30 Cities to Pilot DRG Payment Reform: In-Depth Analysis of Hospital Management Model Transformation
On May 20, the National Healthcare Security Administration (hereinafter referred to as the “NHSA”) held a video conference to launch the national pilot program for Diagnosis-Related Groups (DRG)-based payment, marking the official commencement of nationwide exploration into DRG payment reform. Fourteen days later, on June 5, the NHSA, in conjunction with four other departments, issued the “Notice on Printing and Distributing the List of Cities Selected for the National Pilot Program on Diagnosis-Related Groups (DRG)-Based Payment” (hereinafter referred to as the “Notice”). The Notice outlined clear pathways for implementing reform measures in the 30 pilot cities mentioned.
The “Notice” first outlines the reform framework, requiring pilot cities and their respective provinces to follow the three-step approach of “top-level design, simulation testing, and actual payment” to ensure task completion. It specifies that 2020 would serve as the simulation period, while 2021 would mark the commencement of actual payments. In the face of the impending DRG-based payment reform, what impacts and challenges will hospitals encounter? What changes in management models and preparatory measures are needed in advance to adapt to this shift in the rules of the game? This article will delve into these questions.
I. Challenges Posed by DRG-Based Payment to Hospitals
For a long time, China’s healthcare payment system has been predominantly based on fee-for-service (FFS). Under the incentives of this payment model, hospitals have become accustomed to a management paradigm that treats each individual service item as a revenue source. This situation has been exacerbated by a distorted pricing structure in which medical service fees have been significantly undervalued, while prices for pharmaceuticals, consumables, and diagnostic tests have been substantially overvalued. Consequently, under this payment system, pharmaceuticals, consumables, and diagnostic services have become the primary revenue streams for hospitals. Physicians are thus motivated to increase hospital income by prescribing more medications and consumables, as well as ordering more diagnostic tests. Under such a payment framework, hospital management remains extensive rather than refined. Revenue growth driven by the accumulation of service items constitutes the core operational and management model, while cost control and refined management practices remain weak.
DRG-based payment is essentially a bundled, fixed-amount reimbursement model organized by diagnosis-related groups. With the adoption of a DRG-based payment system, hospitals’ revenue structures will undergo significant changes. The traditional hospital management model, which relied on fee-for-service as its primary revenue source, will shift to a bundled, fixed-payment approach based on diagnosis-related groups. Each DRG group will become a standardized product for the hospital. For example, an appendectomy may be bundled at a fixed price of RMB 6,000. All associated inputs—including diagnostic tests, laboratory examinations, medications, and consumables—will no longer constitute revenue sources for the hospital; instead, they will be treated as cost components incurred in successfully treating appendicitis within the predetermined total payment of RMB 6,000. This will fundamentally change the previous rules of the game: items such as medications, consumables, and diagnostic or laboratory tests will no longer serve as revenue generators. Physicians will no longer have incentives to order excessive services; rather, they will focus on achieving positive clinical outcomes while implementing rational cost control measures.
The payment system built on Diagnosis-Related Groups (DRGs) helps establish a positive incentive mechanism that changes the behavior of healthcare providers, thereby altering hospitals’ revenue strategies. Health insurance agencies have become the overall controllers of medical costs and agents for patients, which to some extent curbs supplier-induced demand and encourages hospitals to minimize patients’ length of stay.
However, this shift in payment methods poses significant challenges for hospitals that have long been accustomed to the fee-for-service operational model, as it necessitates a fundamental transformation of their management and operational frameworks. If hospitals fail to promptly adapt to an operational model centered on refined cost control with diagnosis-related groups (DRGs) as the product unit, they risk facing a scenario where increased patient volume leads to greater financial losses.
Consequently, the implementation of this payment system forced a segment of healthcare institutions, unable to proactively adapt to the framework, to withdraw from industry competition. Between 1987 and 1994, 454 hospitals closed in the United States, resulting in the loss of 22,000 acute-care beds. As financial liability risks for hospitals intensified, corresponding changes became imperative in physicians’ clinical practices and hospital management models.
However, the DRG payment system also incentivizes hospitals to proactively reduce costs to maximize profits, encouraging them to prioritize cost-effectiveness in the procurement of pharmaceuticals, medical supplies, and equipment, as well as in the utilization of medical resources and clinical practice. By leveraging DRG data analysis, hospitals can compare various treatment protocols to identify clinical pathways that are effective, efficient, and economical, thereby achieving low-cost, high-efficiency care. Under this guidance, hospitals can curb unreasonable growth in medical expenditures by reducing average length of stay and minimizing inducement-driven healthcare consumption among patients.
Studies have shown that after Germany implemented the DRG payment system, the average length of stay in 750 pilot hospitals decreased by 30%. Meanwhile, a large number of private hospitals in Germany have thrived due to their competitive advantages, giving rise to large private hospital groups such as HELIOS and Asklepios.
Therefore, the reform of the Diagnosis-Related Group (DRG) payment system presents both challenges and opportunities for hospitals. If hospitals can rapidly transform their operational philosophy and establish strategic goals centered on efficient, cost-controlled operations during the implementation of DRG payment reforms, they are likely to achieve accelerated growth and build more core competitive advantages in the new round of competition.
II. Hospitals should proactively transform their operational and management models, turning the challenges of DRG-based payment into new development opportunities
DRG-based payment, which reimburses according to pre-established DRG payment standards, will compel healthcare providers (hospitals) to shift their profit-generation strategy from increasing service volume to controlling costs. Healthcare institutions and physicians can achieve surpluses and generate revenue only by reasonably controlling costs and improving service efficiency. Pharmaceuticals, medical consumables, and diagnostic tests have transitioned from revenue sources to cost items; therefore, rational resource utilization is essential for efficient operations.
To adapt to the challenges posed by DRG-based payment, healthcare institutions must transform their operational and management models through cost control, process reengineering, adjustments in staffing and capital allocation (including campuses, departments, equipment, and beds), enhancement of diagnostic and treatment capabilities, and optimization of clinical pathways, so as to ensure financial balance. This will help establish a positive incentive mechanism from within, encouraging hospitals and physicians to proactively modify their medical practices, independently manage costs, and achieve the goal of reasonable cost containment.
Following the implementation of DRG-based payment, hospital operational management will shift to a model focused on managing profitability and loss by diagnosis-related groups, as illustrated in the figure below:
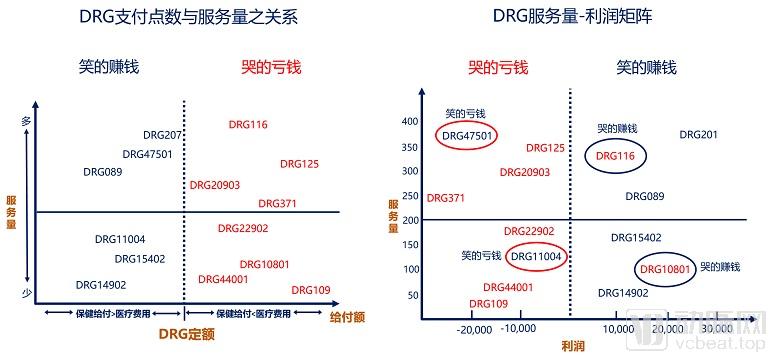
Figure 1. Post-DRG Payment Implementation in Taiwan: Hospital Operational Management Shifts to a Model Based on Diagnosis-Related Group Profitability and Loss
A DRG expert from Taiwan Province of China stated in a speech at an academic forum that, after the implementation of DRG-based payment, hospital management in Taiwan has shifted to focus primarily on the profitability of disease groups. Taking DRG group 47501 as an example, a fee-based analysis shows that “healthcare benefits exceed medical expenses”; however, when costs are taken into account, the group incurs a loss of NT$20,000. Therefore, under DRG-based payment, hospitals need to place greater emphasis on cost accounting for disease groups and adopt a management mindset centered on group-level profitability and loss control. By continuously adjusting actual hospital costs to ensure that “payment standards > standard costs > actual costs,” hospitals can achieve an optimal operational model.

Figure 2: Hospital Operational Management Shifts to DRG-Based Cost Data-Driven Operations
In addition to China, some European countries, such as Germany, have further strengthened their cost accounting management systems after implementing the G-DRG payment model by establishing a bottom-up cost accounting approach. Specifically, they first allocate indirect cost centers to direct cost centers, and then perform a bottom-up allocation based on the actual volume of services provided during patient treatment. This process determines the actual cost for each type of medical service per patient, which is then aggregated to generate a disease group cost matrix. This matrix supports refined internal hospital management by enabling detailed cost analysis for each DRG group, thereby achieving the goal of precision management.

Figure 3 Example of the DRG Cost Matrix in Germany
Hospitals can better address the challenges and disruptions posed by DRG-based payment through structural adjustments. Taking Germany as an example, following the implementation of G-DRG payment reform, hospital management structures underwent the following changes:
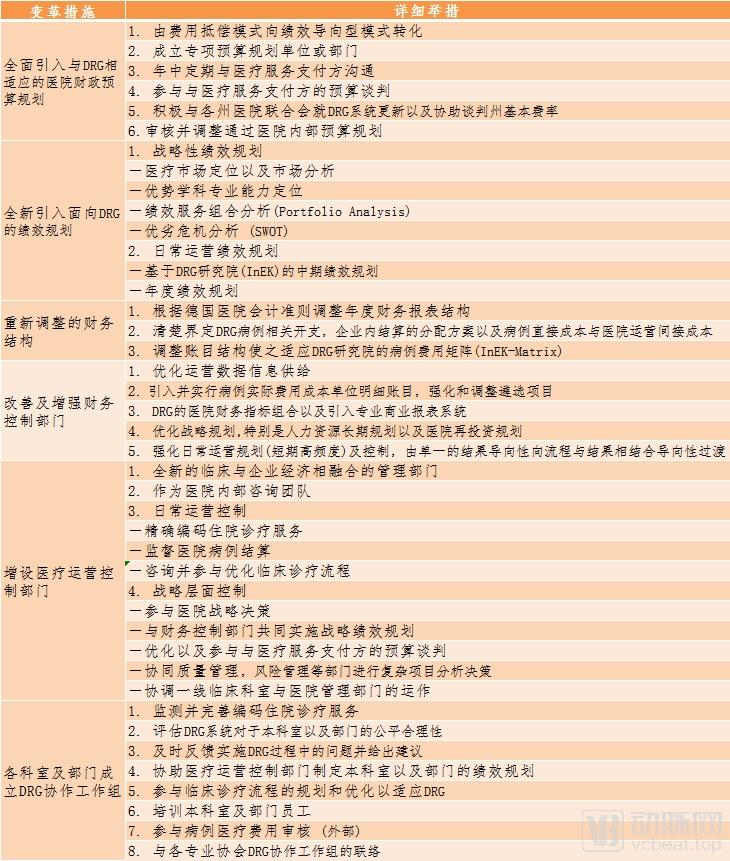
Table 1 Changes in Hospital Management Structure Following the Implementation of G-DRG in Germany
From a long-term development perspective, hospitals should also re-evaluate and formulate their overall strategic goals in light of their own competitive advantages. Large hospitals tend to focus on complex and critical cases (with higher Case Mix Index, CMI) that can drive revenue growth, thereby prioritizing the development of specialized medicine and the research and development of new technologies as their main strategic objectives. In contrast, small and medium-sized medical institutions often transition into rehabilitation or traditional Chinese medicine hospitals, or form medical consortiums with large hospitals to take on outpatient services and rehabilitation patients referred by these larger institutions.
Hospitals also need to re-examine and reshape collaborative relationships within their ecosystem, restructuring the benefit distribution across the ecological chain around a cost-centric management model, as illustrated in the figure below:
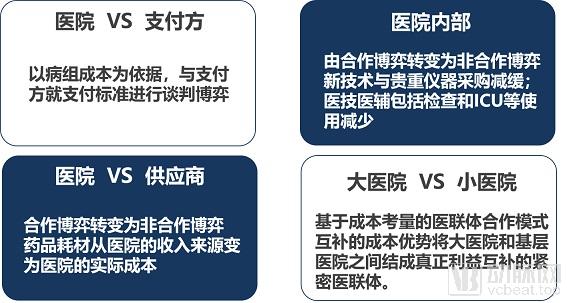
Figure 4: Cost-Centric Management Model Will Reshape the Benefit Landscape of the Hospital Ecosystem
In a sense, this facilitates the evolution of China’s medical institutions toward the Medical Consortium model. Taking the United States as an example: the U.S. Integrated Delivery System (IDS), which is similar to the Medical Consortium, comprises various healthcare institutions that assume comprehensive medical and financial responsibilities for delivering long-term, holistic care to a relatively defined population, thereby aiming to improve healthcare quality and optimize costs.

Figure 5. Integrated Healthcare Delivery Systems in the United States: Enhancing Quality of Care and Optimizing Healthcare Costs
Columnist: Dr. Liu Zhichen, a senior DRG expert and postdoctoral fellow in Public Administration at Fudan University

Professional Profile: Chief Expert in the Healthcare Sector, Industrial Internet Product Center, China Unicom Group. Postdoctoral Fellow at the Postdoctoral Mobile Station of Public Administration, Fudan University, and the Postdoctoral Workstation of the Statistical Information Center, National Health and Family Planning Commission. Senior Strategic Expert in the Big Health sector. With nearly a decade of strategic consulting experience in internet healthcare and the broader health industry, previously served as Director of Strategic Consulting and R&D Business Development at a listed domestic IT solutions and services provider. Spearheaded the planning of numerous forward-looking innovative business models for the Big Health sector. Presciently predicted that healthcare payment reforms in China, particularly the adoption of Diagnosis-Related Groups (DRG)-based payment systems, would become a key initiative in deepening healthcare reform during the 13th Five-Year Plan period. As the overall project lead, participated in a pilot project for DRG-based medical insurance payment reform at the prefectural level in China. Assisted the municipal Medical Insurance Bureau in designing the top-level framework for citywide DRG payment system reform and implemented the supporting information technology infrastructure.
References:
1. Wang Qian. Specific Application of DRG in German Hospitals [R]. Speech delivered at the Second National DRGs Forum, July 2017
2. Wang Liuming, Lang Wen, Tao Hongbing. Advantages and Disadvantages of the German Diagnosis-Related Groups Payment System and Its Implications [J]. Medicine and Society, 2013(11):45
3. Huang Jin’an. Activity-Based Costing and DRG Performance Management: A Feasibility Assessment of Implementing Activity-Based Costing [R]. Speech delivered at the 1st National Diagnosis-Related Group (DRG) Forum, December 2016.
Copyright Notice:
Most of the viewpoints presented in this article are based on the postdoctoral research findings of Dr. Liu Zhichen. The cited articles and viewpoints reflect those of their respective authors, obtained from publicly available sources. Unauthorized reproduction, excerpting, copying, mirroring, or any other form of use is strictly prohibited.