AI-Powered Diabetic Retinopathy Screening: China's Nationwide Prevention Initiative Reaches 680,000 Screenings in Three Years
The public lacks awareness of disease prevention.
"This is the greatest insight Professor Sun Zilin from Zhongda Hospital of Southeast University has gained over his 20 years of medical practice. As a senior endocrinologist, he has treated countless patients, but three particular experiences have left a lasting impression on him."
“More than a decade ago, a young girl from a rural area came to our hospital and was diagnosed with type 1 diabetes. Due to financial constraints, her condition was already severe upon arrival. Furthermore, the traditional preference for sons over daughters led to her family’s lack of proactive engagement in her treatment. I deeply regret the ultimate outcome.”
“The second case involved an entrepreneur in the IT industry whom I encountered a few years ago. This individual was wealthy and faced no financial constraints. He suffered from type 2 diabetes, which had already led to diabetic retinopathy and renal insufficiency by the time he sought medical attention. Upon inquiry, the underlying causes were invariably his excessive occupational demands, irregular lifestyle, and tendency to endure minor symptoms until they became unbearable, at which point it was already too late.”
“A while ago, the dean of an engineering school from a certain university came to me for medical consultation, which left me deeply reflective. This group is never lacking in knowledge; on the contrary, they are carriers of knowledge and promoters of science. However, their awareness of disease prevention is virtually nonexistent.”
These three cases reflect a widespread lack of awareness regarding diabetes prevention, and disease prevention in general, across diverse populations and socioeconomic strata. In fact, timely screening and early intervention can significantly alleviate the financial burden on both patients and the national healthcare insurance system. Moreover, such measures can prevent irreversible physiological damage, such as vision impairment or even blindness caused by diabetic retinopathy.
In fact, as early as October 28, 2016, the National Health and Family Planning Commission formulated the “13th Five-Year” National Eye Health Plan (2016–2020), incorporating the protection of citizens’ visual health into its overall planning.
Data show that fundus screening can reduce the risk of severe vision loss from diabetic retinopathy by 94.4%.
However, according to 2016 statistics from the National Health and Family Planning Commission, China currently has only 32,000 ophthalmologists, among whom approximately 800–1,000 are engaged in the provision of fundus disease services and research. Relative to the more than 100 million patients with diabetes mellitus, there is a severe shortage of ophthalmologists, which constitutes a major reason for the very low screening rate for diabetic retinopathy in China.
Professor Sun Zilin stated that while the shortage of ophthalmologists is one factor, another critical issue is the need for collaborative efforts between ophthalmologists and endocrinologists in the prevention and management of diabetic retinopathy. However, in actual clinical practice, few physicians possess the awareness, time, or capacity to conduct diabetic retinopathy screening. “I can understand patients’ lack of awareness regarding diabetic retinopathy prevention and control, but for a long time, many hospitals and physicians have also lacked such awareness. We need to correct this mindset.”
Amid these pressing challenges, screening and prevention for diabetic retinopathy cannot be delayed. In essence, diabetic retinopathy is a complication arising from the progression of diabetes. Its greatest significance in prevention and control lies not merely in averting ocular diseases, but in the broader management of diabetic complications. Therefore, the most effective current approach is to integrate it into endocrinology-based diabetes care, treating it as a fundamental indicator for diabetes monitoring, rather than viewing it solely through the lens of ophthalmic disease.
Advancing awareness of diabetic retinopathy screening and prevention is a top-down process; it requires physicians to take the lead before residents can be effectively engaged. Therefore, the first step is to identify the key leverage point for driving this initiative.
In June 2016, the “China Diabetic Retinopathy Screening and Prevention Project” was launched in Beijing. Centered on three core objectives—raising awareness of diabetic retinopathy screening among hospitals, physicians, and patients; conducting diabetic retinopathy screening; and reducing the incidence of diabetic complications—the project has redefined the concept of “network” and leverages diabetic retinopathy screening and prevention to mitigate diabetes and its complications.
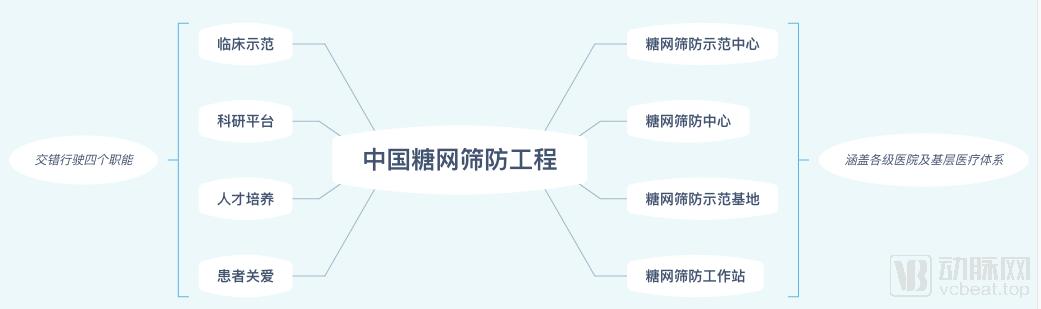
Diagram of the Structure and Functions of China's Diabetic Retinopathy Screening and Prevention Project
This initiative is hosted by the Chinese Society of Microcirculation and the National Technical Steering Group for Blindness Prevention, undertaken by the Professional Review Committee on Diabetes and Microcirculation of the Chinese Society of Microcirculation, with artificial intelligence technical support provided by Beijing Shanggong Yixin Technology Co., Ltd. Aimed at “increasing the screening rate for diabetic retinopathy and preventing blindness in patients with diabetes,” the project is led by Professor Sun Zilin.
As of June 2019, the China Diabetic Retinopathy Screening and Prevention Project had completed screening for diabetic retinopathy in 680,000 cases across more than 400 medical institutions in 28 provinces and municipalities nationwide, with all screenings supported by artificial intelligence technology.
Professor Sun Zilin expressed great satisfaction with the application of artificial intelligence technology in this project: “In our screening and prevention initiative, the accuracy rate of AI technology reached 89%. In real-world practice, this is already a very high figure.”
More importantly, this technology enhances the diagnostic and treatment capabilities of primary healthcare institutions such as community health service centers and health stations. A major reason for patients’ reluctance to seek care at the primary level is their lack of confidence in the quality of care provided there, and AI directly addresses this pain point.
In fact, eye diseases and artificial intelligence (AI) technology have a natural synergy. This is because fundus photography is more convenient, more universally applicable, and easier to scale up, providing AI companies with larger datasets to enhance the intelligence of their algorithms.
Moreover, national policies have also provided clear direction for the development of AI enterprises. In the past, when the state prioritized the diagnosis and treatment of glaucoma, there was a significant increase in glaucoma-related products. Similarly, as diabetes chronic disease management became part of the national strategy, diabetic retinopathy naturally emerged as a key focus for AI product development.
For the China Diabetic Retinopathy Screening and Prevention Project at its current stage, artificial intelligence primarily serves as a physician’s assistant, significantly enhancing the screening and prevention capabilities of grassroots institutions such as demonstration bases and workstations for diabetic retinopathy screening and prevention.
Beyond identifying the characteristics of fundus photographs, artificial intelligence (AI) technology is poised to shift the management of diabetic retinopathy from current screening and prevention strategies toward future-oriented preventive care. AI imaging companies can empower the entire data processing workflow; through continuous technological refinement, they can assist medical institutions in constructing robust disease models, thereby providing guidance for disease prevention.
From the perspective of data utilization, AI companies can, on one hand, optimize existing algorithms to enhance their accuracy, sensitivity, and robustness. Secondly, extensive data collection provides valuable guidance for physicians to deeply explore the underlying associations between diabetes and its complications. Furthermore, given the current scarcity of medical resources, providing flexible health management recommendations to diabetic patients through interval-based data collection may prove superior to traditional periodic follow-ups. From a macroscopic viewpoint, regional disease prevention and control also require such big data analytics.
In practice, the project categorizes institutions involved in diabetic retinopathy (DR) screening and prevention into four tiers. Professor Sun Zilin stated that screening data from the China DR Screening and Prevention Project reveal that the current primary screening population is concentrated in Tier 1 and Tier 2 institutions—namely, the DR Screening and Prevention Demonstration Centers affiliated with provincial-level Grade A tertiary hospitals, and the DR Screening and Prevention Centers affiliated with prefecture-level city Grade A tertiary hospitals.
Data as of late June show that Grade A tertiary hospitals participating in China’s Diabetic Retinopathy Screening and Prevention Project account for approximately 40% of the entire initiative, yet they have screened 510,000 patients with diabetic retinopathy, representing 75% of the total screening volume.
From the current perspective, although the Diabetic Retinopathy Screening and Prevention Project’s screening workstations in China have begun to take shape, patients still place greater trust in major Grade 3A hospitals.
At the heart of the matter remains the issue of trust: How can patients be retained at the primary care level to maximize the value of diabetic retinopathy screening stations?
In March 2017, the General Office of the National Health and Family Planning Commission issued the “Technical Plan for Tiered Diagnosis and Treatment Services for Diabetic Retinopathy,” aiming to achieve early detection and early intervention for diabetic retinopathy through the implementation of a tiered diagnosis and treatment system, thereby reducing the disease burden on the public. However, in practice, the successful implementation of this plan requires joint efforts from both hospitals and patients.
A glimpse into the family physician community reveals that, as managers of community health for residents, many family physicians have not played their ideal role in the management of patients' chronic diseases, with contracts signed but little actual management provided.
Gu Yuan, Professor of General Practice at Capital Medical University, told VCBeat, “Health insurance must first recognize the role of primary care institutions, rather than having patients seek treatment at large hospitals and then return to their communities to purchase medications with prescriptions. The true function of community healthcare is to serve as a gatekeeper.”
Thus, the incentive issue has become central. “Family doctors are currently reluctant to order diagnostic tests because such tests are not linked to medical insurance reimbursement, offering no benefits to any party. However, effective testing can facilitate early identification of patients’ symptoms and significantly reduce medical costs. Therefore, medical insurance is the key to the problem. If the payment model were shifted to capitation-based prepayment with a fixed management budget, outcomes in early diagnosis and early rehabilitation would improve,” said Gu Yuan.
The diabetic retinopathy screening workstation also requires the same mechanism; meanwhile, establishing a strong trust relationship with patients is another key factor for the workstation to function effectively.
Wu Hao, Director of the Beijing Fangzhuang Community Health Service Center, aptly summarized: “The core of general practice lies in continuity. You must make every effort to build friendships with residents and patients. Once you establish such relationships and serve them with genuine care, continuity will naturally follow. Continuity implies sustained health care services, which in turn lead to a series of favorable health outcomes.” This is precisely the core objective that Diabetic Retinopathy Screening Workstations must achieve.
Regarding the aforementioned issues, the Maigaoqiao Community Health Service Center in Nanjing (hereinafter referred to as “Maigaoqiao Community”) may offer some insights.
As of June 2019, this Nanjing-based community health center had provided health management services to 129,000 residents. Its diabetes specialty department, established in March 2016, currently employs 29 staff members, including 14 with intermediate or senior professional titles. The specialty team adopts a “multi-disciplinary co-management” model, comprising specialists, dedicated health education nurses, rehabilitation therapists, dietitians, and health managers.
Data show that the Maigaoqiao Community Specialist Outpatient Clinic recorded over 60,000 patient visits. From January to August 2018, the volume of specialist outpatient visits increased by 67% compared to the same period in the previous year, while operational revenue from specialist services rose from over RMB 1 million in 2016 to more than RMB 7 million in 2018, representing a 193% increase.
The unique feature of the Maigaoqiao Community lies in its management objective of “Two Integrations and Three Characteristics.” The “Two Integrations” refer to the integration of doctors and patients, and the combination of prevention and education. The “Three Characteristics” denote the standardization of diabetes diagnosis, treatment, and screening; patient compliance and adherence; and the stickiness between the community and patients with chronic diseases.
To strengthen the connection with patients and enhance their self-awareness and engagement in treatment, diagnostic and therapeutic plans as well as lifestyle intervention strategies are jointly developed by physicians, patients, and the diabetes management team. Under this model, patients develop a sense of collaborative partnership, recognizing that disease management is not a solitary endeavor, thereby directing greater effort toward health management.
Furthermore, the Maigaoqiao Community has established four WeChat groups for individuals with diabetes, launched the “Mai Dong Tang Meng” (Maigaoqiao Diabetes Alliance) Club to encourage patient exercise, and implemented a membership-based points management system, thereby sustaining the sense of engagement patients experienced during enrollment throughout the ongoing management period.
In terms of health management, the Maigaoqiao Community will conduct annual screening for diabetes-related complications among enrolled patients with diabetes, aiming to achieve early detection and intervention. Specialized technical services, including diabetic foot screening, vibration perception threshold testing, fundus photography, bone mineral density assessment, and intensive insulin pump therapy, enable a comprehensive evaluation of patients’ diabetic status from multiple perspectives.
As a modern community integrating prevention and treatment, patients can sign up for exclusive health managers and specialist physician teams via the WeChat platform of the Maigaoqiao Community Health Service Center’s integrated management system, enabling online disease management. Furthermore, the platform provides online diagnosis, treatment, and consultation services with experts from tertiary hospitals.
“At the inception of the project, our goal was to screen 100,000 individuals within three years; however, in just two years, we have screened nearly 700,000 people. While this figure may seem modest relative to the total population, it represents a promising start.” Reflecting on the achievements of the past two years, Professor Sun Zilin expressed mixed emotions.
“Now that the ripple effect is beginning to emerge, the expansion of China’s Diabetic Retinopathy Screening and Prevention Project will become much more straightforward. In terms of overall direction, we will shift our focus from quantity to quality, establishing truly effective prevention mechanisms, which is the fundamental objective of this initiative.”
Specifically, progress must continue in two areas. First, decentralize patient care to community health stations and promote the Maigaoqiao model nationwide. Second, accelerate the technological empowerment of primary healthcare, improve the diabetic retinopathy database, enable physicians to leverage big data to build regional patient models for diabetic retinopathy, and fully implement the supportive role of artificial intelligence at the primary care level.
However, it is crucial to remain vigilant about patients’ persistent reluctance to seek care at primary healthcare facilities. In the absence of adequate payment safeguards and effective resource allocation mechanisms, widespread diabetic retinopathy screening at the primary care level will not be realized. This requires policy-backed safety nets, and greater multi-stakeholder participation is needed to strengthen the development of primary healthcare stations.