GLP-1 Receptor Agonists: The Future First-Line Therapy Set to Replace Insulin in Type 2 Diabetes Management
In March 2019, the Queenstown Molecular Biology Meetings, themed “Drug Discovery and Technological Innovation,” were held in Shanghai. The academic event was co-chaired by Professor Wang Mingwei, Director of the National Center for Drug Screening, and Professor Peter Shepherd from the University of Auckland, New Zealand. Professor Daniel Drucker from the University of Toronto, Canada, delivered a special lecture titled “GLP-1 Receptor Agonists for the Treatment of Diabetes and Metabolic Diseases,” which garnered significant acclaim.
Daniel Drucker, MD,PhD
Professor Drucker is a founding figure and distinguished leader in the field of GLP-1. His pioneering achievements in GLP-1 drug research and therapy earned him the Banting Award at the 74th Scientific Sessions of the American Diabetes Association (ADA, 2014).
As early as 1987, Professor Drucker observed that GLP-1 promotes insulin secretion and hypothesized that it serves as a “physiological regulator of insulin gene expression,” thereby launching his research career focused on GLP-1. Over the past three decades, he has been granted 29 U.S. patents. His scientific achievements have sparked a revolution in the history of diabetes treatment, directly leading to the development and commercialization of two major classes of drugs: GLP-1 receptor agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors. These substantial and direct translational medical outcomes have benefited countless patients worldwide.
As an endocrinologist and former Director of the Banting-Best Diabetes Centre (BBDC) in Canada, Professor Drucker recounted the discovery of GLP-1 in his report, introducing its biological functions and pharmacological mechanisms. He began with the first marketed short-acting agent (exenatide) and provided a systematic review of long-acting GLP-1 drugs up to the present (dulaglutide), offering insights into the future prospects of GLP-1 drug development.
In 1921, Professor Frederick Banting of the Department of Physiology at the University of Toronto and his student Charles Best discovered insulin and its efficacy in treating diabetes. This marked a major revolution in the medical field, and Banting was awarded the Nobel Prize in 1923 for this achievement.
For nearly a century thereafter, insulin remained the first-line injectable therapy for diabetes. However, the emergence of GLP-1 has disrupted insulin’s century-long dominance as the first-line agent. GLP-1 receptor agonists not only exhibit glucose-lowering efficacy comparable to that of insulin but also offer additional benefits derived from their pleiotropic effects, including appetite suppression, weight loss, and cardiovascular benefits.(1)These benefits are not offered by insulin or other oral hypoglycemic agents.
Insulin therapy carries a high risk of hypoglycemia, whereas GLP-1 lowers blood glucose in a glucose-dependent manner, resulting in an extremely low risk of hypoglycemia. Most patients with type 2 diabetes are obese; further weight gain associated with insulin injection therapy can exacerbate metabolic disturbances and increase the risk of mortality from diabetes-related complications, including both microvascular and macrovascular complications.(2). The weight-loss efficacy of GLP-1 receptor agonist therapy is highly beneficial for patients with diabetes. More importantly, its cardiovascular benefits contribute to excellent clinical adherence during long-term GLP-1 treatment.

Discovery of insulin by Drs. Banting and Best in 1921
Professor Drucker also analyzed the development prospects of drugs from a market perspective. GLP-1 drugs currently account for 10% of total sales in the diabetes treatment market, while China accounts for only 2–3%, indicating significant room for growth. In his concluding remarks, Professor Drucker optimistically pointed out that in the near future, GLP-1 drugs will replace insulin as the first-line therapy for diabetes.
GLP-1 Enters U.S. Diabetes Guidelines as a First-Line Therapy
In 2019, the American Diabetes Association (ADA)(3) and the European Association for the Study of Diabetes (EASD) (4)New Clinical Practice Guidelines Released. The guidelines recommend against using insulin as first-line therapy for type 2 diabetes and designate GLP-1 receptor agonists as the preferred injectable treatment for diabetes in most cases. The rationale is summarized in the following three aspects:
1) GLP-1 has glucose-lowering efficacy similar to that of insulin, but with a very low risk of hypoglycemia;
2) GLP-1 not only lacks the weight-gain side effect associated with insulin therapy, but also has weight-loss benefits;
3) GLP-1 has cardiovascular protective effects (Table 1).

Table 1. Comparison of the Glucose-Lowering Characteristics of Insulin and GLP-1 Receptor Agonists
In patients with type 2 diabetes and confirmed atherosclerotic cardiovascular disease, the use of GLP-1 receptor agonists offers "proven cardiovascular benefits." Guidelines also recommend GLP-1 receptor agonists for patients with type 2 diabetes and chronic kidney disease. For patients with hyperglycemia due to gestational diabetes, metformin and glyburide are not recommended as first-line agents because they cross the placenta and affect the fetus; alternative medications, such as GLP-1 receptor agonists, should be considered.
In recent years, insulin sales have declined year over year, while the market for GLP-1 drugs has surged (see Figure 1). With the introduction of new guidelines in 2019, this trend is expected to become even more pronounced.
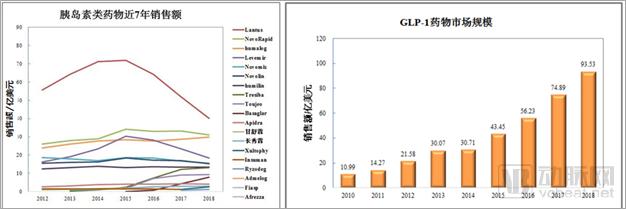
Figure 1.Global Insulin Sales Decline Year on Year, While GLP-1 Drug Sales Continue to Rise
Source: Armstrong, 2018 Diabetes Market Research Report: GLP-1 Receptor Agonists Stand Out
Only Human-Derived Long-Acting GLP-1 Can Provide Cardiovascular Benefits
Professor John B. Buse, a leading authority on diabetes, in the journal *Metabolism* in June 2019(5)Published a paper providing an in-depth analysis and evaluation of the ADA-EASD guidelines’ designation of GLP-1 receptor agonists as first-line therapy for diabetes. Professor Buse is the recipient of the 2019 Outstanding Achievement Award in Clinical Diabetes Research, conferred by the American Diabetes Association (ADA). This award honors clinical scientists who have made exceptional contributions to patient-oriented clinical research and have had a significant impact on the prevention and treatment of diabetes.

John B. Buse, MD, PhD (Image from the internet)
Professor Buse pointed out that type 2 diabetes is a progressive chronic disease, and patient factors must be considered during treatment, including patients' self-care, the occurrence of comorbidities, and the long-term financial burden of medication costs.
Article Review: Prior to the U.S. FDA’s approval of the GLP-1 receptor agonist exenatide in 2005, insulin was the only injectable medication for diabetes. Since then, the FDA has approved five additional GLP-1 receptor agonists: lixisenatide, albiglutide, dulaglutide, liraglutide, and semaglutide.
GLP-1 drugs are categorized into two types: animal-derived (exenatide and lixisenatide) and human-derived (liraglutide, semaglutide, dulaglutide, and albiglutide). Animal-derived agents (exenatide and lixisenatide) are short-acting, although exenatide has been formulated as a long-acting weekly preparation using microsphere sustained-release technology. Human-derived agents are long-acting; liraglutide is administered once daily, while albiglutide, dulaglutide, and semaglutide are injected once weekly.
For both physicians and patients, it is crucial to weigh the risks and benefits of each option and understand the considerations guiding the selection of a specific medication. The most significant hazard in diabetes treatment is the occurrence of hypoglycemia. Since the pharmacological action of GLP-1 receptor agonists is glucose-dependent, hypoglycemic events are rare. Another major advantage of GLP-1 receptor agonist therapy is its ability to promote satiety, helping patients achieve clinically meaningful weight loss. In contrast, insulin therapy typically tends to cause weight gain. Given the negative impact of obesity on glycemic control, this distinction between the two treatments is highly significant.
A vicious cycle ensues when drug-induced weight gain necessitates further intensification of diabetes therapy. Insulin-induced weight gain occurs not only during initial treatment but also accumulates over time as insulin doses are escalated. The weight-reducing effects of GLP-1 receptor agonists hold significant implications for the management of obesity-associated diabetes.
Cardiovascular disease is the most common complication in patients with type 2 diabetes and the leading cause of disease-related mortality. Therefore, there is an urgent need to develop medications that improve cardiovascular outcomes by controlling hyperglycemia and ameliorating metabolic syndrome. Since patients with type 2 diabetes require lifelong pharmacotherapy, GLP-1 receptor agonists with cardioprotective effects are expected to demonstrate superior adherence.(6)These characteristics of GLP-1 medications provide the theoretical basis for the ADA-EASD guideline recommending “GLP-1 receptor agonists, rather than insulin, as the first injectable therapy for most patients with type 2 diabetes.”
Professor Buse also pointed out that the discontinuation rate of GLP-1 is usually higher than that of basal insulin. To minimize the risk of gastrointestinal symptoms, patients should take the lowest dose of GLP-1 and titrate upward slowly. Therefore, high-efficacy, low-dose GLP-1 drugs will be popular among patients.
Furthermore, it should be taken into account that type 2 diabetes requires lifelong medication, and the cost of drugs directly affects patients' quality of life. If the manufacturing costs and sales prices of GLP-1 medications can be reduced, this will pave the way for their broader adoption as first-line therapies for diabetes treatment.
Human-Derived Long-Acting GLP-1 Receptor Agonists to Take Center Stage
To date, a total of six products (including those of human and animal origin) have been approved for marketing by the U.S. FDA and the European EMEA (Table 2).

Table 2. Six GLP-1 Drugs Approved for Marketing by the FDA and EMEA
Among them, exenatide (approved on October 21, 2010) and the extended-release formulation of exenatide (approved on May 18, 2018, for which 3SBio obtained sales distribution rights in China), liraglutide (approved on April 13, 2011), and dulaglutide (approved on February 26, 2019) have been marketed in China.
Notably, domestically developed innovative drugs with independent intellectual property rights, namely Benaglutide (Renhui Bio; human-derived, short-acting, administered via subcutaneous injection three times daily; approved on December 19, 2016) and Polyethylene Glycol Lozenatide (Hansoh Pharmaceutical; animal-derived, long-acting, administered via subcutaneous injection once weekly; approved on May 6, 2019), have also been launched sequentially. As of today, approximately 20 GLP-1 receptor agonists are registered with the Center for Drug Evaluation (CDE) in China and are currently in clinical development. The development of GLP-1 therapies has become a focal point in the field of diabetes.
At first glance, the landscape of GLP-1 medications appears crowded with numerous agents. However, a closer examination reveals that GLP-1 drugs can be primarily categorized along two dimensions: human-derived versus animal-derived, and short-acting versus long-acting. Human-derived, long-acting GLP-1 agents have not only demonstrated superior clinical efficacy but also significantly reduced the risk of cardiovascular mortality in patients with type 2 diabetes. In contrast, animal-derived (exendin-based) GLP-1 analogs share only approximately 50% amino acid sequence homology with human GLP-1. Besides local injection-site reactions, they may also elicit systemic immune responses. Numerous clinical studies, including a large-scale, international, multicenter trial in type 2 diabetes published in the New England Journal of Medicine, have shown that animal-derived GLP-1 receptor agonists (such as exenatide) do not confer cardiovascular benefits (2). Previous studies on type 2 diabetes medications raised concerns about the cardiovascular risks associated with glucose-lowering therapies, prompting the U.S. Food and Drug Administration (FDA) to mandate cardiovascular outcome trials for all new diabetes drugs.
Clearly, diabetes medications that lack cardiovascular benefits will not be adopted by physicians and patients.
Market data for GLP-1 drugs in 2018 show that the long-acting human GLP-1 analogs liraglutide and dulaglutide dominated, accounting for 85% of the entire GLP-1 drug market (Table 3). The terms “long-acting” and “short-acting” are relative: once-daily liraglutide is considered long-acting compared with twice-daily exenatide, but it is short-acting relative to the weekly formulations introduced later. The weekly formulation of dulaglutide has already surpassed once-daily liraglutide.
Indeed, clinical research data always guide the direction of the pharmaceutical market. Although exenatide microspheres, characterized by their long-acting weekly formulation and animal-derived origin, were launched earlier (2012) than dulaglutide (2014), their sales have remained sluggish and continued to decline.
Latest clinical research data show that dulaglutide and semaglutide have satisfactory cardiovascular benefits.(7,8)Based on these data, industry experts predict that over the next 3–5 years, the long-acting formulations dulaglutide (with $3.199 billion in sales in 2018) and semaglutide (with $297 million in sales in 2018) will each reach a market size of $5–10 billion in sales. Therefore, human-derived long-acting GLP-1 receptor agonists will lead the diabetes drug market.

Table 3. Sales of GLP-1 Receptor Agonists Over the Past 8 Years
Source: Armstrong, 2018 Diabetes Market Research Report: GLP-1 Receptor Agonists Stand Out
Analysis of the Structural Characteristics of Human-Derived Long-Acting GLP-1 Drugs
Public data from the Center for Drug Evaluation (CDE) indicate that there are four human-derived long-acting GLP-1 drugs either marketed or in clinical stages in China: Eli Lilly’s dulaglutide, Novo Nordisk’s semaglutide, Yinnuo Medicine’s supaglutide, and Hongyun Huaning’s GMA102 (Table 3). Dulaglutide injection has completed its clinical studies in China and was approved by the CDE for marketing in China on February 26, 2019.

Table3. Human-derived long-acting agents marketed or in clinical stages in ChinaGLP-1Medications, data fromCEDPublic information.
In summary, the common feature of these human-derived long-acting GLP-1 drugs is the use of genetic engineering techniques to fuse or bind GLP-1 analogs with the Fc fragment of human immunoglobulin G (IgG) or human albumin, thereby preventing rapid renal clearance and metabolic degradation in vivo and extending their half-life.
Dulaglutide is a fusion protein consisting of GLP-1 linked to the human IgG4-Fc fragment, formed by covalently connecting the N-terminus of a GLP-1 analog to a modified human IgG4 heavy chain Fc region via an artificial linker. This protein shares 90% homology with native human GLP-1 and has a molecular weight of 63 kDa.
Supalutide is a fusion protein consisting of GLP-1 linked to human IgG2-Fc, formed by covalently connecting the N-terminus of a GLP-1 analog to the Fc region of the human IgG2 heavy chain via the natural hinge region of immunoglobulin. This protein shares 97% homology with native human GLP-1 and has a molecular weight of 60 kDa.
GMA102 (monoclonal antibody injection) is a fusion protein consisting of GLP-1 linked to human IgG4. It is constructed by genetically engineering the covalent linkage of the N-terminus of a GLP-1 analog to the entire human IgG4 molecule via an artificial linker. This protein shares 97% homology with native human GLP-1 and has a molecular weight of 157 kDa.
Semaglutide is a modified GLP-1 analog linked to an 18-carbon fatty diacid side chain, which binds to human albumin to form a macromolecular complex. This molecule is engineered by genetically modifying the lysine at position 26 of the GLP-1 analog sequence into its derivative form (acylated with stearic diacid), followed by acylation via a spacer and a C-18 fatty diacid side chain, enabling binding to human albumin to form a macromolecular complex. This protein shares 94% homology with native human GLP-1 and has a molecular weight of 70.6 kDa.
A common feature of these human-derived long-acting GLP-1 drugs is the use of genetic engineering techniques to fuse or conjugate GLP-1 analogs with the Fc fragment of human immunoglobulin G (IgG) or human albumin, thereby preventing rapid renal clearance and metabolic degradation in vivo and extending their half-life.
Fusing the IgG-Fc domain with effector molecules (such as GLP-1) to confer in vivo stability; such Fc fusion protein drugs typically contain only the Fc portion of two heavy chains without IgG light chains, aiming to enhance thermal stress stability.(9). Both dulaglutide and supaglutide adhere to this design principle.
GMA102 is a fusion protein composed of a GLP-1 analog covalently linked to an entire human IgG4 molecule via an artificial linker. The rationale for retaining the IgG light chain can be understood as follows: the Fab fragment directs the fusion protein to target cells, enabling the GLP-1 moiety to bind to the GLP-1 receptor and activate downstream signaling pathways. In fact, GLP-1 itself exhibits strong affinity for the GLP-1 receptor and does not require any auxiliary mechanisms. Retaining the light chain in the IgG fusion protein not only compromises its thermal stability but also, due to its high molecular weight, typically necessitates higher drug concentrations to achieve the desired efficacy.
Human IgG has four subclasses. The Fc region can bind to soluble Fcγ receptors in the bloodstream, activating the effector functions of immune cells to destroy pathogens or kill target cells (such as tumor cells).(10). IgG1 and IgG3 exhibit high affinity for all Fcγ receptors (FcγRs); therefore, IgG1 or IgG3 is commonly selected for use in anti-inflammatory or antitumor therapies. In contrast, IgG4 binds to Fcγ receptors with lower affinity. Among all IgG subclasses, IgG2 has the lowest affinity for FcγRs, thereby offering a better safety profile.(11)。
Semaglutide, which is modified with a fatty diacid side chain to bind to human albumin and form a macromolecular complex, represents an ingenious design. Novo Nordisk is developing an oral formulation of semaglutide using the proprietary technology of Emisphere Technologies, Inc. (http://www.emisphere.com/) in the United States. This once-daily GLP-1 medication is currently undergoing Phase III clinical trials.
Injectable Formulations vs. Oral Formulations: Adherence and Potential Risks
In recent years, the American Diabetes Association has held dedicated sessions on injectable diabetes medications. It is evident that drugs administered via injection exhibit clear pharmacokinetic profiles, high bioavailability, and minimized negative risks of drug-drug interactions.
Although injection techniques have advanced to enable needle-free and painless administration, an innate fear of injections persists among the public. This is the primary reason patients desire oral formulations. As early as 1922, just one year after the discovery of insulin, Dr. Elliott P. Joslin attempted to use oral insulin preparations for the treatment of diabetes. Over the subsequent nearly 100 years, all efforts to develop oral insulin have ended in failure.
The lack of pharmacokinetic response is a major challenge in the development of oral insulin. In fact, patients with type 2 diabetes retain the ability to secrete insulin but lack an immediate response to postprandial blood glucose elevation, specifically referred to as the loss of the first-phase insulin secretion. Even if current technologies can overcome the “intestinal barrier,” ensuring that protein drugs are not degraded and pass intact through the intestinal wall into the bloodstream, patients still require at least 20 minutes after administration to achieve effective plasma drug concentrations.(12). This means that oral formulations cannot meet the body's immediate demand for insulin after meals. Furthermore, interactions between food (or other medications) and oral insulin pose potential risks to its therapeutic use.
Although researchers can ensure that study participants remain fasting and refrain from taking any other medications in “meticulously” designed clinical trials, the real-world scenario is different. Most patients with type 2 diabetes are elderly and often have comorbid metabolic disorders, including hypertension, hyperlipidemia, and coronary heart disease. These patients frequently take “a handful of medications simultaneously.” Drug-drug interactions and the potential adverse effects of food on drug efficacy are risks that cannot be ignored.
Some scholars have pointed out(10), the current literature on oral insulin research has been disappointing. All proposed trials have been early-stage feasibility and proof-of-concept studies with very small sample sizes. Although the conclusions of these proof-of-concept trials unanimously indicate that oral insulin is feasible, a closer examination of their designs and data reveals that there is still room for improvement.(13). In 2017, Novo Nordisk announced the termination of Phase III clinical trials for oral insulin, indicating that there is still a long way to go before oral insulin can be truly realized for clinical use.
Compared with insulin, GLP-1 possesses unique biological functions, and its glucose-lowering efficacy varies according to changes in patients’ blood glucose levels. Therefore, unlike insulin, the lack of a pharmacokinetic response is no longer a major challenge for GLP-1, even when administered orally. However, since patients with type 2 diabetes often require concurrent use of multiple medications, the primary challenges facing oral GLP-1 agents are the potential adverse effects of food intake and drug–drug interactions. The ultimate success of oral peptide or recombinant protein drugs requires extensive clinical studies as well as validation in real-world patient populations post-marketing. Furthermore, due to the very low bioavailability of oral formulations, doses typically need to be 10 to 100 times higher than those of injectable formulations. Manufacturing costs and pricing are also key determinants of whether these drugs will be adopted by U.S. insurers and European healthcare systems.(13)。
Summary:
As GLP-1 receptor agonists have been incorporated as first-line therapies for type 2 diabetes in the ADA-EASD guidelines, there will be substantial market demand for these agents. Long-acting human GLP-1 analogs exhibit glucose-lowering efficacy comparable to insulin, with a minimal risk of hypoglycemia. Furthermore, their benefits in weight reduction and cardiovascular protection enable patients on long-term GLP-1 therapy to achieve greater overall clinical gains.
Patients with type 2 diabetes require lifelong pharmacological treatment. Physicians must take into account patient-specific factors that significantly influence disease management, including self-care practices, the presence of comorbidities, and the long-term financial burden of medication costs.
Overall, the market demands high-quality, low-cost, and affordable diabetes medications with pleiotropic effects to improve patients’ metabolic syndrome and quality of life; long-acting human-derived GLP-1 agents will be the mainstay dominating the diabetes market in the future.
References:
1. J. Li, J. Zheng, S. Wang et al., Cardiovascular Benefits of Native GLP-1 and its Metabolites: An Indicator for GLP-1-Therapy Strategies. Front Physiol 8, 15 (2017).
2. R. R. Holman, M. A. Bethel, R. J. Mentz et al., Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med 377, 1228-1239 (2017).
3. https://professional.diabetes.org.
4. https://www.easd.org.
5. A. S. Alexopoulos, J. B. Buse, Initial injectable therapy in type 2 diabetes: key considerations when choosing between glucagon-like peptide 1 receptor agonists and insulin. Metabolism, (2019).
6. A. C. Sposito, O Berwanger, LSF de Carvalho et al., GLP-1RAs in type 2 diabetes: mechanisms that underlie cardiovascular effects and overview of cardiovascular outcome data. Cardiovasc Diabetol. 17(1), 157 (2018).
7. H. C. Gerstein, H. M. Colhoun, G. R. Dagenais et al., Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 394, 121-130 (2019).
8. H. C. Gerstein, H. M. Colhoun, G. R. Dagenais et al., Dulaglutide and renal outcomes in type 2 diabetes: an exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet 394, 131-138 (2019).
9. Y. Wang, Q. Lu, SK Wu et al., Characterization and comparison of disulfide linkages and scrambling patterns in therapeutic monoclonal antibodies: using LC-MS with electron transfer dissociation. Anal Chem. 2011 Apr 15;83(8):3133-40.
10. C. Rosales, Fcgamma Receptor Heterogeneity in Leukocyte Functional Responses. Front Immunol 8, 280 (2017).
11. P. M. Hogarth, G. A. Pietersz, Fc receptor-targeted therapies for the treatment of inflammation, cancer and beyond. Nat Rev Drug Discov 11, 311-331 (2012).
12. E. Zijlstra, L. Heinemann, L. Plum-Morschel, Oral insulin reloaded: a structured approach. J Diabetes Sci Technol 8, 458-465 (2014).
13. A. W. Michels, P. A. Gottlieb, Learning From Past Failures of Oral Insulin Trials. Diabetes 67, 1211-1215 (2018).