Has Internet Healthcare Emerged from Its Wild West Era and Caught the Tailwind of National医保 Coverage?
By Li Yanyu, Luo Mei
Perhaps the most disheartening aspect is the absence of a strategic blueprint that commands the unanimous agreement and trust of all reformers. They possess abundant historical data and are accustomed to relying on solid evidence to build consensus for action. However, due to the lack of data concerning the future, there is no compelling guide to indicate which paths lead to dead ends and which offer promising avenues for reform. Few people truly understand the interconnections among these different pathways.
——Christensen
"The Original Intent" of Internet Healthcare
In 2006, Li Tiantian abandoned his doctoral studies and, at the invitation of two friends, moved to Hangzhou. As a native Northeasterner, he settled down by the West Lake, bringing with him two DXY.cn servers packed in his luggage.
In the same year, after experiencing two internet startup ventures—3721 and Qihoo, co-founded with his middle school classmate Zhou Hongyi—Wang Hang established Haodf Online. This decision was driven by two factors: first, his medical background; and second, a series of unpleasant healthcare experiences following the birth of his son two years earlier, which inspired him, as a medically trained professional, to leverage the internet to transform healthcare.
Also in 2006, Liao Jieyuan founded China Greenline Co., Ltd. Prior to this, he had developed the first intelligent voice computer, “Tianyin Generation I.” Four years later, prompted by his family’s difficult experience seeking medical care, Liao led his team to pivot from the telecommunications industry into healthcare, establishing Guahaowang (the predecessor of WeDoctor).
In the same year that Guahao.com was founded, Zhang Rui, who harbored a certain “indignation” toward the news industry, left NetEase to establish Chunyu Doctor, transforming himself into an iconic entrepreneur in the internet healthcare sector. In later assessments of his legacy, he was invariably described with labels such as “passionate” and “free-spirited.”
In 2014, after the National Health and Family Planning Commission (the predecessor of the National Health Commission) officially introduced the term “telemedicine,” internet healthcare experienced an explosive growth that year.
Anyone in the industry mentioning internet healthcare will frequently recall the dialogue in late 2015 between Zhang Rui, founder and former CEO of Chunyu Yisheng (Spring Rain Doctor), and Wang Shan, President of Peking University People’s Hospital. Zhang represented internet healthcare entrepreneurs riding the wave of a booming trend, while Wang represented traditional healthcare, which held a monopolistic position. That dialogue, interrupted 18 times by both parties, was described later by Zhang Kun as epitomizing the sentiment that “the internet seeks to transform healthcare, but healthcare does not accept the internet.”
In reality, internet healthcare enterprises differ from brick-and-mortar hospitals across every stage of the care continuum. Brick-and-mortar hospitals primarily assume a disease-centric role throughout the diagnosis and treatment process, focusing on delivering diagnostic results and formulating treatment plans. In contrast, due to policy and environmental constraints, internet healthcare can only leverage its technological advantages in specific areas such as triage, appointment registration, health consultations, post-treatment follow-ups, and chronic disease management. Internet healthcare and brick-and-mortar hospitals constitute two entirely distinct systems in terms of physician resources, service delivery models, focal points, and payment mechanisms.
Light Consultation Phase: Health Insurance Is Not a Strong Demand
The misallocation of resources within traditional healthcare systems has long been criticized. Most founders of internet healthcare companies have, to varying degrees, experienced unpleasantness during their own medical journeys. Take Liao Jieyuan, founder of WeDoctor, as an example: the direct reason for his transition from a speech recognition expert to the healthcare sector was his young nephew’s development of a lump on the foot due to tuberculosis. Despite seeking care at multiple facilities, the condition was mistakenly diagnosed as a synovial hernia.
Leveraging internet technologies to address the challenges patients face in accessing medical care and finding the right specialists became the original intention of Liao Jieyuan, a technology-driven entrepreneur seeking to disrupt the traditional healthcare industry structure.
From the perspective of healthcare resource allocation, internet-based healthcare offers an efficient pathway to address the challenges of optimizing existing resources and bridging the information gap within the public tertiary hospital system, which has long suffered from systemic inefficiencies. To some extent, it facilitates the redistribution of physicians—a key productive factor in healthcare—thereby partially breaking down and lowering previous barriers and thresholds.
For these entrepreneurs, the goal is to leverage technological innovation to reduce the cost of healthcare services while improving their quality and coverage.
Around 2014, during the phase when internet healthcare was enhancing convenience, established platforms such as Chunyu Yisheng (Spring Rain Doctor), WeDoctor, and Haodf Online had already entered the public eye. However, a significant issue at that time was that the qualifications for online consultations remained unclear.
In particular, in April 2015, Song Shuli, spokesperson for the National Health and Family Planning Commission (the predecessor of the National Health Commission), stated that apart from telemedicine services provided by medical institutions, other activities involving medical diagnosis and treatment were not permitted to be conducted online. The suspended practice of online consultations subsequently evolved into health consulting services.
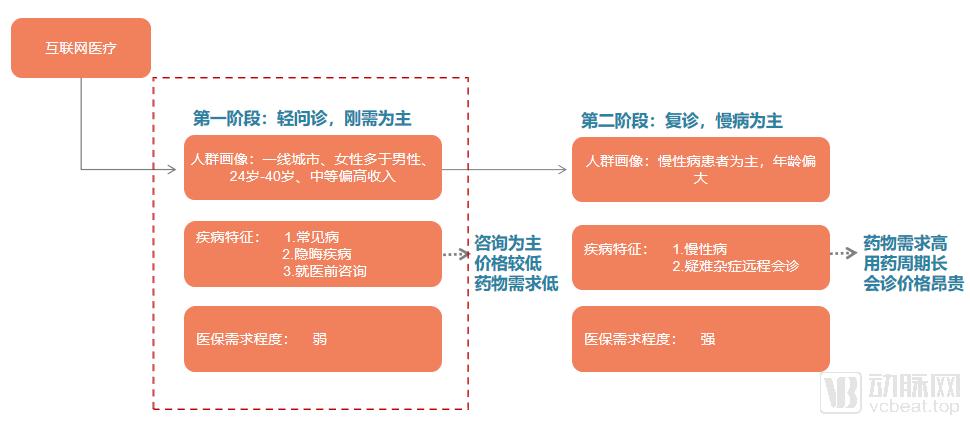
Phase I of Internet Healthcare Services: Focusing on Lightweight Consultations | Chart by VCBeat
Therefore, in the face of policy red lines and while exploring viable profit models, the first phase of internet healthcare can only focus primarily on lightweight online consultations.
Chunyu Doctor first introduced the “light consultation” model in 2011. This model primarily involves consultations on various diseases via text, image-and-text, voice, or video formats, providing only Q&A advisory services without offering treatment plans. This approach has since been gradually adopted by major platforms.
On major platforms, random consultations with attending physicians or higher-level doctors at standard tertiary hospitals typically range from ten to several dozen RMB. For complex or refractory cases requiring one-on-one video consultations with designated specialists in specific departments, prices generally range from 100 to 500 RMB.
Under this model, in 2015, Chunyu Doctor’s online consultation business generated actual revenue of RMB 130 million and a profit of RMB 30 million.
As shown in the figure above, an analysis of users of internet healthcare platforms reveals that the user profile of core internet healthcare users largely overlaps with that of China’s mobile internet users. This demographic primarily consists of urban young adults born in the 1980s and 1990s. Synthesizing reports from Analysys, Kantar Consulting, Frost & Sullivan, and VCBeat’s Eggshell Research Institute, it is found that 50% of internet healthcare users come from middle-to-high income segments, 40% reside in first-tier cities, the core user base has an average age range of 24–40 years, and female users constitute a majority.
To address the needs of this demographic during the initial online consultation phase, individuals who are accustomed to using mobile internet or those with higher incomes primarily leverage digital healthcare solutions to manage common conditions and sensitive issues (such as dermatological, andrological, and gynecological disorders), or to seek preliminary medical advice before visiting a hospital. This approach facilitates accurate symptom assessment, enabling patients to identify the appropriate clinical department for subsequent in-person care.
Therefore, during the early stage of online consultations, the issues that internet healthcare resolved for most patients included:
1. Reduce the time cost of hospital visits for ambiguous conditions;
2. Online consultations protect patient privacy and reduce the stigma associated with "avoiding medical care due to embarrassment" over sensitive conditions;
3. “Over-treatment” Caused by Visiting Hospitals for Minor and Common Illnesses.
In such medical demand scenarios, services utilizing light consultation typically exhibit the following characteristics:
1. During consultations, the focus is primarily on providing advice and recommendations;
2. There is no strong demand for repeat medication purchases, as short-term drug regimens are sufficient to improve or cure symptoms;
3. Use the Internet to address the issue of visiting hospitals for minor illnesses.
In light of the above characteristics, at that time, lightweight consultation services—which did not ultimately lead to prescriptions—were priced affordably and were primarily utilized for short-term needs. Consequently, repurchase rates were low unless similar needs arose again. Given their ability to meet demands for convenience and reduced hospital visits, reimbursement through medical insurance was not a critical necessity. Furthermore, the lightweight consultation model aligned well with the requirements of the tiered diagnosis and treatment system, which has been implemented since 2015.
Furthermore, from a business model perspective, the scale of paid consultations is small, and conversion rates for other revenue streams, such as value-added services, are low. This makes it difficult to establish a complete commercial closed loop. Consequently, platforms cannot rely solely on online models to sustain long-term development and urgently need to identify a new extension model.
Online consultations may not constitute a profitable business model capable of covering costs. For internet healthcare companies to fulfill their original mission, two conditions must be met: first, they must genuinely provide effective medical care; second, reimbursement depends on delivering quality care. In the second phase, a widespread integration between internet healthcare enterprises and physical hospitals emerged, with the internet hospital model flourishing across the board.
Internet Healthcare Ultimately Points to Follow-Up Visits for Chronic Diseases
In 2017, a document circulated online titled “Letter on Soliciting Comments on the Administrative Measures for Internet-Based Diagnosis and Treatment (Trial)” and “Opinions on Promoting the Development of Internet-Based Medical Services (for Public Comment)” (hereinafter referred to as the “Draft for Comments”) put the brakes on the explosive growth of internet hospitals and nearly forced all internet healthcare companies to start from scratch. Many people believed this marked the “death knell” for internet healthcare enterprises; however, they were unaware that another piece of information within the document actually charted a “clear path” for the future development of internet-based healthcare.
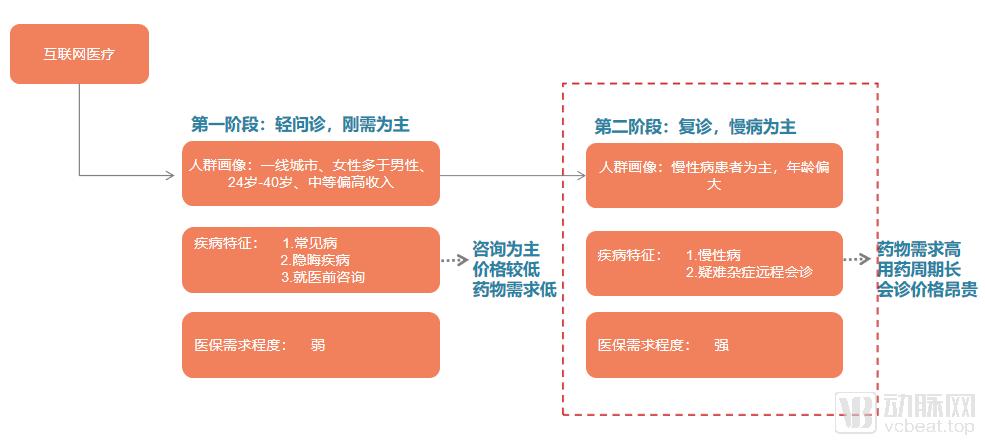
Transition to the Second Phase: Internet Medical Services Focused on Follow-up Visits and Chronic Disease Management. Graphic by VCBeat
In 2017, the "Administrative Measures for Internet-Based Diagnosis and Treatment (Trial) (Draft for Comments)" and the "Opinions on Promoting the Development of Internet-Based Medical Services" were released for public consultation. These documents clearly delineated core medical services from non-core medical services, encouraging the practice and exploration of internet technologies in areas "outside the core business of diagnosis and treatment."
What does this mean? It means encouraging internet-based healthcare to explore areas that physical medical institutions intend to address but are not particularly adept at handling. The core function of physical medical institutions is centered on disease treatment; therefore, beyond their core clinical services, these areas include pre-consultation health education and health science popularization, as well as post-consultation follow-up and chronic disease management.
In fact, since the compilation and implementation of the “Healthy China 2030” Planning Outline at the National Health and Wellness Conference in 2016, China’s healthcare service system has been gradually shifting from a disease-centered model to a health-centered one. Notably, the document explicitly sets forth the goal of “achieving chronic disease health management for the entire population across the full life cycle by 2030.” The management and control of chronic diseases have thus been elevated to a national strategic priority.
Moreover, past practice has shown that hospitals have performed poorly and lacked initiative in preventive care, chronic disease management, and disease rehabilitation. Therefore, conducting follow-up consultations on internet healthcare platforms offers inherent advantages for out-of-hospital chronic disease management.
Patients with chronic diseases are characterized by prolonged disease courses, extended medication regimens, and high drug volumes. In the context of an increasingly aging population, elderly individuals with mobility impairments constitute a major segment of the chronic disease patient group. Under previous conditions, patients with chronic diseases were required to visit hospitals frequently for follow-up examinations and prescription renewals. Shifting these follow-up visits to internet healthcare platforms offers dual benefits: on one hand, it provides convenience for chronic disease patients by eliminating the need for repeated hospital trips and avoiding processes such as registration and queuing; on the other hand, after prescriptions for chronic diseases are issued and reviewed by pharmacists, medical institutions and pharmaceutical distributors can entrust qualified third-party agencies to deliver medications directly to patients’ homes, thereby further enhancing the convenience of purchasing medicines.
For patients with chronic diseases who need to spend thousands of yuan on medication each month, whether they can be reimbursed by medical insurance has become a key issue.
As internet-based healthcare enters the era of follow-up consultations, the medication needs associated with chronic disease management underscore the necessity of medical insurance coverage. In fact, the official document released in 2018 closely mirrored the draft opinion circulated in 2017, highlighting four key factors: reliance on physical medical institutions, prohibition of initial online diagnoses, chronic disease management, and the outflow of prescriptions. Even during earlier exploratory phases, some companies had already been providing services in accordance with these standards.
"Has been consistently encouraged to be gradually included in the national medical insurance coverage."
In October 2014, the Guangdong Provincial Internet Hospital, affiliated with the Second People’s Hospital of Guangdong Province, became the first physical hospital to pioneer the “Internet Hospital” model. Just one year later, on December 7, 2015, Wuzhen Internet Hospital, the first internet hospital in China jointly established by WeDoctor and the Tongxiang Municipal Government, was launched in Wuzhen. These two models of internet hospitals represent distinct pathways: the former signifies public tertiary Grade A hospitals expanding into online services, while the latter represents internet healthcare companies extending their operations into offline settings.
In the subsequent process of incorporating internet-based healthcare services into the medical insurance system, hospital-centric online medical services have further clarified the logical framework for achieving insurance reimbursement, namely: unified pricing → formulation of a fee schedule → integration with local medical insurance systems → settlement.
To meet the reimbursement needs of individuals utilizing internet-based medical services, efforts to include such services in the national health insurance system have been underway since 2016.
On October 12, 2016, the Sichuan Provincial Health and Family Planning Commission (the predecessor of the Health Commission), the Development and Reform Commission, and the Department of Human Resources and Social Security took the lead nationwide in issuing the “Guiding Opinions on Accelerating the Promotion of Internet + Medical and Health Services,” while simultaneously introducing supporting policies such as pricing for “Internet + Medical and Health” service items and medical insurance reimbursement. Among these, internet-based diagnosis and treatment services, including remote consultations and online outpatient clinics, were explicitly assigned pricing and reimbursement standards, and relevant services provided by internet hospitals were eligible for inclusion in medical insurance coverage. The Sichuan WeDoctor Internet Hospital, jointly established by Wuzhen Internet Hospital and the Fourth People’s Hospital of Sichuan Province, as well as West China Second University Hospital of Sichuan University, were among the internet hospitals that benefited from this wave of policy dividends.
On March 19, 2017, the Yinchuan Municipal People’s Government issued the “Interim Measures for the Administration of Medical Insurance Personal Accounts and Outpatient Pooling for Internet Hospitals in Yinchuan” (hereinafter referred to as the “Measures”). For medical expenses incurred by Yinchuan residents through Haodf Online Yinchuan Smart Internet Hospital for services including text-based consultations, telephone consultations, disease counseling, and remote consultations, payment can be made using funds from their personal medical insurance accounts. Expenses that fall within the scope of the Basic Medical Insurance’s “Three Directories” are eligible for reimbursement from the pooled fund.
This document primarily regulates internet-based outpatient consultations, rather than directly addressing reimbursement for prescriptions. Given the policy constraints at the time, internet medical services were not authorized to issue prescriptions. Consequently, efforts to incorporate internet medical services into the national health insurance system remained confined to the initial stage of online consultations and did not involve cross-regional settlement mechanisms. However, patients could benefit from immediate cost offsets through direct online payment, eliminating the need for offline reimbursement procedures. A notable breakthrough during this period was the preliminary integration of Haodf Online with the Yinchuan municipal health insurance information system.
In September 2018, the National Health Commission of China issued three landmark documents: the “Administrative Measures for Internet-Based Diagnosis and Treatment (Trial),” the “Administrative Measures for Internet Hospitals (Trial),” and the “Standard Specifications for Remote Medical Services (Trial).” These regulations enabled internet hospitals to legally conduct follow-up consultations and prescribe medications for certain common and chronic diseases, thereby comprehensively standardizing the internet healthcare industry. The documents also explicitly stated that eligible internet-based diagnosis and treatment services would be gradually included in the scope of medical insurance reimbursement. It was this subsequent integration of internet healthcare with medical insurance that ushered in the era of reimbursable online medication purchases.
Prescription outflow is a key initiative in addressing reimbursement needs for medications used in the management of chronic diseases. According to Liu Xiaofang, President of Foshan Hospital of Traditional Chinese Medicine (TCM), in February 2019, the Foshan Medical Insurance Prescription Sharing and Convenience Service Platform was first piloted at the Internet Hospital of Foshan Hospital of TCM, which was jointly built and operated with WeDoctor. Residents of Foshan can complete online follow-up consultations, settle medical insurance claims, and have medications delivered by courier or pick them up quickly at nearby pharmacies—all via their mobile phones. Although this model does not involve direct online payment using medical insurance cards after teleconsultations, it represents the first such attempt in Foshan and is expected to be expanded in scope in the future.
In addition to the aforementioned cases, examples that have achieved certain breakthroughs in various aspects of including internet medical services in medical insurance coverage include:
In May 2018, Wuzhen Internet Hospital was included in the list of designated medical institutions for basic medical insurance in Tongxiang City, allowing insured employees in Tongxiang City to receive reimbursement for medical expenses incurred at the hospital.
In October 2018, 28 designated medical institutions in Guangzhou had launched online mobile payment services for medical insurance. Patients can directly use the online mobile payment function for medical insurance when seeking medical treatment.
In 2019, Guizhou Province included telemedicine service fees in the reimbursement scope of basic medical insurance and the New Rural Cooperative Medical Scheme (NRCMS). Patients in counties with extreme poverty can claim reimbursement for remote consultation and remote diagnosis services under standard medical service items, with reimbursement rates ranging from 70% to 85%.
Internet Healthcare Must Still Clear These Hurdles to Be Covered by Medical Insurance
A review of regions such as Guizhou Province, Sichuan Province, and Yinchuan City, which have continuously explored internet-based healthcare, reveals that their internet healthcare models have garnered significant attention largely due to their breakthroughs in pricing and reimbursement standards.
On June 4, 2019, the General Office of the State Council issued the “Notice on Key Tasks for Deepening the Reform of the Medical and Healthcare System in 2019” (hereinafter referred to as “Document No. 28 [2019]”), which explicitly stipulated the formulation of policy documents regarding fees for internet-based medical consultations and their coverage under medical insurance reimbursement. The National Healthcare Security Administration was designated as the responsible entity, with an emphasis on completing this task by the end of September 2019. The issuance of this document has made it increasingly clear that internet-based medical services are being formally integrated into the national medical insurance system across China.
Tan Wanneng, Public Relations Director at Chunyu Yisheng, stated that based on the timeline stipulated in Document No. 28 [2019] issued by the General Office of the State Council, it is highly likely that all provinces currently offering internet-based medical services will gradually include relevant internet diagnosis and treatment items within the scope of medical insurance coverage this year.
Whether it is a hospital-based internet hospital or an enterprise-run internet hospital, Document No. 28 [2019] marks the formal recognition of internet hospitals as an integral component of the medical service system. Moving forward, policy documents governing aspects such as pricing for online consultations and health insurance reimbursement must be formulated in accordance with the current laws and regulations of the medical service system.
Although explorations into incorporating internet-based healthcare into medical insurance have never ceased, in the face of the nationwide unified medical insurance policy implemented at the end of September, internet-based healthcare still needs to address these two core issues:
Internet-based healthcare is a typical non-standardized sector, with consultation fees varying across platforms depending on the physician and the specific services provided. However, the core of an internet hospital lies in its affiliated physical hospital. To incorporate internet-based diagnosis and treatment services into the hospital’s billing system, corresponding billing codes must be assigned to enable chargeable transactions. Therefore, standardized pricing for internet-based diagnosis and treatment services is essential, representing a prerequisite step before such non-standardized internet healthcare services can be included in medical insurance coverage.
When it comes to diagnostic and treatment services in internet healthcare, most people’s first impression is that they are expensive and non-standardized. The absence of unified service codes and exclusion from the official fee schedule mean that these services cannot be integrated into hospitals’ revenue systems. Under the “two separate lines” financial management system adopted by hospitals, where revenue and expenditure are managed independently, services not listed in the official fee schedule are ineligible for reimbursement from the basic medical insurance fund.
Currently, various regions, including Jiangsu Province, Guizhou Province, Sichuan Province, and Yinchuan City, have undertaken different initiatives to address pricing issues.
Taking Jiangsu Province as an example, in October 2018, Jiangsu Province solicited public opinions on the trial pricing for “Internet + Healthcare” services. The published table of trial prices for “Internet + Healthcare” services indicated that Jiangsu Province had announced 17 specific service items under four major categories: remote consultation, internet hospital outpatient services, remote diagnosis, and remote monitoring.
Among these, the price for remote consultation services ranges from 200 to 600 yuan, internet hospital outpatient visits cost between 10 and 50 yuan, and remote diagnosis fees range from 40 to 300 yuan. Remote monitoring prices are set independently by hospitals. No fee is charged for patients who only require medication pickup without a new treatment plan.
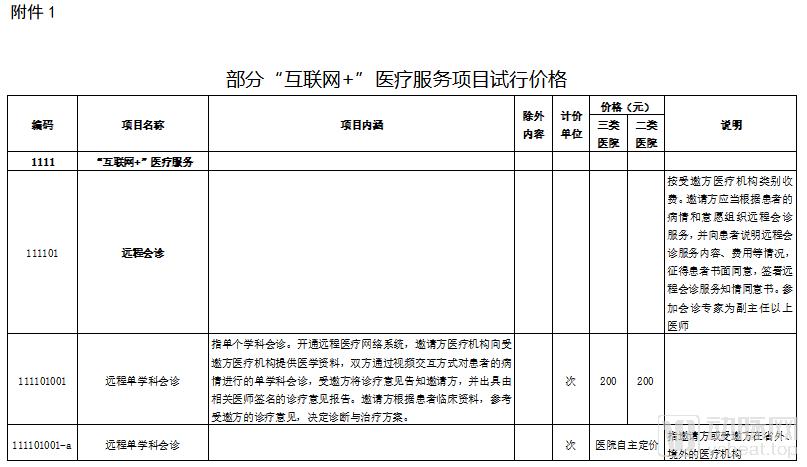
Trial Prices for Selected "Internet + Healthcare" Service Items in Jiangsu Province
The persistent status quo is that internet-based medical services lack a defined business model, making it difficult for price control authorities to calculate costs and set prices. Even in provinces and cities that have explored pricing mechanisms, the fees for remote consultations vary depending on the tier of the medical institution and the professional rank of the participating physicians. How to reasonably classify the diverse “Internet+” medical service items across different regions, uniformly price those services that should be covered by the basic medical insurance fund, and incorporate them into the reimbursement system remains a challenge. Reasonable pricing must be established based on a comprehensive assessment of the costs associated with remote service delivery.
Hospital revenues and expenditures are managed as two separate lines. For internet-based diagnosis and treatment, this is not only driven by the needs of patients with chronic diseases; it also applies to patients with complex or refractory conditions seeking high-quality medical resources. In such cases, a significant proportion of remote medical consultations will be initiated by patients from other regions, ultimately involving cross-regional settlement.
From an internet-centric perspective, telemedicine exhibits distinct cross-regional characteristics. Beyond establishing corresponding fee schedules and defining services eligible for reimbursement, enterprises are seeking more robust institutional frameworks to facilitate cross-provincial direct settlement of medical insurance for telemedicine services.
Due to the convenience of the internet, most services provided by internet hospitals involve cross-regional medical care, while local residents generally still prefer in-person visits at physical medical institutions. For expenses incurred from cross-regional medical treatment, the portion covered by the basic medical insurance fund through cross-provincial direct settlement is typically recorded as accounts receivable by the treating hospital. The handling agency in the place of treatment is responsible for settling payments with the hospital for these recorded amounts, while the provincial-level handling agency is responsible for final reconciliation and clearing.
Under such a system, not only is the hospital’s settlement infrastructure put to the test, but achieving real-time reimbursement settlements for internet hospitals integrating with the medical insurance system also presents considerable challenges.
Will Internet Healthcare Enjoy a Smooth Path Forward with Health Insurance Coverage?
Does the inclusion of internet-based medical services in health insurance coverage, akin to physical hospitals and clinics, directly attract more patients and boost revenue?
For most internet healthcare companies, the inclusion of their services in the national medical insurance scheme is significant positive news. However, the aforementioned representative stated that this is not necessarily the case from the hospital’s perspective. In scenarios where a single legal entity handles unified settlement, incorporating internet-based diagnosis and treatment into medical insurance essentially establishes clear reimbursement standards for what functions as a newly added department.
A large number of internet healthcare companies have chosen to either build their own platforms or partner with physical medical institutions to obtain internet hospital licenses, which symbolize regulatory compliance. However, if these efforts fail to translate into patient prescriptions, the clinical consultation process remains incomplete, and patient experience is difficult to satisfy, ultimately preventing any conversion into profitability.
Therefore, industry insiders speculate that the ultimate goal of including internet medical services in the national health insurance scheme may be to facilitate the outflow of prescriptions.
From the perspective of the current system, the entity responsible for accommodating the outflow of prescriptions is the prescription-sharing platform. This platform needs to integrate hospital information systems (HIS) with pharmacy management systems (ERP), forming a comprehensive ecosystem centered on hospitals and jointly developed by various government departments and pharmacies. This ecosystem aims to achieve interconnectivity among medical institution prescriptions, medical insurance settlements, and pharmaceutical retail. Internet healthcare platforms will ultimately serve as the connecting link between hospitals upstream and pharmaceutical companies downstream.
Under the backdrop of the “4+7” volume-based procurement policy, the profit margins for pharmaceutical companies have shrunk sharply. For hospitals, the era of subsidizing medical services with drug revenues is coming to an end. Pharmacies are increasingly functioning as cost centers, with drug procurement shifted outside hospital walls. This approach helps hospitals reduce their drug-to-revenue ratio, allows pharmaceutical companies to bypass the costs associated with getting drugs listed in hospitals, and makes it more convenient for patients to purchase medications.
Following online consultations, patients can use their medical insurance cards for payment and settlement. Similar practices of prescription outflow have already been implemented in Chinese provinces such as Guangdong and Zhejiang. This truly achieves the goal of internet hospitals connecting end-users, hospitals, and pharmaceutical companies.
In addition, regarding practical implementation, Tan Wanneng stated that, based on the supporting documents issued by various provinces to date, the pricing and reimbursement for internet-based medical consultations are likely to follow the approaches adopted in certain provinces. For instance, “medical service items delivered via the internet that fall under basic medical services shall comply with the standard pricing regulations for basic medical services and be included in the scope of medical insurance coverage as prescribed; for services characterized by sufficient market competition and strong demand for personalized care, market-regulated pricing shall apply.” Meanwhile, the introduction of systems such as Diagnosis-Related Groups (DRGs) cannot be ruled out.
Therefore, before the detailed implementation rules are officially released, companies should primarily focus on making preparations in terms of information sharing and regulatory compliance. All answers will be revealed in September.
Overall, the inclusion of internet-based medical services in the national health insurance scheme may represent another significant hurdle overcome by the sector amidst its many twists and turns. However, the path ahead is not necessarily smooth; internet healthcare companies must adapt to their evolving roles while coordinating with government agencies and hospitals. Fortunately, as the market transitions from a wild, unregulated state to an orderly one, the outlook for internet healthcare is gradually improving.
The transformation of the healthcare industry through internet technology has remained sluggish to this day. The fundamental reason lies in the fact that, for physicians, clinical practice is a matter of life and death. This has fostered a long-standing model of trust in healthcare, one rooted in offline, face-to-face interactions. This explains why internet-based healthcare has yet to penetrate the core of diagnosis and treatment. Even as hospitals have opened their doors to digital integration, authority over initial consultations and prescription rights remains tightly controlled.
Here, I would like to quote a wise remark published by a WeChat official account author in 2016, which remains equally applicable to today’s internet healthcare sector: “This industry is moving too slowly. So much so that five years after its emergence, most people have lost their patience and are eagerly predicting its decline. I have no effective way to change this pessimistic mindset; I can only continuously seek out and observe new ‘gold mines’ and trends within the industry. Fortunately, most of the time when I look to the future, I remain optimistic.”
Once the supporting medical insurance policies are finalized in September, will they revitalize internet healthcare as previous favorable measures have? This time, we hope to see tangible data-driven results from these policy changes.