DRG Series No.8: Why Did Germany Initiate the DRG Payment Reform?
Author: Dr. Liu Zhichen, Senior DRG Expert and Postdoctoral Fellow at Fudan University
Germany was the first country in the world to establish a social security system through legislation. Prior to 1993, it primarily adopted a fee-for-service payment model. Due to the lack of relevant regulatory measures, this led to a rapid increase in healthcare costs. To curb the rapidly rising healthcare expenditures, Germany initiated reforms in health insurance payment methods in 1993, implementing a per-unit-of-service payment system under a global budget framework. However, the per-unit-of-service payment approach incentivized healthcare providers to artificially split visits and prolong hospital stays, among other issues, which ultimately drove up healthcare costs and compromised the quality of care.
In 1984, Germany began exploring its own G-DRG payment system by drawing on the DRG payment models of the United States and Australia. In 1997, the German government commissioned the Hospital Association and the Health Insurance Associations to develop the G-DRG system. The 2000 German Statutory Health Insurance Reform Act mandated the adoption of the G-DRG system for reimbursing inpatient care costs starting January 1, 2003. Subsequently, the “Institute for the Hospital Remuneration System (DRG Research Center)” was established, jointly operated by the Social Health Insurance Association, the Private Health Insurance Association, and the Hospital Association.
Germany’s current payment system is hybrid, with distinct payment methods for outpatient and inpatient services. Reimbursement for outpatient services involves a two-step process: first, health insurance companies pay physicians’ associations using a capitation model; then, the physicians’ associations reimburse outpatient physicians based on a point-based fee-for-service system. Inpatient services are primarily reimbursed through Diagnosis-Related Groups (DRGs). Data show that approximately 97% of hospital discharges in 2010 were paid using the DRG-based system (Zhu Mingjun, 2012).
From the perspective of overall implementation effectiveness, Germany’s average healthcare quality is comparable to that of the United States, yet its expenditure is only half that of the U.S. (Thomas Mansky, 2016). In his presentation titled “The German Health Insurance System and the Application of DRGs” at the “First National Diagnosis-Related Groups (DRG) Forum” on December 9, 2016, Thomas Mansky from Technische Universität Berlin & Berlin University of Technology noted that, in terms of hospital mortality rates for coronary artery bypass grafting (CABG) surgery, the figure for California, USA, in 2010 was 2%, while Germany’s figure in 2011 was 2.1% (with raw data indicating a higher risk profile among Germany’s elderly population). However, from a cost perspective, Germany achieves healthcare service outcomes of equivalent quality at merely half the cost incurred in the United States.
Background of Germany's Introduction of DRG Payment Reform
1. Accelerating Pace of Population Aging
Data show that in 2011, Germany’s total population was 81.8 million, with the elderly population accounting for 20% of the total. Projections indicate that by 2060, the total population will decline to 71.7 million, while the proportion of elderly individuals (aged ≥65 years) will rise to 33%. The markedly accelerated pace of population aging has generated increased demand for healthcare services.
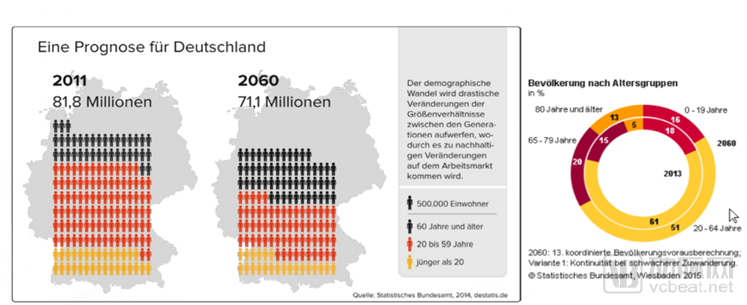
Figure 1. Population Projection for Germany
2. Rapid Surge in Demand for Healthcare Services
Since 2005, the demand for health services (i.e., the number of inpatient cases) has surged. Meanwhile, the supply of health services (the total number of full-time hospital employees) has also increased, but at a significantly slower rate than the growth in demand. In other words, the supply of health services fails to meet the ever-rising demand. Therefore, it is necessary to reform payment methods and adjust the healthcare structural system to better satisfy people’s needs for health services.
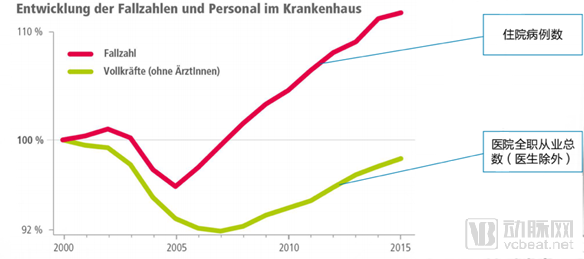
Figure 2 Development of Private Hospitals in Germany, 2000–2015
3. Limited and Unevenly Distributed Medical Service Resources
Medical resources are scarce and limited in quantity. Meanwhile, their distribution is uneven, with a disproportionate concentration in a small number of large cities, while smaller cities, despite being more numerous, have fewer medical resources, resulting in an irrational healthcare service system. Therefore, payment method reforms are needed to promote the rational allocation of health resources.
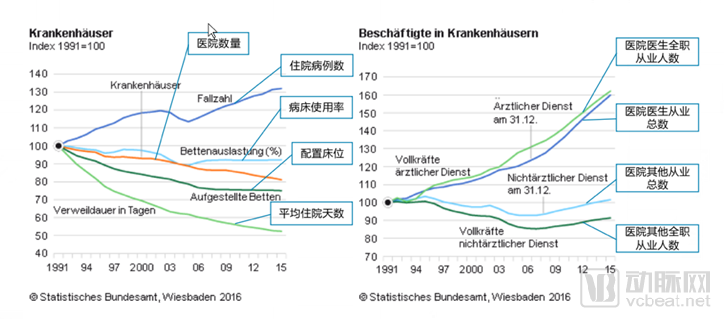
Figure 3 Statistics of Wiesbaden Federal Hospital and Medical Staff, 1991–2015
4. Rapid Growth in Medical Expenses
Since 2011, costs for inpatient care, contracted physician services, and pharmaceuticals have risen significantly. This cost escalation has compelled the government to consider payment method reforms as a means to achieve cost containment.
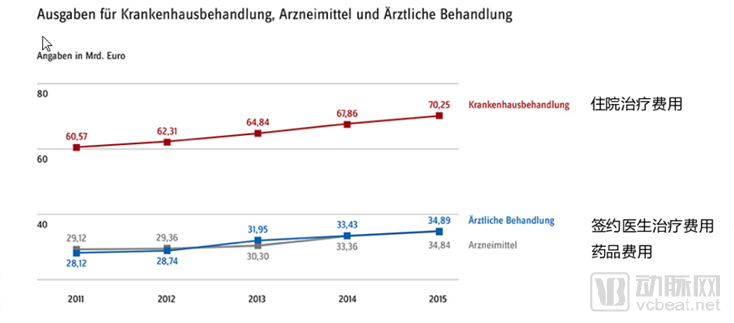
Figure 4. Expenditure on Federal Medical and Pharmaceutical Services in Wiesbaden, 2011–2015
5. Drawbacks of the Existing Payment System
Germany is a typical country with a social insurance model, where approximately 90% of insured individuals have their medical insurance costs covered by Social Health Insurance (SHI). Germany’s healthcare service system has developed based on a robust social health insurance framework, representing one of the world’s typical models for healthcare system development.
Prior to the reform of the Diagnosis-Related Groups (DRG) payment system, health insurance payments to hospitals in Germany were primarily made through methods such as per-diem payments for inpatient stays and fee-for-service for specific items, all under a global budget framework. This per-diem payment model had a strong capitation and budgetary nature, with single and fixed payment standards that reflected the principle of treating all patients equally. However, it also tended to incentivize physicians to prolong patients’ hospital stays and compelled some patients who could have been treated on an outpatient basis to undergo inpatient care. This directly led to a sharp rise in Germany’s total healthcare expenditures. By 2002, Germany’s total healthcare spending reached 11% of its GDP, indicating that the existing payment system was increasingly unable to meet patients’ needs. The German Federal Ministry of Health recognized that controlling costs required starting with reforms to the payment methods. Furthermore, regarding the content and outcomes of medical services, the mechanism determining healthcare costs under the existing payment system lacked transparency, medical quality information was not comparable internationally, and there were significant cost variations among hospitals. These issues urgently necessitated changes through payment system reform.
Therefore, drawing on the mature DRG payment systems of the United States and Australia while taking into account its own health insurance realities, Germany developed its G-DRG payment system, achieving notable results in healthcare cost management and becoming a successful model for subsequent DRG implementation efforts.
The Implementation Process of the German DRG Payment System
Implementing the DRG payment system is a large-scale government initiative that requires close collaboration among multiple sectors, including governmental decision-making bodies, legal departments, research centers, and professional associations. Since passing the statutory Health Insurance Reform Act in 2000, the German government has adopted a gradual approach to advance this reform in phases and steps. Based on the characteristics of DRG implementation in Germany, the process can be divided into four stages: the preparatory stage, the budget-neutral stage, the base rate integration stage, and the full implementation stage.
I. Preparation Phase: 2000–2003
1. Select the G-DRG System Suitable for Application in Germany
In 1997, the German Ministry of Health assigned the task of developing Diagnosis-Related Groups (DRGs) to the Hospital Federation, the Association of Private Health Insurance Companies, and the Statutory Health Insurance Funds, entrusting them with the development of a DRG system. The primary objective was to enhance the transparency of medical costs rather than to control them. Starting in 2000, the German government conducted in-depth research on the DRG systems of the United States and Australia, ultimately deciding to adopt the Australian AR-DRG system. This decision was based on the fact that this classification system was highly modern, offered sufficient transparency, provided realistic categorization, facilitated reimbursement, and closely aligned with Germany’s requirements for DRG implementation. Through code conversion and the establishment of specific coding rules, the G-DRG system tailored for application in Germany was researched and developed by November 2000.
2. Establishment of a DRG Research Center
In 2000, the German government enacted the statutory Health Insurance Reform Act, which mandated the introduction of a comprehensive, all-encompassing Diagnosis-Related Group (DRG) payment system for inpatient care effective January 1, 2003. Through legislation, the government resolved the legal status of DRG implementation and established the Institute for the Hospital Remuneration System (InEK), commonly referred to as the DRG Research Center. This institute was jointly founded by the National Association of Statutory Health Insurance Funds, the Association of Private Health Insurers, and the German Hospital Federation. The InEK operates under the direct leadership of the German Government’s Committee on Healthcare System Reform. In addition to developing rules for defining DRG case groups and related coding standards, the center’s primary responsibilities include the annual update and in-depth development of the G-DRG system through the establishment of disease and cost databases. These activities encompass adjusting the classification system, calculating relative cost weights, determining the base rate for DRGs, updating and managing add-on payments, deductions, and other additional fees, processing applications for new diagnostic and therapeutic technologies, and addressing proposals for structural dialogue.
3. Data Collection and Cost Estimation
From 2001 to 2002, the DRG Research Center (InEK) collected and analyzed data from 480,000 cases across 115 hospitals. Based on this data, the German Ministry of Health collaborated with InEK to develop Germany’s DRG cost weight analysis system.
One of the primary responsibilities of InEK is data collection and processing. Data collection mainly comprises three components: clinical data, cost data, and sample size. Clinical data are primarily used for diagnostic classification systems and procedure classification systems; they are collected and aggregated by InEK’s Data Center and then submitted to DIMDI for diagnostic and procedural coding. Cost data are mainly derived from domestic sources but require standardized cost accounting. Germany’s sample size is based on statistical data of patients visiting healthcare institutions nationwide, thereby ensuring high data authenticity and reliability. To safeguard patient privacy and prevent healthcare institutions from selecting patients based on InEK’s data, the data submitted by the Data Center to InEK must be anonymized. The basic DRG statistical data for hospitals (such as patient counts, length of stay, and case grouping) are ultimately published by the Federal Statistical Office.
In 2000, following the establishment of InEK, the research center assumed full responsibility for determining DRG cost standards based on the DRG grouping database and cost data. Germany established national-level specifications for hospital cost accounting, clearly defining cost types and allocation methods. The G-DRG system employs a bottom-up activity-based costing approach to determine case costs. Indirect cost centers are first allocated to direct cost centers; then, costs are allocated from the bottom up according to the actual volume of services provided during patient treatment to calculate the actual cost of each type of medical service per patient. Finally, the costs of various medical services for each patient are aggregated to obtain the total patient cost, thereby deriving the relative weight for each DRG group.
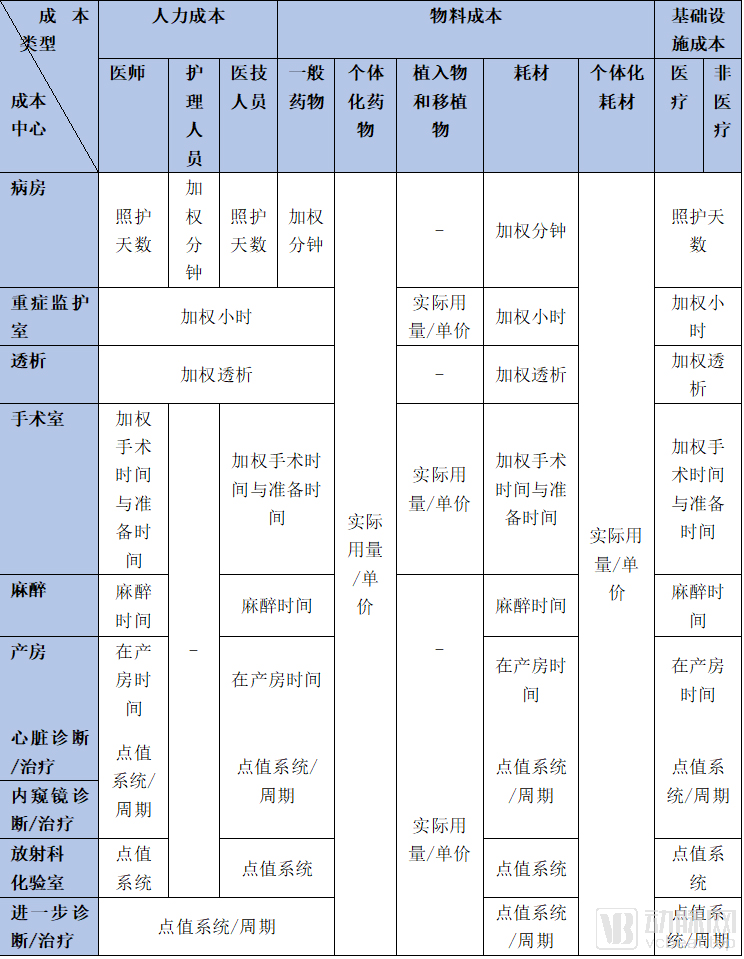
Based on the DRG grouping database and cost data, the research center was solely responsible for determining DRG cost standards and established a DRG cost accounting model. Key parameters in this model included DRG weights, average length of stay, and base payment rates. In 2003, Germany formulated cost standards for 664 DRG groups based on the DRG cost accounting model and relevant data. In 2007, adhering to the principle of consistent cost standards for the same medical conditions, Germany began implementing unified DRG cost accounting nationwide. The cost types, cost centers, and key cost drivers of G-DRG are shown in Table 1.
Table 1 Framework of the General Cost Accounting System for German G-DRG
4. Implement a unified disease coding and DRG coding system nationwide
DRG coding is the core of the DRG system. The Health Insurance Reform Act explicitly mandates the nationwide implementation of a unified DRG coding system in China. In Germany, the official DRG coding work is primarily carried out by the German Institute for Medical Documentation and Information (DIMDI). The first edition of the coding guidelines was published in May 2001 and has been updated annually since then.
Diagnostic codes are based on the World Health Organization’s International Classification of Diseases, Tenth Revision (ICD-10), modified to meet German requirements to form ICD-10-GM. Codes for surgeries and procedures use the Operation and Procedure Classification System (OPS), which was independently developed in Germany.
DRG coding is based on the ICD-10-GM disease classification system, combined with the OPS procedure coding system, to determine the Major Diagnostic Category (MDC). The MDC is then integrated with the Patient Clinical Complexity Level (PCCL) to generate different case mix groups, known as DRGs. The PCCL is stratified into five levels based on the presence and severity of complications and comorbidities: Level 0 indicates no complications or comorbidities, while Level 4 indicates very severe complications or comorbidities. The DRG Coding Guidelines are German coding directives designed to standardize documentation of diseases and treatments during hospitalization. The purpose of implementing these coding guidelines is to calculate medical costs, independent of the clinical disease types and medical history of the patients treated.
II. Pilot and Transition Phase: 2003–2009
In 2003, the German government introduced version 1.0 of the German G-DRG payment system, designating the period from 2003 to 2009 as a pilot and transitional phase to enable hospitals to establish operational systems adapted to the new healthcare framework.
In 2003, 750 hospitals were selected from over 2,000 hospitals nationwide as pilot institutions to voluntarily implement the DRG reimbursement system. In 2004, the G-DRG system was made mandatory across Germany. From 2005 to 2006, hospitals implemented budget plans based on DRG pricing. In 2007, all hospitals in Germany adopted a unified G-DRG fee reimbursement system. Additionally, since 2005, the German government has publicly released quality assessment reports for hospitals based on G-DRG payments. In 2007, adhering to the principle of consistent cost standards for the same disease categories, Germany began implementing nationwide uniform DRG cost accounting.
If classified according to the trend in changes of the base rate, the period from 2003 to 2009 can be further divided into two phases (as shown in Figure 5):
1. Budget-Neutral Phase: 2003–2005 (Different Base Rates Implemented by Each Hospital)
In 2003, hospitals voluntarily participated in the DRG system. In 2004, China mandated the nationwide adoption of the G-DRG system to pilot DRG-based reimbursement. A key characteristic of this phase was that each hospital had a different base rate, calculated based on its actual budget from the previous year. Due to the overall adoption of a budget-neutral strategy, this phase inevitably gave rise to so-called “DRG winners” and “DRG losers.”
2. Consolidation Phase: 2005–2009 (Statewide Standardization and Unification of Base Rates)
From 2005 to 2009, hospitals within each state had their own individual base rates, necessitating gradual adaptation through annual adjustments. In accordance with the government-mandated principle of converging toward a unified provincial-level rate within five years, this process aimed to reduce cost variations attributable to Diagnosis-Related Groups (DRGs) and mitigate risks for both the government and hospitals. By 2010, base rates for the same medical conditions were standardized across each state, completing the integration of base rates.
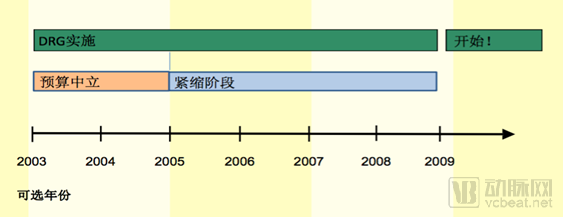
Figure 5 Phases of DRG Implementation in Germany, 2003–2009
The process of gradual unification of Germany’s base rates can be illustrated in the figure below:
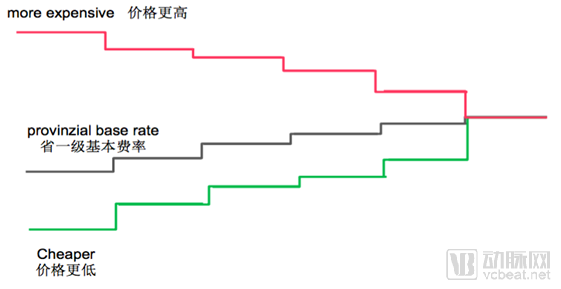
Figure 2. The Process of Convergence of German DRG Base Rates from 2003 to 2009
III. Full Implementation Phase: From 2010 to Present
Germany has fully implemented the Diagnosis-Related Groups (DRG) payment system in its inpatient sector, annually updates disease coding classifications, and explores various implementation models; furthermore, German sickness funds are primarily utilized for inpatient services.
In summary, after the introduction of DRGs, Germany spent nine years stabilizing and promoting their implementation, continuously addressing issues of selective treatment and quality concerns associated with case-based payment. The system gradually transitioned from hospital-specific proprietary rates based on individual medical records to unified benchmark rates at the state level. Beyond serving as a powerful tool for controlling hospital costs, DRGs were also regarded as a pricing mechanism that enhanced transparency in service scope and pricing, thereby incentivizing hospitals to improve their technical efficiency.
Over the past two decades, the number of hospital beds per capita in Germany has continuously declined, while the number of outpatient visits per capita has steadily increased and the average length of stay has decreased, a trend closely associated with the implementation of the Diagnosis-Related Groups (DRG) system.
References:
1. Zhu Mingjun. Payment System for Statutory Health Insurance in Germany [J]. China Medical Insurance, 2012(4):68-70.
2. Wang Qian. Specific Application of DRG in German Hospitals [R]. Speech delivered at the Second National DRGs Forum, July 2017
3. Wang Liuming, Lang Wen, Tao Hongbing. Advantages and Disadvantages of the German Diagnosis-Related Groups Payment System and Its Implications [J]. Medicine and Society, 2013, 26(11):44-47.
4. Chang Feng, Ji Meiyan, Lu Yun. Germany’s G-DRG Health Insurance Payment System and Its Implications for China [J]. Chinese Health Economics, 2016(6):92-96.
5. China Health Insurance Research Association. Health Insurance Systems in Germany and Sweden and the Application of DRGs [J]. China Health Insurance, 2010: 61–63.
6. Chang Feng, Ji Meiyan, Lu Yun. Germany’s G-DRG Health Insurance Payment System and Its Implications for China [J]. Chinese Health Economics, 2016(6):92-96.
7. Frank Heimig. Experience and Lessons from the Implementation of G-DRG in Germany: What Are the Key Factors for Success? [R]. Speech delivered at the China DRG Payment Conference, September 14, 2017.
8. Wang Li. Reform of the Diagnosis-Related Groups (DRG) Payment System in the United Kingdom and Germany [J]. Foreign Medical Sciences: Health Economics Fascicle, 2013, 30(120): 145-151.
9. Reinhard Busse,Alexander Geissler,Wilm Quentin,Miriam Wiley.Diagnosis Related Groups in Europe[M].European Observatory on Health Systems and Policies Series.2011.
10. Wang Liuming, Lang Wen, Tao Hongbing. Advantages and Disadvantages of the German Diagnosis-Related Groups Payment System and Its Implications [J]. Medicine and Society, 2013, 26(11):44-47.
11. Thomas Mansky. The German DRG Reimbursement System [R]. Speech delivered at the Beijing DRG Academic Exchange Conference, November 12, 2015.
Copyright Statement:
Most of the views presented in this article are based on Dr. Liu Zhichen’s personal postdoctoral research findings. The cited articles and viewpoints reflect those of their respective authors, obtained from publicly available sources. Any unauthorized reproduction, excerpting, copying, mirroring, or other forms of use are strictly prohibited.
Author Introduction:

Liu Zhichen
Chief Expert in the Healthcare Sector, Industrial Internet Product Center, China Unicom Group.
Postdoctoral Fellow, Postdoctoral Mobile Station in Public Administration at Fudan University and Postdoctoral Workstation of the Statistical Information Center of the National Health and Family Planning Commission. Senior Strategic Expert in the Greater Health Sector.
With nearly a decade of strategic consulting experience in the internet healthcare and broader health industry, I previously served as Director of Strategic Consulting and R&D Business Development at a leading Chinese listed IT solutions and services provider. In this role, I spearheaded the planning of numerous forward-looking innovative business models for the health sector. Notably, I accurately predicted that reforms in medical payment mechanisms, particularly the adoption of Diagnosis-Related Groups (DRG), would become a key initiative in deepening China’s healthcare reform during the 13th Five-Year Plan period. As the overall project lead, I participated in a pilot program for DRG-based medical insurance payment reform in a prefecture-level city in China. I assisted the municipal Medical Insurance Bureau in designing the top-level framework for the citywide DRG payment system reform and facilitated the implementation of supporting information technology systems.