Physician Employment Models in Premium Private Hospitals: The Key to Breakthrough Lies in the Advancement of Multi-Practice Licensing
Physician Employment Models Are Crucial for Private Hospitals. A well-structured physician employment model can help private hospitals efficiently attract high-caliber physicians and healthcare teams, establish differentiated branding, ensure stable hospital management, and achieve reasonable cost control.
Certainly, for private hospitals, establishing an optimal physician employment model requires consideration of their own financial situation and market positioning, as well as the current state and future development of the market. This article will take Shanghai's existing high-end private hospitals as examples to delve into the current status of physician employment models in private hospitals from various perspectives.
Development and Current Status
Looking back 5 to 10 years ago, ultra-premium private healthcare providers such as United Family Healthcare and Parkway Pantai primarily targeted the ultra-high-end market, particularly the expatriate community. Consequently, in terms of physician composition, foreign doctors practicing in China constituted the vast majority of their medical staff.
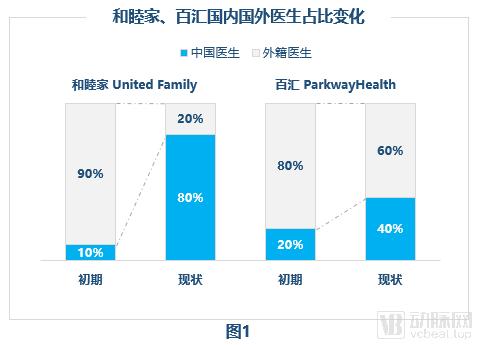
However, due to the rapid development of China's economy, the target clientele of such ultra-premium private hospitals has gradually shifted toward high-end domestic customers, leading to certain changes. Taking United Family Healthcare as an example, in its early years, it relied primarily on foreign physicians and mainly served expatriate patients and senior executives of multinational corporations stationed in China. Currently, it is gradually transitioning to a model dominated by Chinese physicians, with international physicians primarily serving only expatriate patients.
For another example, consider Parkway Healthcare. Although its target customers remain primarily expatriates, the proportion of high-end patients with commercial health insurance among its current patient base is gradually increasing. Consequently, the proportion of foreign physicians has decreased from 80% in the early stages to approximately 60% at present (Figure 1).
Of course, despite this, such high-end private hospitals still impose additional requirements on locally recruited physicians. For instance, United Family Healthcare requires local physicians to have overseas work experience; those without such experience must participate in the hospital’s training program and pass the assessment. Additionally, full-time physicians must be proficient in two or more languages.
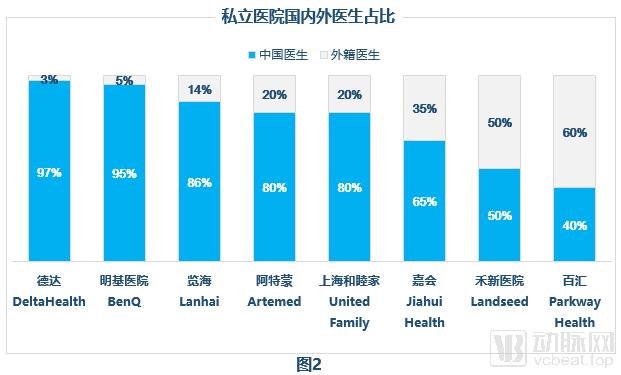
Examining the current situation of high-end private hospitals in Shanghai, the proportion of local and foreign physician teams is still determined by their respective differentiations, market positioning, and customer base (Figure 2). For example, DeltaHealth focuses on cardiovascular diagnosis and treatment, with its target customers being domestic high-end patients with cardiovascular diseases; therefore, foreign physicians account for only about 3% of its medical team.
Of course, although the proportion of full-time foreign physicians is decreasing, the practice of dispatching foreign physicians remains very common due to the increase in overseas collaborative projects, such as those between Jiahui Health and MD Anderson, and between Artermed and its German headquarters. Taking DeltaHealth as an example, due to its partnership with Columbia University Medical Center (CUMC), CUMC regularly dispatches experts to provide consultations at DeltaHealth and offers clinical guidance and training to DeltaHealth physicians.
Therefore, a hybrid model combining local and foreign physicians, tailored to specific needs, can effectively help private hospitals attract high-end local patients while securing their foreign patient market. Furthermore, this collaborative approach brings a range of additional benefits to the hospital.
From another perspective, the hybrid model combining part-time (multi-site practice) and full-time physicians has undergone a series of changes in recent years. In the early stages, ultra-high-end private hospitals primarily adopted a full-time employment model for physicians. This was mainly because the recruited physicians were mostly foreign nationals who did not hold positions in public hospitals, making it easier to hire them on a full-time basis.
However, the situation is slightly different for some mid-to-high-end hospitals. The primary model for these institutions involves part-time engagement of specialists from Grade 3A hospitals. Recruiting such part-time experts requires either obtaining permission from their affiliated public hospitals or engaging specialists who are approaching retirement and thus transitioning into the private healthcare system on a part-time basis.
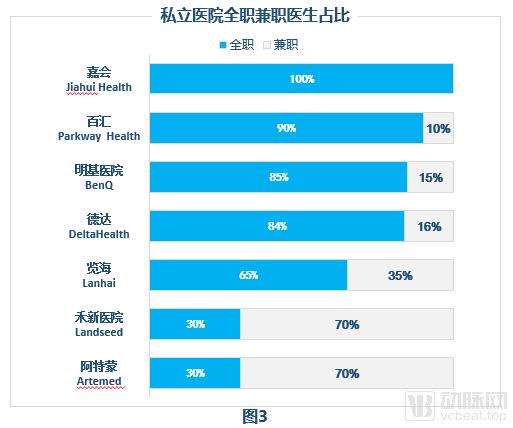
After several years of rapid development in the private healthcare sector, mid-to-high-end part-time specialists are increasingly transitioning to full-time roles. This shift is driven not only by personal factors such as retirement but also by attractive working environments and compensation packages comparable to those in public hospitals. However, in ultra-high-end private hospitals, part-time physicians are gradually becoming a notable feature of their physician employment models (Figure 3). Notably, the proportion of part-time physicians at Luxhealth and Arterton has even reached 70%.
Balancing the Ratio of Full-Time to Part-Time Physicians: A Private Hospital Must Weigh the Pros and Cons (Figure 4).
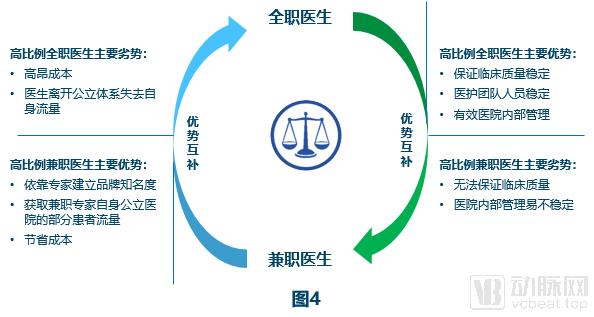
Full-time physicians can ensure clinical quality and stability in hospital management, yet the most significant drawback lies in the high costs. Meanwhile, physicians who completely leave the public healthcare system may lose a portion of their patient flow, resulting in certain losses for both private hospitals and the physicians themselves. The advantage of the part-time physician model is that private hospitals can build brand awareness by leveraging renowned experts while also capturing a share of the patient flow from these experts’ affiliated public hospitals.
Of course, for these experts from public hospitals, the high surgical volume in public hospitals allows them to maintain their surgical skills while also practicing at multiple private hospitals, which appears sufficiently attractive. However, the downside is that clinical quality cannot be guaranteed to some extent.
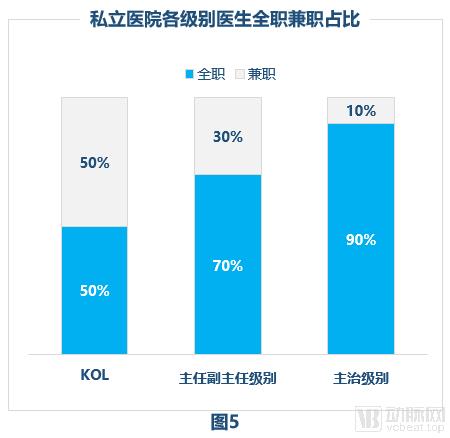
Therefore, in ultra-premium private healthcare (Figure 5), physicians in core departments are predominantly full-time employees; however, young key clinicians involved in hands-on practice are often part-time. In contrast, physicians in non-core departments, including those at the director level, remain primarily part-time.
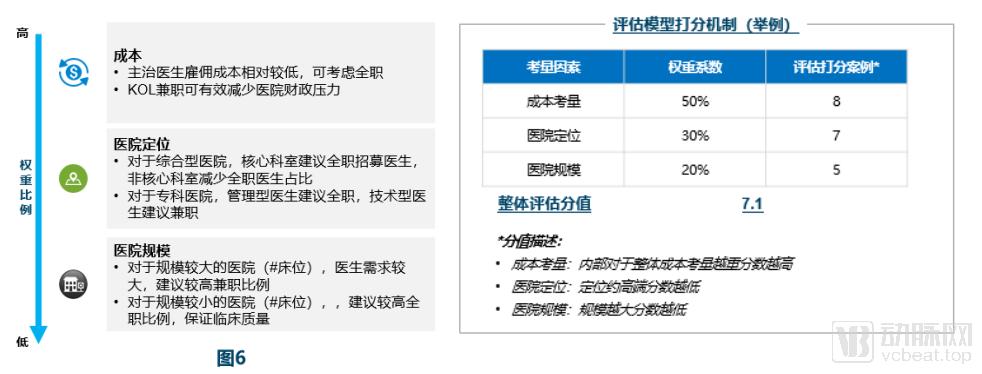
Overall, based on the hospital’s specific circumstances and strategic direction, a reasonable ratio of full-time to part-time physicians can be designed across three main dimensions (Figure 6).
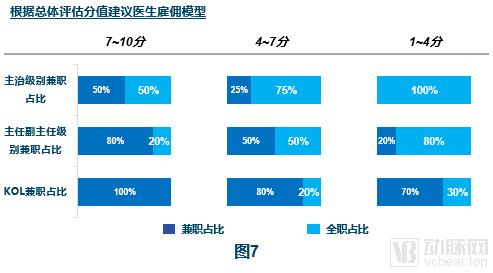
By scoring the overall self-positioning model and based on the comprehensive evaluation score, an appropriate physician employment model is selected (Figure 7).
Certainly, once the physician structure is established, the next step is to consider how to attract physicians. Broadly speaking, there are three key factors for private healthcare institutions in attracting physicians:Compensation, Practice Environment, and Work-Life Balance。
The primary challenge undoubtedly lies in compensation. The most critical factor for private hospitals is to match the salary and benefits that physicians receive in public hospitals. However, for certain specialists who already command substantial incomes in the public sector, private hospitals must offer even higher remuneration to recruit them, imposing a significant financial burden on these institutions.
Therefore, it is now common practice to offer such physicians equity stakes in addition to high compensation; for instance, experts hold shares at institutions like United Family Healthcare and DeltaHealth. For mid-level physicians, private hospitals can attract talent by offering salaries higher than those in public hospitals and providing accelerated promotion pathways.
Secondly, private hospitals offer a favorable practice environment, such as more comfortable consultation rooms and longer consultation times, which are significant attractions for physicians.
Finally, there is the matter of work style. The excessively high patient volume in public hospitals places significant work pressure on physicians. In contrast, most private hospitals operate on an appointment-based system, allowing doctors to schedule their clinic hours with sufficient time, thereby improving their quality of life.
Future Trends
From the current perspective, experts in the industry would consider that the current private healthcareEmployment models are unlikely to change significantly within the next decade.. The primary reason still lies inThe implementation of multi-site practice has been relatively slow.. Therefore, for private hospitals, regardless of how they structure their physician workforce or recruit doctors, the top priority remains ensuring the quality of medical care.
First, private hospitals need not only to train full-time physicians but also to provide training for part-time physicians through various channels, such as overseas collaborative programs. Second, it is advisable to recruit physicians at the level of department director and above on a full-time basis, as these professionals possess the capability to oversee treatment protocols, strengthen hospital management, and ensure medical quality. Therefore, although the short-term imbalance of insufficient physicians relative to the number of hospitals cannot be immediately reversed, private hospitals will continue to improve their oversight of part-time physicians through a series of measures. Finally, with policy support, multi-site practice is expected to become more prevalent in the future, which bodes extremely well for the private healthcare sector.
Source: [Ryan Partners]】, published with authorization from VCBeat. The views expressed above do not necessarily represent the position of VCBeat.
Original Title: Brewing Wine to Discuss Heroes: The Employment Model for Physicians in Private Healthcare