National Healthcare Security Administration: 24 Major Policies and Innovations Across Six Key Areas Within 18 Months of Establishment
Today marks the 552nd day since the establishment of the National Healthcare Security Administration.
At its inception, the National Healthcare Security Administration (NHSA) was entrusted with the mission of promoting the “three-medical-linkage” reform, shouldering high expectations in areas such as healthcare cost containment, fund supervision, and informatization construction—reflecting the determination of the CPC Central Committee and the State Council to deepen medical reform. A year and a half on, what kind of report card has the NHSA delivered?
According to official website data, by the end of 2018, the number of people enrolled in basic medical insurance accounted for more than 95% of China's total population, and the National Healthcare Security Administration managed a medical insurance fund exceeding RMB 2 trillion. As the most important payer in the healthcare sector, every move made by the National Healthcare Security Administration will have a profound impact on the industry.
From the major overhaul of the National Reimbursement Drug List to the centralized procurement of pharmaceuticals; from the development of healthcare security informatization and standardization to the introduction of internet-based medical payment models; from enabling cross-regional medical care settlement to controlling the expenditure of healthcare security funds—the achievements of the National Healthcare Security Administration have been undeniably impressive.
Over the past 552 days, the National Healthcare Security Administration has rolled out 24 major policies, undertaken 122 concrete actions, and pioneered innovations across six key areas. If healthcare is a stubborn ailment, the National Healthcare Security Administration is akin to an attending physician who has begun to operate.
In March 2018, the State Council launched a major institutional reform. The National Healthcare Security Administration (NHSA), like 24 other departments, was a newly established entity. While other departments unveiled their plaques in succession, the NHSA was the last to do so, on May 31.
This seems like some kind of metaphor:
The journey ahead is long; we must not give up, nor should we rush.
In early 2018, the State Council released the Plan for Deepening the Reform of Party and State Institutions. The National Healthcare Security Administration (NHSA), as the first independent national-level agency dedicated to healthcare security, came into public view. Together with the newly established National Health Commission, it assumed the external expectations for the coordinated reform of medical insurance, healthcare services, and pharmaceuticals—known as the “Three Medicals” linkage.
Healthcare reform has entered a critical phase; without implementing robust measures, it will be difficult to achieve further breakthroughs.
Under the previous system, management in this area was fragmented across four departments. The Ministry of Human Resources and Social Security administered health insurance for urban employees and urban residents; the National Health and Family Planning Commission oversaw the New Rural Cooperative Medical Scheme; the Ministry of Civil Affairs managed medical assistance programs; and the National Development and Reform Commission was responsible for regulating medical service and pharmaceutical prices. To achieve truly unified management, these functions must be integrated under a newly established administrative body. Such integration would not only ensure more effective management and regulation of health insurance funds but also leverage the power of a super-payer to drive down drug prices, promote information standardization, and catalyze broader industry transformation.
Only by centralizing power can we truly accomplish major undertakings.
On May 31, the National Healthcare Security Administration was officially inaugurated, and its leadership team, consisting of one director and three deputy directors, was fully established. Hu Jinglin, former Vice Minister of Finance, was appointed as the first Director, while Shi Zihai, Chen Jinfu, and Li Tao serve as the three Deputy Directors. Each member of the leadership team boasts an impressive background.
Hu Jinglin, the Director, holds a Ph.D. in Economics. He has authored or translated numerous works, including State-Owned Enterprise Reform and Approaches, Human Capital and Innovation in Corporate Systems, Financial Asset Valuation, and The U.S. Federal Government Budget. During his tenure as Vice Minister of Finance, he oversaw departments such as the General Office, the Department of Agriculture, and the Department of Finance.
Shi Zihai graduated from Beijing Normal University with a master’s degree in economics; Chen Jinfu also has a professional background in economics; Li Tao holds a Ph.D. in Medicine.
The National Healthcare Security Administration is positioned as the primary purchaser of medical services, facilitating its decisive role in shaping the development of the healthcare service system and the allocation of health resources. It comprises six departments and one office.
With the official inauguration of the National Healthcare Security Administration, the sword of reform has been unsheathed.
In July 2018, the hit film “Dying to Survive” resonated deeply with the public by addressing many pressing societal issues, earning an impressive rating of 9.0 on Douban upon its release.
In response to issues that have drawn strong public outcry, the National Healthcare Security Administration (NHSA) has taken action. In the same month, the NHSA’s official website published its first major policy since its establishment: the “Notice on Launching Provincial-Level Centralized Procurement of Anti-Cancer Drugs.”
The rationale behind this policy is that, with approximately RMB 2 trillion in medical insurance funds under its control, the National Healthcare Security Administration can naturally drive down terminal drug prices through centralized procurement and tax reductions, leveraging its substantial bargaining power.
With this as the opening, the National Healthcare Security Administration has frequently taken action.
According to statistics from VCBeat, the National Healthcare Security Administration has issued 24 major policies over a period of one and a half years, covering numerous areas such as the standardization of medical insurance information, internet healthcare, primary care, and supervision of medical insurance funds.
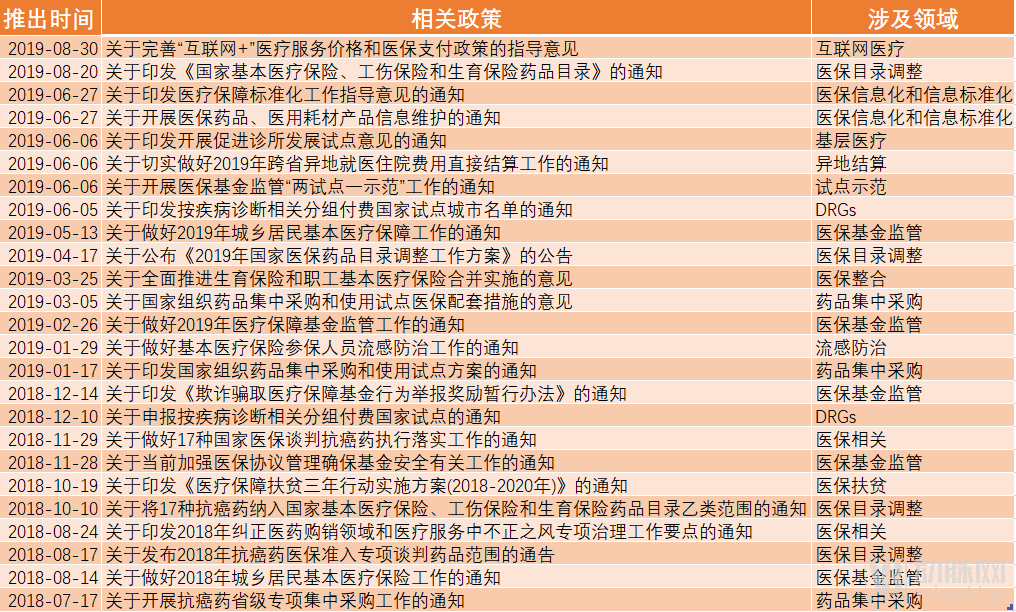
CountryPolicies Issued Since the Establishment of the National Healthcare Security Administration Source: Official Website of the National Healthcare Security Administration
As shown in the table, the work of the National Healthcare Security Administration primarily revolves around three areas: healthcare security fund management, adjustment of the healthcare security reimbursement list, and drug pricing.
These three aspects can be further broken down into: cracking down on insurance fraud and fraudulent claims, with the "Regulations on the Supervision of the Use of Medical Security Funds (Draft for Comments)" open for public consultation; relaunching adjustments to the medical insurance drug list and establishing a dynamic adjustment mechanism for the list; launching national pilot programs for Diagnosis-Related Groups (DRG) payment; promoting cross-regional medical care settlement, merging maternity insurance with basic medical insurance for urban employees, and advancing medical security poverty alleviation initiatives; piloting the "4+7" volume-based procurement program and initiating the third round of national reimbursement negotiations for anticancer drugs.
Each new policy rollout has detonated like a blockbuster bomb, triggering massive repercussions across the industry.
Companies across the healthcare industry chain are responding in diverse ways: some are proactively preparing for potential risks amid stability, others are hitting the emergency brakes, and still others are thriving. In short, all signs point to transformation.
Based on the policies launched by the National Healthcare Security Administration, we have selected and analyzed the six areas most profoundly impacted: supervision of medical insurance funds, adjustments to the medical insurance catalog, centralized drug procurement, informatization and information standardization of medical insurance, internet healthcare, and Diagnosis-Related Groups (DRGs).
1. Supervision of Medical Insurance Funds
Safeguarding fund security and maximizing fund efficacy are critical responsibilities of medical insurance administration, while strengthening the oversight of medical insurance funds constitutes a protracted endeavor requiring the collective participation of society at large.
Since September 2018, the National Healthcare Security Administration (NHSA), in conjunction with the National Health Commission and four other departments, has launched a nationwide “Special Campaign to Crack Down on Fraudulent Insurance Claims.” This marks the first national special campaign specifically targeting insurance fraud since the establishment of China’s medical insurance system. Following CCTV’s exposure of the “Shenyang Insurance Fraud Case,” the NHSA promptly conducted a “follow-up review” of self-inspections across various regions and published a national hotline for reporting fraudulent insurance claims.
In late November 2018, the National Healthcare Security Administration issued the “Notice on Strengthening the Management of Medical Insurance Agreements and Ensuring Fund Security,” requiring medical insurance administrative departments at all levels to exercise strict control and enhance supervision across all stages—including designated provider applications, agreement compliance, expense review, and performance evaluation—and to maintain a high-pressure stance and take decisive action against fraudulent activities aimed at embezzling medical insurance funds in violation of agreement terms.
In December, the National Healthcare Security Administration issued the Interim Measures for Rewarding Reports of Fraudulent Acquisition of Medical Security Funds, further strengthening efforts to combat insurance fraud. Verified whistleblowers may receive direct rewards of up to RMB 100,000.
In February 2019, the “Notice on Doing a Good Job in the Supervision and Administration of Medical Security Funds in 2019” was issued.
Through sustained efforts, a high-pressure stance against fraud and deception in health insurance has been established nationwide. This has led to the implementation of a series of working mechanisms, including clear accountability, streamlined channels for reporting and complaints, and strict, severe, and expedited handling of identified issues.
In terms of supervision over the basic medical insurance fund, the National Healthcare Security Administration reported the following achievements: By the end of 2018, a total of 272,000 designated medical and pharmaceutical institutions had been inspected nationwide, with 66,300 institutions penalized for breaches of contract, regulatory violations, or illegal activities. A total of 24,200 insured individuals suspected of fraudulent behavior were investigated; among them, 8,283 had their medical insurance card settlements suspended, 77 received administrative penalties, and 487 cases were referred to judicial authorities. A total of RMB 1.008 billion in misappropriated medical insurance funds was recovered.
2. Informatization and Information Standardization of Medical Insurance
China’s medical insurance information system has long suffered from three major problems: First, inconsistent standards and mutual non-recognition of data have prevented the formation of big data at the national or regional level, let alone enabling effective big data analytics. Second, fragmented systems and difficulties in data sharing persist, as nearly 400 pooling areas across China have independently developed their own information systems, which are dispersed among different departments such as Human Resources and Social Security, Civil Affairs, and Health Commission, resulting in poor interoperability. Third, regional closure and prominent “information silos” exist, with medical insurance data in each pooling area managed in a closed manner; each pooling area operates as an “information island,” where external access is blocked and internal data cannot be shared outward, leading to isolated and self-contained operations.
Establishing a nationally unified medical insurance information system has become a top priority for the National Healthcare Security Administration.
At the National Healthcare Security Work Conference, Hu Jinglin, Director of the National Healthcare Security Administration, proposed the “One-Two-Three-Four” objective for informatization development: to establish a nationally unified healthcare security information system; to build a two-tier healthcare security information platform at the national and provincial levels; to enhance the standardization, intelligence, and informatization of healthcare security across China; and to advance four major categories comprising 14 subsystems, namely public services, administration and management, intelligent monitoring, and macro-level decision-making.
This serves as a crucial guideline for advancing the informatization of medical insurance, and constitutes the overarching objective for the National Healthcare Security Administration’s subsequent initiatives.
The National Healthcare Security Administration established a leading group for cybersecurity and informatization just two months after its inauguration.
In March 2019, the National Healthcare Security Administration issued the Notice on Launching Pilot Programs for the Construction of Medical Security Information Systems, designating 16 provinces (including municipalities directly under the Central Government), such as Tianjin and Hebei, as pilot regions for the development of medical security information systems.
In June 2019, after ten months of preparation from scratch, the “Dynamic Maintenance of Medical Insurance Business Coding Standards” was launched for trial operation on the official website of the National Healthcare Security Administration (NHSA). This marked the formal implementation of the National Healthcare Security Information Platform. Among the 15 information business coding standards, four medical insurance information business codes—“Disease Diagnosis and Surgical Procedures,” “Pharmaceuticals,” “Medical Service Items,” and “Medical Consumables”—were the first to go live.

The Healthcare Informationization and Information Standardization Project Being Advanced by the National Healthcare Security Administration
In terms of the standardization of medical insurance, the "Guiding Opinions on Standardization Work for Medical Security" pointed out that by 2020, based on the construction of a unified national medical security information system, the implementation and use of 15 information business coding standards, including disease diagnosis and surgical operation codes, would be gradually achieved. During the "14th Five-Year Plan" period, a national list of medical security standards will be formed, and the research, formulation, trial application, and improvement of certain medical security standards will be initiated.
In terms of the informatization construction of medical insurance, the information platform construction project, which includes 14 subsystems, has completed the project approval and public bidding procurement processes, and has entered the substantive implementation phase.
3. Adjustment of the National Reimbursement Drug List
The National Reimbursement Drug List (NRDL) commands 80% of the sales market in public hospitals. For pharmaceutical companies, failure to secure NRDL inclusion means forfeiting the volume growth advantage driven by reimbursement coverage, thereby leaving them mired in fierce market competition. For consumers, the inclusion of more life-saving and emergency medications in the NRDL would help reduce out-of-pocket expenses.
In August last year, the National Healthcare Security Administration issued the “Notice on the Scope of Drugs for Special Negotiations on Medical Insurance Access for Anti-Cancer Drugs in 2018,” including 18 products from 12 companies in the scope of special negotiations for medical insurance access for anti-cancer drugs.
On August 20, 2019, a notice issued by the National Healthcare Security Administration on printing and distributing the “National List of Medicines Covered by Basic Medical Insurance, Work-Related Injury Insurance, and Maternity Insurance” triggered an earthquake in the industry.
In terms of the drugs added, this round of catalog adjustments introduced a total of 148 new items under the standard access category, including 47 Western medicines and 101 proprietary Chinese medicines. These additions cover national essential medicines, medications for chronic diseases, pediatric drugs, and treatments for major diseases such as cancer. Notably, key therapeutic areas like diabetes saw a significant number of new entries with more refined classification management, reflecting that this adjustment will further enhance the accessibility and rationality of medication use.
Based on the drugs removed, a total of 150 drug products were delisted in this adjustment. Approximately half of these were drugs whose approval numbers had been revoked by the national drug regulatory authorities, while the remainder primarily consisted of drugs with limited clinical value, evident potential for misuse, and availability of superior alternatives. Notably, all 20 drug products from the first batch of the Key Monitoring List for Rational Drug Use, which accounted for significant clinical usage volumes, were removed. This demonstrates the determination and intensity of the National Reimbursement Drug List (NRDL) adjustments, thereby creating greater space for drugs with high clinical value.
This major adjustment to the drug list marks the first comprehensive revision since the establishment of the National Healthcare Security Administration (NHSA) and represents a thorough review of the existing formulary items since the inaugural edition in 2000. It comes just two years after the previous major overhaul of the national reimbursement drug list.
From this perspective, the dynamic adjustment of the National Reimbursement Drug List (NRDL) is returning to a normalized routine. With the shortened adjustment cycle, the NRDL can facilitate more timely inclusion and exclusion of drugs, thereby revitalizing existing medical insurance resources, improving drug accessibility, and maximizing the efficacy of medical insurance funds.
The detailed rules of this notice stipulate that all regions must strictly implement the new version of the National Reimbursement Drug List (NRDL). Localities are prohibited from formulating their own drug lists or using alternative methods to add drugs to the list, and they may not independently adjust the restricted payment scope for drugs included in the list. For Class B drugs that were previously added to provincial drug catalogs in accordance with regulations, a phased phase-out process shall be completed within three years. During this phase-out period, each province shall prioritize the removal of drugs under national key monitoring from the reimbursement coverage.
At the media briefing held on the day of the release of the new National Reimbursement Drug List, it was confirmed that the updated list would officially take effect on January 1, 2020.
4. Centralized Drug Procurement
The purpose of centralized drug procurement is to explore and improve the mechanism for centralized drug procurement and the market-driven price formation mechanism for pharmaceuticals, reduce the medication cost burden on the public, standardize the order of drug distribution, and enhance medication safety for the public.
Since the establishment of the National Healthcare Security Administration (NHSA), which consolidates the powers of payment, supervision, and pricing, its first policy initiative focused on centralized drug procurement. The subsequent rollout of multiple related policies underscores the administration’s strong commitment to controlling pharmaceutical costs.
In November 2018, the National Healthcare Security Administration, in conjunction with the National Health Commission, the National Medical Products Administration, and other relevant departments, studied and drafted a pilot program. Following the principle of “state organization, alliance-based procurement, and platform-based operation,” a procurement alliance was formed comprising 11 cities: Beijing, Tianjin, Shanghai, Chongqing, Shenyang, Dalian, Xiamen, Guangzhou, Shenzhen, Chengdu, and Xi’an. This initiative aimed to restore the original intent of “linking volume with price and integrating tendering with procurement” by selecting drug varieties that had passed the consistency evaluation, consolidating the pharmaceutical demand of public medical institutions, and genuinely implementing volume-based procurement to reduce artificially inflated drug prices, all while ensuring quality and supply.
The National Healthcare Security Administration aims to explore the drug pricing formation mechanism through this initiative. Following the launch of the “4+7” pilot program, the 11 cities participating in the pilot achieved remarkable results. Among the 31 drugs included in the pilot, 25 were successfully selected for procurement. Compared with the lowest procurement prices for the same drugs in the pilot cities in 2017, the average price reduction for the selected drugs was 52%, with the maximum reduction reaching 96%.
On September 1, 2019, the Shanghai Sunshine Pharmaceutical Procurement Network released the “Alliance Region Drug Centralized Procurement Document,” extending procurement invitations to 25 provinces and autonomous regions across China. This signals that the model of centralized drug procurement is likely to be rolled out nationwide in the near future.
Lowering drug prices is the first step toward truly separating prescribing from dispensing, and the achievements of the “4+7” pilot program seem to herald the official onset of an era of healthcare reform led by medical insurance.
5.DRGs
DRG-based payment is a relatively advanced healthcare reimbursement model, currently adopted by countries such as the United States, Germany, and France. It involves comprehensive analysis of patients’ clinical conditions to assign them into specific diagnostic groups for bundled care, thereby standardizing treatment protocols and ensuring controllable healthcare costs.
From a historical perspective, since 2017, the National Health Commission has launched pilot programs for DRG-based payment and charging reforms in Sanming City (Fujian Province), Shenzhen City (Guangdong Province), Karamay City (Xinjiang Uygur Autonomous Region), and three medical institutions in Fujian Province. In January 2018, Sanming City, Fujian Province, officially implemented the DRG payment and charging system.
On December 20, 2018, the National Healthcare Security Administration issued the “Notice on Declaring National Pilot Programs for Diagnosis-Related Groups (DRG)-Based Payment,” deciding to organize and launch the declaration process for national DRG pilot programs. The objective is to formulate and refine nationally standardized DRG payment policies, procedures, and technical standards, thereby generating pilot outcomes that are referenceable, replicable, and scalable. In terms of pilot scope, each province may, in principle, recommend one or two cities (with municipalities directly under the Central Government participating as entire administrative units) as candidate cities for the national pilots.
In June 2019, the National Healthcare Security Administration, in conjunction with other ministries and commissions, officially issued the “Notice on Printing and Distributing the List of National Pilot Cities for Diagnosis-Related Group (DRG) Payment,” designating 30 cities as national pilot cities for DRG-based payment.
The document discloses that we will follow a three-step approach of “top-level design, simulation testing, and actual payment,” entering the simulation phase in 2020 and launching actual payments in 2021.
Regarding Diagnosis-Related Groups (DRGs), this year remains in the stage of top-level design. Ongoing initiatives include strengthening the information systems for DRG-based payment, standardizing the collection of medical insurance data for DRGs, and continuously refining medical insurance payment policies as well as administrative and operational management processes.
The strategic positioning and management models of healthcare institutions are undergoing profound transformation.
6. Internet Healthcare
Since the beginning of this year, with the gradual establishment of provincial-level regulatory platforms for internet medical services across various regions, the number of licensed internet hospitals has surged. After years of development, the industry has gradually formed a business model covering healthcare, pharmaceuticals, and insurance. However, this “insurance” component largely involves commercial insurance, as public medical insurance has yet to incorporate internet medical services into its coverage system. In contrast, for offline consultations, public medical insurance serves as a primary payment method. Consequently, there is a widespread consensus within the industry that the lack of integration with public medical insurance payments has significantly hindered the sector’s growth.
On August 30, 2019, the National Healthcare Security Administration released the “Guiding Opinions on Improving Pricing and Medical Insurance Reimbursement Policies for ‘Internet+’ Medical Services,” sending shockwaves through the industry once again.
The current policy guidance on medical insurance proposes that online and offline medical services shall be subject to equitable pricing and reimbursement policies. For “Internet+” medical services provided by designated medical institutions, if the service content is identical to that of offline medical services covered by medical insurance reimbursement and the charges adhere to the fee schedules of corresponding public medical institutions, such services shall be included in the scope of medical insurance reimbursement and paid accordingly upon completion of the requisite filing procedures.
As the internet is most likely to bring disruptive innovation to healthcare, the National Healthcare Security Administration has provided support from the payment side.
“Healthcare security funds are life-saving money for the people, by no means a free-for-all; (the healthcare security authorities) must act as the Monkey King, cracking down hard on evildoers.” Thus stated Hu Jinglin, Director of the National Healthcare Security Administration, at the National Healthcare Security Work Conference held on January 10, 2019.
Under his leadership, the National Healthcare Security Administration has delivered an impressive performance report in the year and a half since its establishment, rooting out many “malpractices and irregularities.” Nevertheless, the path of healthcare reform is arduous and long; the industry still faces numerous pain points, and more “malpractices and irregularities” are likely to emerge in the future.
But we believe we can root out the industry’s “demons and monsters”;
We believe that a Healthy China will inevitably come to pass.