Institute has assessed the implementation progress of emerging medical technologies and new service models, as well as the extent to which grassroots needs are being met. By re-examining typical models and evaluating the development trajectory and pace of primary healthcare, this report aims to inspire further reflection and practical action among readers. The following is the content of the report.
The primary healthcare market is the main battlefield of China’s healthcare system, characterized by a large population base and extremely strong demand for medical services. Meanwhile, primary healthcare institutions suffer from weak service capabilities, poor infrastructure, and a lack of high-quality medical service supply. Due to various factors such as policy, technology, talent, and funding, there have been persistent challenges in effectively implementing initiatives to strengthen primary healthcare. As a result, many patients’ first choice when seeking care is to go directly to tertiary Grade A hospitals.
Policy-induced incentive distortions, insufficient capital investment, high staff turnover and difficulty in retention, lack of patient trust, and the powerful inertia generated by these factors all constitute formidable obstacles to the development of primary healthcare.
In 2017, we were delighted to discover that many obstacles that had long hindered the development of primary healthcare are dissolving, driven by the rapid advancement of internet technologies, continuous progress in smart hardware, revolutionary breakthroughs in intelligent algorithms and AI, and the sustained boom in biomedical technologies. Leveraging these multifaceted digital technologies, new business models have emerged and flourished. Together with the favorable momentum of policy reforms, these developments will significantly facilitate the two-way flow of high-quality medical resources. We refer to this process as “empowerment.”
Two years on, we revisit the primary healthcare market and find that the foundational environment for primary care has undergone tangible changes, with a marked improvement in the service capabilities of primary healthcare institutions; however, development progress varies across different sub-sectors.
Key Findings:
The advancement of community hospital construction will bring structural changes to primary care.
Among diagnostic and treatment cases that could not be definitively diagnosed, referrals due to lack of imaging capabilities accounted for 12.25%;
The primary departments involved in tiered diagnosis and treatment referrals initiated due to conditions exceeding the therapeutic capacity of primary healthcare institutions are mainly internal medicine, surgery, gynecology, orthopedics, and rehabilitation.
Primary Healthcare Investment and Financing Enter a Period of Mega-Deals, with Momentum Returning in 2018.
Structural Evolution of the Primary Healthcare Market
Primary healthcare institutions account for as much as 95% of China’s entire healthcare system, encompassing community health service centers (and stations), township (and sub-district) health centers, village clinics, and outpatient departments. With the gradual implementation of healthcare reform policies, there has been significant improvement in the scale, medical workforce size, and service capacity of primary healthcare in China. However, compared with tertiary hospitals, primary healthcare facilities still fall short in bed supply and equipment sophistication, and the imbalance between urban and rural development remains a prominent issue. Based on data published in the recently released China Health Statistics Yearbook 2018, we provide an overview of the current state of primary healthcare.
(1) Overall Institutional Landscape: Numerical Advantage with Pronounced Imbalances in Development

Data source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat.
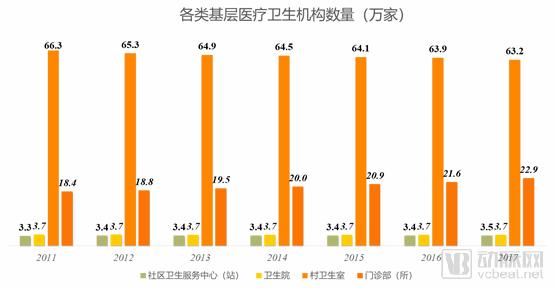
Rising Total Volume with Slowing Growth Rate: From 2011 to 2017, the number of primary healthcare institutions in China showed an overall upward trend, albeit at a relatively slow pace. Notably, in 2012, there was a significant decline in the number of these institutions, primarily driven by a reduction in village clinics. As urbanization accelerated, the rural population decreased year by year, leading to a corresponding decline in the number of village clinics.
Data Source: China Health Statistics Yearbook 2018, compiled by VCBeat.
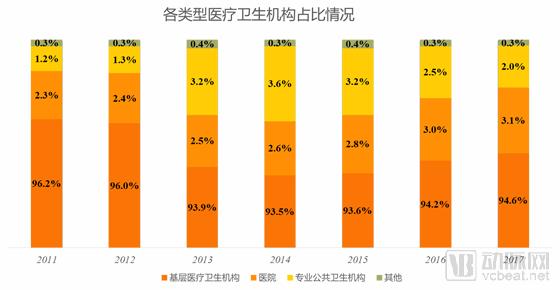
An Overwhelming Majority in Numbers: Primary healthcare institutions account for approximately 95% of the entire medical and health institution system, playing a vital role in the development of China’s healthcare sector. In contrast, hospitals, which contribute 78% of the total revenue of medical institutions in China, constitute only 3% by number.
Decline in Proportional Share: From 2011 to 2017, the proportion of primary healthcare institutions decreased by 1.6 percentage points. During the same period, the shares of hospitals and specialized public health institutions each increased by 0.8 percentage points. As a key pillar of China’s healthcare service system, hospital construction has maintained steady growth.
Data source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat
Leading Number of Village Clinics: Among all types of primary healthcare institutions in China, village clinics account for 70%, significantly outnumbering other facilities and ensuring the provision of medical services in rural areas.
Strong Growth Momentum in Outpatient Departments and Clinics: The number of outpatient departments and clinics has increased year by year, with an overall growth of 17% from 2011 to 2016, thanks to the relaxation of policy requirements for establishing clinics.
The number of township health centers remains stable: In recent years, the number of township health centers has remained stable at around 37,000, primarily because there have been no changes to China’s township administrative divisions.
Insufficient Development of Community Health Service Centers (Stations): China Needs to Strengthen the Network Construction of Community Health Service Centers (Stations) in the Later Stage to Better Meet the Medical Service Needs of Community Residents.
(2) Service Performance: Highest patient volume, with township health center revenue accounting for half of the total

Data Source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat Research Institute

Data source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat.
Highest share of patient visits, but sluggish growth: This is mainly because the quality of primary care services lags behind that of hospitals, leading to a lack of patient trust in primary care and a preference for seeking treatment at hospitals.
Mismatch Between Scale and Service Capacity: Primary healthcare institutions account for 95% of the total number but only 55% of patient visits; in contrast, hospitals, which make up merely 3% of the total number, handle as high as 41.2% of patient visits.

Data source: China Health Statistics Yearbook 2018, compiled by VCBeat
Total Volume Increases, Growth Rate Declines: The total revenue of primary healthcare has risen year by year, but its growth rate has dropped from 16.4% in 2011 to 6%. This is primarily due to the year-on-year decline in the growth rate of patient visits at primary healthcare institutions.
Township Health Centers Account for the Majority of Revenue: An analysis of annual revenues across various types of primary healthcare institutions shows that township health centers consistently contribute over 50% of the total. This predominance is primarily attributed to their superior medical equipment and service capabilities compared to other primary care providers, resulting in a higher volume of patient visits.
Data Source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat.
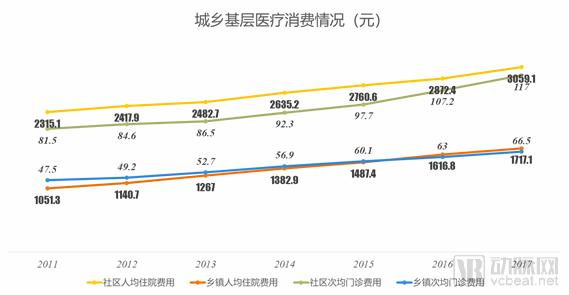
Residents' healthcare consumption expenditure has been increasing year by year: the per capita inpatient and outpatient costs in communities and townships continue to rise, indicating a steady annual growth in residents' healthcare spending.
Inpatient Costs Are the Primary Revenue Driver: Per Capita Inpatient Expenses in Community and Township Health Centers Far Exceed Outpatient Costs, Becoming the Main Source of Income for Primary Healthcare Institutions.
Significant Disparity in Grassroots Healthcare Consumption Between Urban and Rural Areas: Per Capita Inpatient and Outpatient Costs in Urban Communities Are Approximately Twice Those in Townships During the Same Period. This is primarily because urban residents have higher incomes and greater ability to pay for medical services; meanwhile, their healthcare consumption concepts are keeping pace with the times, making them more willing to increase spending on health and medical care.
(3) Bed and Equipment: Increased bed supply capacity, but insufficient equipment advancement

Data source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat.
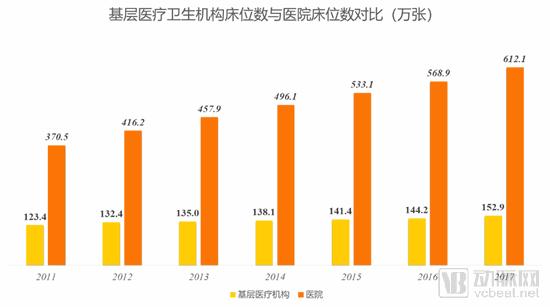
Expansion in Scale, Slowing Growth Rate: With strong government support for the development of primary healthcare, the number and scale of primary healthcare institutions have increased, leading to a greater supply of hospital beds. However, as the policy effects diminish, the growth in the number of primary healthcare institutions has slowed, resulting in a corresponding decline in the growth rate of bed capacity.
Data Source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat.
Bed counts are increasing: this indicates that both primary healthcare institutions and hospitals are continuously improving their medical service facilities.
Widening Gap in Total Capacity: The disparity in bed numbers between primary healthcare institutions and hospitals continues to expand, primarily due to the significant advantages hospitals hold in terms of fiscal support and financial strength. The government needs to further increase fiscal support for primary healthcare institutions, while these institutions must also continuously enhance their financing capabilities and further improve their service facilities.
Data source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat.
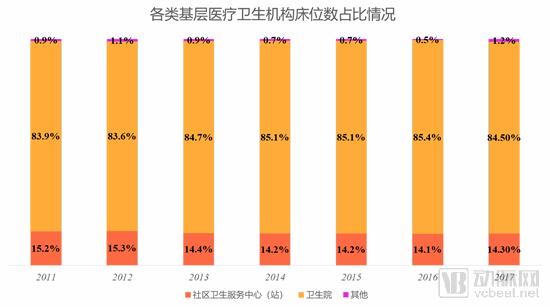
The proportion of hospital beds in township health centers is the highest and continues to expand year by year, while the proportion in community health service centers (stations) decreases annually. This is mainly due to the decentralization of medical services, with township health centers becoming the primary providers of inpatient care at the grassroots level.
Data source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat Research Institute
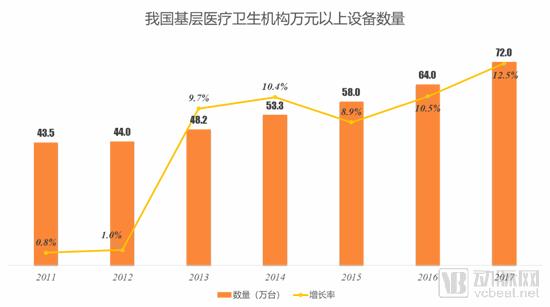
Hardware infrastructure is continuously improving and maintaining rapid growth: Primary healthcare institutions have intensified their equipment procurement efforts and accelerated the replacement and upgrading of devices, which helps enhance diagnostic and treatment capabilities. Notably, since 2013, the average annual growth rate in the number of medical devices valued at over RMB 10,000 has reached as high as 9.9%. This progress is attributable to increased government investment in primary healthcare equipment.
Data Source: China Health and Family Planning Statistical Yearbook 2018, compiled by VCBeat Research Institute
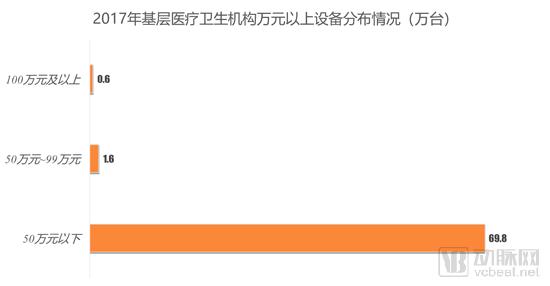
Insufficient Equipment Sophistication: Medical equipment in China’s primary healthcare institutions is predominantly priced below RMB 500,000, with very few units exceeding RMB 1 million. This indicates a low level of technological advancement, limiting capabilities to the diagnosis and treatment of basic diseases. There is an urgent need to introduce more advanced and higher-quality medical equipment.
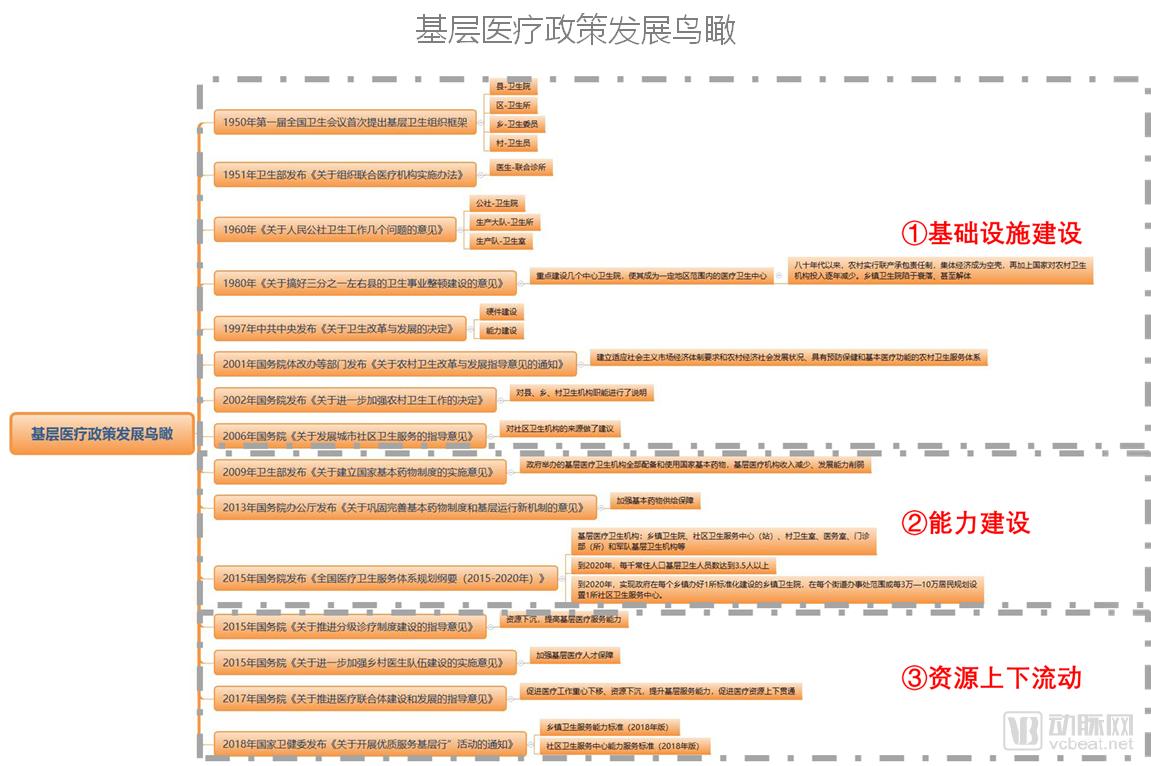
We examine the core driver behind the development of the primary healthcare market: policy. By reviewing the evolution of China’s primary healthcare policies since the founding of the People’s Republic, we observe that policy reforms are entering a more complex and critical phase. The overarching theme has consistently centered on building and optimizing primary healthcare capabilities. Over the past decade, the “tiered diagnosis and treatment” system, which facilitates patient flow between different levels of care, has emerged as the most substantive and far-reaching policy initiative.
Source: VCBeat Eggshell Research Institute
From 1949 to 2008, we define this period as the phase of infrastructure development for primary healthcare. From 2009 to 2014, we observed that major policies were primarily focused on enhancing the capacity of primary healthcare institutions. Since 2015, a series of detailed interpretations have been proposed around the tiered diagnosis and treatment system, aiming to facilitate the downward flow of high-quality medical resources, achieve resource sharing, and improve the lagging development of primary healthcare.
There are disparities in the levels of regional, urban, and rural economic development in China. The inherent scarcity of high-quality medical resources at the grassroots level in rural areas has led to pronounced imbalances in the development of primary healthcare. To achieve the healthcare reform goal of equalizing access to basic medical services, it is essential to redistribute medical resources and increase support for grassroots-level institutions.
In recent years, the Chinese government has actively advanced various policy initiatives centered on “tiered diagnosis and treatment.” Tiered diagnosis and treatment refers to the classification of diseases based on their severity and urgency, as well as the complexity of required care, with medical institutions at different levels assuming responsibility for treating corresponding conditions. This tiered model, spanning from general practice screening to specialized treatment, aims to achieve initial consultations at primary care facilities, bidirectional referrals, differentiated management of acute and chronic conditions, and coordinated care between upper- and lower-level institutions. Ultimately, it seeks to establish an ideal healthcare delivery pattern in which minor ailments are managed within communities, serious conditions are treated at hospitals, and rehabilitation takes place back in the community.
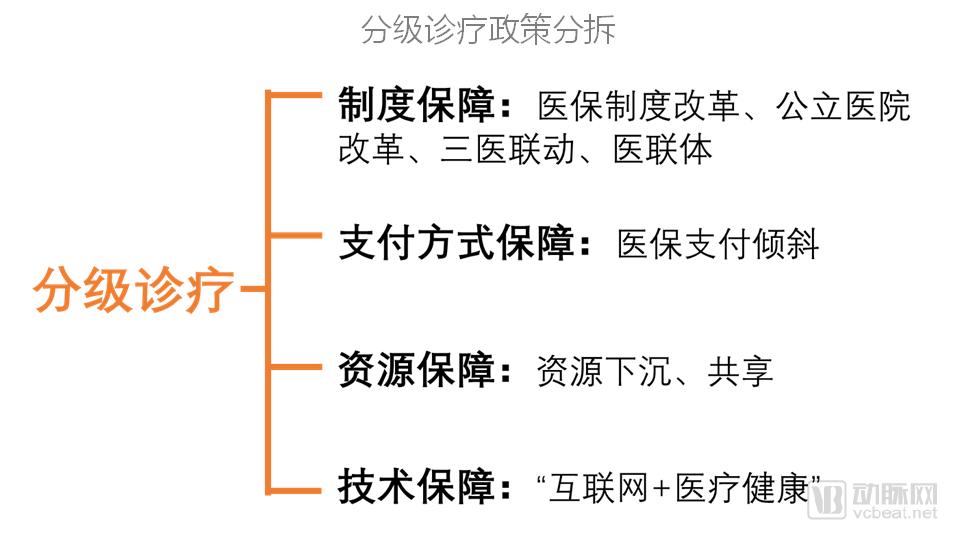
Establishing a tiered diagnosis and treatment system is a complex systemic engineering project, characterized by broad scope and intricate circumstances, necessitating a long-term process. Our analysis of the tiered diagnosis and treatment policy will be grounded in institutional safeguards, payment mechanism guarantees, resource allocation assurances, and technological support, thereby elucidating the policy’s composition and implementation roadmap.
Source: VCBeat Research Institute

Data Source: Public Information, VCBeat
In 2009, China first proposed the concept of “tiered diagnosis and treatment.” From 2010 to 2012, top-level designs such as the National 12th Five-Year Plan were frequently introduced, leading to a substantial increase in policies related to tiered diagnosis and treatment.
In 2015, “tiered diagnosis and treatment” was elevated to the institutional level, leading to an explosive growth in policies related to “tiered diagnosis and treatment.”
In 2016, the number of relevant policies at the national level decreased, while those related to “tiered diagnosis and treatment” increased at the provincial level.
From 2017 to 2018, with the introduction of medical insurance payment policies and relevant plans under the “13th Five-Year Plan,” policies on tiered diagnosis and treatment gradually increased.
In 2019, Document No. 4 issued by the General Office of the State Council incorporated “tiered diagnosis and treatment” into the performance evaluation framework for public hospitals, while Document No. 8 from the State Council proposed enhancing the service quality of tiered diagnosis and treatment and allocating all newly increased fiscal subsidies for basic public health services exclusively to villages and communities. With the introduction of these policies, “tiered diagnosis and treatment” is poised to become a centerpiece of healthcare reform, serving as a crucial mechanism for controlling health insurance expenditures and optimizing the allocation of medical resources.
Through a four-pronged analysis of the “tiered diagnosis and treatment” policy theme—covering institutional, payment, resource, and technical safeguards—we found that policy implementation accelerated significantly after 2015. Policies related to resource and technical safeguards were progressively refined, with local governments actively following suit. Under the guidance of these policies, various provinces have successively issued implementation plans for tiered diagnosis and treatment systems.
On March 15, 2019, the Department of Primary Health Care issued the “Notice of the General Office of the National Health Commission on Launching Pilot Programs for Community Hospital Construction,” proposing that, to implement the spirit of the 19th National Congress of the Communist Party of China and the strategic deployment of the Healthy China Initiative, and to meet the public’s demand for basic medical and health services, pilot programs for community hospital construction should be launched in selected regions with the necessary conditions.
The current pilot regions include the following 20 provinces, municipalities, and autonomous regions: Hebei Province, Shanxi Province, Inner Mongolia Autonomous Region, Heilongjiang Province, Jiangsu Province, Anhui Province, Jiangxi Province, Shandong Province, Henan Province, Hubei Province, Hunan Province, Guangdong Province, Guangxi Zhuang Autonomous Region, Hainan Province, Chongqing Municipality, Sichuan Province, Yunnan Province, Shaanxi Province, Gansu Province, and Qinghai Province.
Promoting pilot programs for the development of community hospitals helps to reasonably expand the service capabilities of primary healthcare, enhances the influence and social standing of primary healthcare institutions, boosts the professional confidence and sense of belonging among grassroots health workers, and increases residents’ trust in and utilization of primary healthcare facilities.
As pilot primary healthcare institutions, community hospitals are constructed in accordance with established development tasks. Upon passing evaluation by the provincial health administrative department, they are authorized to operate under the “Community Hospital” designation. After receiving this designation, community hospitals may perform Level 1 and Level 2 surgeries; those evaluated as meeting the standards of secondary-level hospitals may also perform Level 3 and lower-level surgeries.
Community hospitals performing surgical procedures shall establish operating rooms and anesthesiology departments; pathological diagnosis services may be provided by third-party institutions or higher-level medical institutions within the medical consortium. After being designated as a “community hospital,” the operational nature of the facility shall remain unchanged, and existing levels of fiscal compensation and preferential policies shall not be reduced or diminished.
The current pilot program for community hospitals features extensive coverage and rapid implementation. As May began, detailed policies from the pilot provinces have been rolled out successively. More importantly, by applying to become a pilot community hospital, existing medical institutions can expand their diagnostic and treatment services, equip themselves with medical devices that meet operational needs, and offer a comprehensive range of pharmaceutical products. By enhancing their medical service capabilities to achieve an upgrade to secondary hospital status, these institutions will gain developmental support through medical service pricing and health insurance reimbursement mechanisms. This represents a significant opportunity for the rapid improvement of primary care delivery capabilities.
In the 8 trillion yuan health industry market, the primary decision-making power lies in the medical services sector. Prescription authority determines the flow of pharmaceuticals, manufacturer budgets, national health insurance payments, and commercial insurance funds. The baton guiding this industry will increasingly shift toward community-level care in the future. In China, 80% of national health insurance expenditures are also expected to be allocated to community healthcare, bringing with them greater commercial opportunities.
Demand Classification: Reanalyzing the Empowerment of Primary Healthcare Models
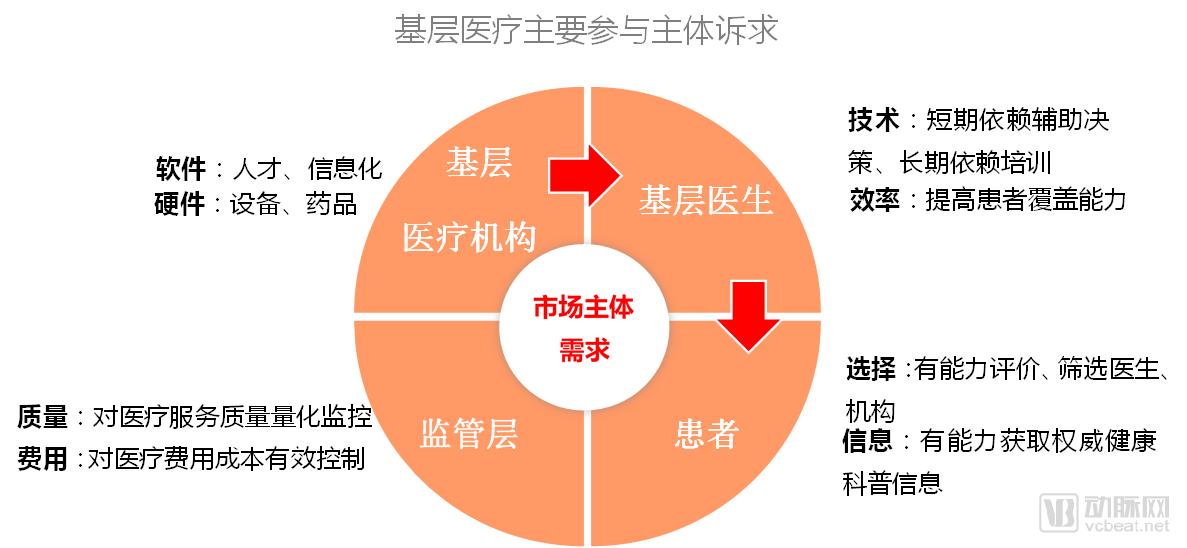
The primary care market can be mainly divided into four key stakeholders: regulatory authorities, primary care institutions, primary care physicians, and patients. Here, we categorize and summarize the needs of these four groups based on their healthcare demands.
Source: VCBeat
In summary, the pain points and urgent issues faced by grassroots participants mainly fall into three categories:
Infrastructure issues, including laboratory testing and pharmaceuticals, to ensure that patients at the primary care level can access diagnostic tests and treatment for minor illnesses.
Efficiency issues primarily refer to freeing them from existing tedious and repetitive tasks.
Addressing the Enhancement of Diagnostic and Treatment Capabilities: Strengthening the Service Capacity of Primary Care Physicians, Gradually Building Trust, Expanding Service Offerings, and Achieving a Virtuous Cycle of Concurrent Growth in Physician Income and Service Quality.
Addressing the Three Types of Needs of Grassroots Participants Through a Multi-Dimensional, Bottom-Up Approach Encompassing Peripheral and Grassroots Levels. For instance, to enable community residents to access high-quality medical service resources, a regional healthcare information platform has been established to achieve interconnectivity, information sharing, and regional collaboration among hospitals, community health information service centers, and healthcare administrative departments. Additionally, a series of medical skills training tools have been developed to enhance the competencies of grassroots physicians, allowing them to conduct training anytime and anywhere for rapid improvement in technical proficiency. Furthermore, internet-based tools have been introduced from the patient’s perspective to assist patients in self-managing their diseases.
Source: VCBeat Eggshell Research Institute
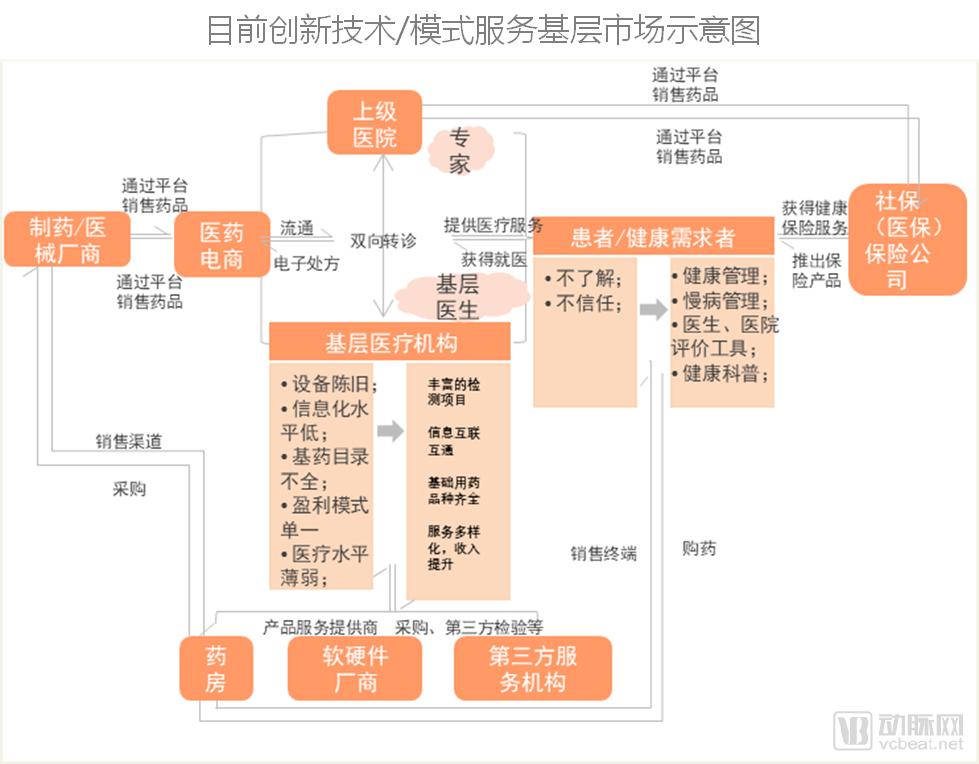
We have matched the three categories of issues urgently needing resolution at the primary care level with the currently visible directions for innovation in primary healthcare:
Addressing Primary Care Infrastructure Issues
Diagnosis: Implement the "primary-level testing, senior-level diagnosis" model to enhance accessibility and overall efficiency. Adopt an integrated service model combining equipment, systems, and expert services to provide unified testing and diagnostic solutions.
Rehabilitation Equipment: The drivers that spurred significant growth in rehabilitation medicine in the United States at the end of the last century—such as population aging, reforms in health insurance payment models, and technological advancements—are now unfolding in China. It is estimated that the domestic rehabilitation medical market will reach a scale of hundreds of billions of yuan.
Addressing the Complexity of Grassroots Work
Informatization: Affordable information systems (EHR, HIS, SaaS), electronic health records (EHR), and participation in health information exchange (HIE) between hospitals and external medical institutions to ensure optimal care pathways and enhance nursing capabilities and efficiency. Internal functionalities include electronic prescription and medical record management, pharmaceutical inventory management, member/patient management, medical knowledge bases, and integration with third-party laboratory services.
Efficiency Enhancement/Chronic Disease Management: “Hardware and Software + Services + Primary Healthcare Institutions.” The profit model primarily leverages established doctor-patient relationships to drive the conversion and purchase of capitated bundled services.
Capacity Enhancement and Expansion of Service Offerings
Skills Enhancement: Improve medical skills through platforms such as clinical decision support tools, remote training, and video-based instruction.
Imaging + Artificial Intelligence: Through deep learning, artificial intelligence can rapidly and accurately interpret and recognize medical images.
CDSS: A Digital Solution to Effectively Enhance the Standardization of Clinical Practice in Primary Healthcare
Following in the Footsteps: Exploring Development Pathways for Grassroots Markets
To gain a genuine understanding of primary healthcare, we obtained graded diagnosis and treatment business data from Peach Internet Hospital, a builder of medical consortiums that has deeply cultivated the primary healthcare market and served over 10,000 small and micro medical institutions. Through a brief analysis of its operational data, we aim to identify certain patterns in the operation of primary healthcare.
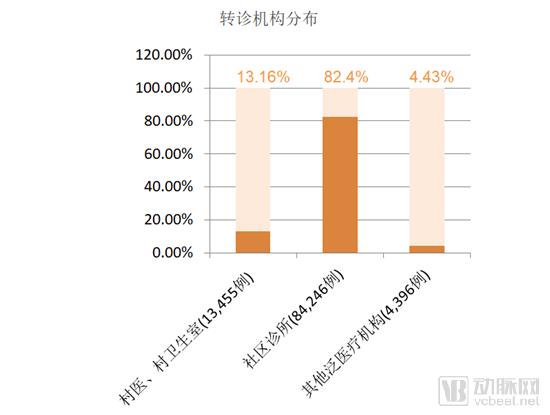
Data from the Taozi Internet Medical Consortium Platform between September 2018 and April 2019 show that the platform facilitated over 100,000 tiered diagnosis and treatment interactions. Taking primary healthcare institutions in third-, fourth-, and fifth-tier cities as an example, a total of 68,688 tiered diagnosis and treatment referrals were initiated. Among these, village clinics, community health stations, and village doctors initiated 9,040 referrals, accounting for 13.16% of the total; 3,048 patients were referred for in-person treatment following online consultations with other pan-medical institutions, representing 4.43% of the total referral volume; and community clinics handled 56,600 referrals, comprising 82.4% of the total. Of the referrals from community clinics, 48,232 were for outpatient treatment and 20,456 for inpatient care, accounting for 70.2% and 29.8%, respectively.
Data Source: Taozi Internet Hospital, VCBeat Eggshell Research Institute
There were 33,552 instances of undiagnosed conditions at primary healthcare institutions due to the lack of biochemical testing and medical imaging diagnostics (ECG, radiology, and ultrasound). Among these, 4,112 referrals (12.25%) were generated due to insufficient imaging capabilities, while 29,440 referrals (87.74%) resulted from the lack of biochemical testing capacity. Additionally, tiered diagnosis and treatment referrals initiated because cases exceeded the treatment capacity of primary healthcare institutions included 22,976 in internal medicine, 8,520 in surgery, 2,696 in gynecology, 2,456 in orthopedics, and 6,576 in rehabilitation.

Data Source: Taozi Internet Hospital, VCBeat Research Institute
Influenced by the traditional healthcare-seeking behavior of Chinese residents, who tend to avoid medical consultations during the Lunar New Year, patient visits at most primary care institutions dropped significantly during and around the Spring Festival. Some hospitals chose to adjust staff on-duty schedules or even temporarily close for holidays. Under these circumstances, during the Spring Festival in February 2019, partner institutions of the Taozi Internet Medical Consortium provided a total of 1,141 referral services to the public through a convenient tiered diagnosis and treatment system.

Data Source: Taozi Internet Hospital, VCBeat Eggshell Research Institute
The fundamental issue facing primary healthcare institutions is weak infrastructure. Solutions such as point-of-care testing (POCT) devices, rehabilitation equipment, third-party services, telemedicine, and pharmaceutical solutions can effectively enhance these institutions’ service capabilities, enabling them to increase profitability while reducing costs, thereby improving the level of infrastructure development at the primary care level.
Efficiency empowerment addresses the issue where energy and time are insufficient to cover the existing patient population. We consider this a subsequent step; however, we observe that primary care physician systems and chronic disease management systems, derived from health information technology platforms, are currently freeing primary healthcare practitioners from cumbersome daily tasks.
By helping primary healthcare institutions resolve the aforementioned two issues, economies of scale will naturally emerge, enabling gradual changes in patient awareness and habits through efficient patient outreach, education, and guidance. Mobile smart devices and big data analytics will serve as the core value drivers for patient empowerment, with physician evaluation tools and chronic disease management representing the models with the greatest development potential in the future.
The above highlights key excerpts from the report, which also provides a detailed analysis of the development pathways for three market segments—primary-care pharmaceuticals, primary-care diagnostics, and primary-care healthcare IT—as well as the business models of seven major companies: Akang Health, Shanghai Pharmaceuticals Cloud Health, KuaiYiJian, Yizhan Medical Group, Comper, Dingxiang Cloud Manager, and Xinyi International. The following is the entireReport Structure:
I. Structural Evolution of the Primary Healthcare Market
1.1 Overview of the Primary Healthcare Market: A Structural Shift Is Underway
1.1.1 Overall Institutional Landscape: Numerical Advantage Coupled with Pronounced Imbalances in Development
1.1.2 Service Performance: Highest Patient Volume, with Health Center Revenue Accounting for Half of the Total
1.1.3 Bed and Equipment: Increased bed supply capacity, but insufficient equipment advancement
1.2 Further Enhancing Primary Care Service Capacity: The Call for Community Hospital Construction Has Sounded
II. Demand Classification: Reanalyzing the Empowerment of Primary Healthcare Models
2.1 Classification of Primary Care Needs
2.2 Revisiting the Empowerment of Primary Healthcare Models
III. Following in Their Footsteps: Exploring Development Pathways for the Primary Healthcare Market
3.1 Analysis of Primary Healthcare Services and Market Supply “Positioning”
3.2 Primary Healthcare and Pharmaceuticals
3.2.1 The shortage of medical personnel and medicines in primary healthcare institutions is being alleviated
3.2.2 Expansion of the 2018 Edition of the National Essential Medicines List
3.2.3 Aikang Health: Integrated Rural Prescription Drug Services
3.2.4 Shanghai Pharma Cloud Health: Urban Community DTP Pharmacies
3.3 Primary Care Laboratory Testing
3.3.1 92% of Village Clinics and Medical Practices Lack Laboratory Testing Capabilities
3.3.2 Rapid Rise and Volume Growth of Third-Party Laboratory Service Providers
3.3.3 KuaiYiJian
3.3.4 Yizhan Medical Group
3.3.5 Comper
3.4 Informatization of Primary Healthcare
3.4.1 Current Challenges
3.4.2 Two Innovative Models
3.4.3 Dingxiang Cloud Manager
3.4.4 Heart Medical International
IV. Investment and Financing Conditions of Enterprises in the Primary Healthcare Market
4.1 Sustained Momentum: Financing Amounts Continue to Rise
4.2 Chain Clinics Emerge as a New Force, with Momentum Returning in 2018
Click here to get the full version of 《2019 Report on Innovative Practices in Primary Healthcare》。
Note:
Definition of the Primary Healthcare Market: In our previous studies, the primary healthcare market was examined as a broad market segment. In this report, based on documents issued by relevant national ministries and commissions and our understanding of the primary healthcare sector, we define the primary healthcare market as the industrial aggregation of medical and health services delivered within primary healthcare institutions. These institutions primarily include community health service centers (and stations), township health centers (and village clinics), as well as various types of clinics and pharmacies.